 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 43, No. 2, April-June, 2006, pp. 54-59 Review Article Is interferon-α and retinoic acid combination along with radiation superior to chemo-radiation in the treatment of advanced carcinoma of cervix? Basu P, Biswas J*, Mandal R, Choudhury P** Departments of Gynecologic Oncology, *Medical Oncology and **Radiation Oncology, Chittaranjan
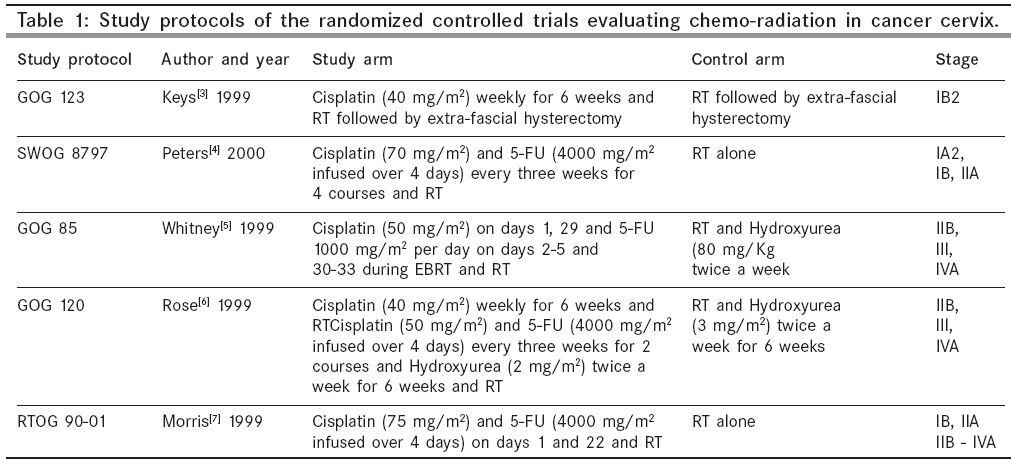
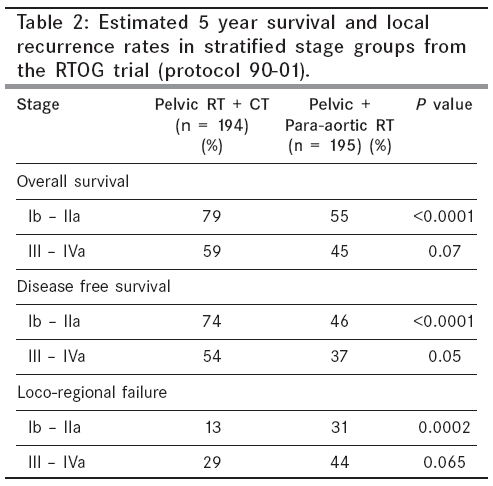
National Cancer Institute, 37, S. P. Mukherjee Road, Kolkata, India Code Number: cn06009 Abstract Locally advanced cervical cancers comprise a large majority of the gynecologic cancers in India and other developing countries. Concurrent chemo-radiation has improved the survival of high risk stage I and stage II cervical cancers. There is no evidence that the same survival benefit has been achieved with chemo-radiation in stage III and stage IV disease. Interferon-α and Retinoic acid have synergistic anti-proliferative activity. In combination with radiation, they substantially enhance the sensitivity of the squamous carcinoma cells to radiation. Based on these observations from the in vitro studies, a few clinical trials have evaluated the combination of interferon-α and Retinoic acid, concomitant with radiation, to treat cervical cancers. The results from these early trials were encouraging and the combination had minimal toxicities. However, till date, no phase III randomized controlled trial has been done to evaluate this therapeutic modality.Keywords: Cervical cancer, chemo-radiation, interferon alpha, retinoic acid, radiation, immunotherapy. Cancer of uterine cervix is the second most common cancer among women worldwide and is the cause of largest number of cancer-related deaths among women in the developing countries. Cervical cancer is the commonest cancer among the Indian women (126,000 new cases, 71,000 deaths around the year 2000), accounting for a quarter of the global burden of cervical cancer (471,000 new cases and 233,000 deaths).[1],[2] As there is no population-based screening program in India, 70-80% of the cervical cancer patients are diagnosed at advanced stages (Stage III and IV), with very poor long term survival. The situation is similar in many countries of Latin America and Sub-Saharan Africa, where cervical cancer is a major public health problem. The success of Cisplatin-based chemotherapy, administered concomitant with radiation to treat cervical cancer, gave rise to a lot of initial optimism. Unfortunately, the therapeutic benefit is not as evident in advanced stage disease (stages III and IV), as in early stages (stage I bulky disease or stage II). Retinoic acid (RA) and interferon alpha (IFN-α) have excellent synergistic cytotoxic effect against squamous cell carcinoma cell lines, specially when combined with radiation. Based on this observation, retinoic acid and interferon alpha have been tried by various investigators, with or without radiation, against squamous cell carcinoma of cervix. The current review sums up the results of the trials done so far and tries to explore the potentials of this combination in treating locally advanced cancer of uterine cervix. Concomitant Chemo-Radiation in Advanced Cervical Cancer In the year 1999, the National Cancer Institute (NCI) of United States of America recommended Cisplatin-based chemotherapy concurrent with radiation, as the standard treatment protocol for cervical cancer patients, who require radiation. This recommendation was based on the results of five randomized trials, that claimed a significant survival advantage of radiation and concurrent Cisplatin-based chemotherapy, over radiation therapy alone.[3],[4],[5],[6],-[7] The protocols of these trials are described briefly in [Table - 1]. The GOG 123 protocol recruited patients with only bulky (greater than 4 cm) stage IB disease and the SWOG 8797 protocol recruited patients with only stage I-IIA disease with poor prognostic factors (metastatic disease in the pelvic lymph nodes, parametrial invasion, positive surgical margin).[3],[4] No inference regarding the effectiveness of chemo-radiation in advanced cervical cancer, can be drawn from these studies. The other three trials recruited patients with stage III and stage IVA disease. Of these, two trials (Protocols GOG 85 and GOG 120) did not publish the response rates or survival rates stratified by stages.[5],[6] The survival advantage of chemo-radiation in stages III and IV cannot be conclusively inferred from these studies, because of the relatively less number of patients at these stages. Another criticism against both these studies, is that the control arm received Hydroxyurea along with radiation and there was no radiation alone control arm. The myelo-suppressive effect of Hydroxyurea and the consequential anemia, can reduce the effectiveness of radiation in the control arms, thus falsely inflating the success rate in the study arms. Only the trial based on RTOG Protocol 90-01 published the survival rates stratified by the stages of disease [Table - 2].[7] They observed that concomitant CT RT significantly improved the disease free and over all survival, in the early stage of the disease (Stage Ib and IIa with tumor diameter at least 5 cm or pelvic node involvement). The benefit was not significant in the patients suffering from stage III or IV disease. All the trials based on which the NCI alert was sounded, excluded patients with para-aortic lymph node metastasis, determined surgico-pathologically or radiologically, or by both methods. As a result, these trials cannot draw a logical conclusion about the effectiveness of chemo-radiation in improving the survival of the patients with para-aortic node metastasis. Nearly 30% of the patients with stage III/IV disease have para-aortic node metastasis. A Canadian phase III randomized trial on cervical cancer patients compared radiation alone to Cisplatin (40 mg/m2 on days 1, 8, 15, 22 and 29), given concurrently with radiation.[8] Randomization was stratified by stages. The study was less selective in their choice of patients, as they excluded those with para-aortic node metastasis detected by CT scan alone and not by staging laparotomy. The study did not find any advantage of chemo-radiation over radiation alone, in terms of either pelvic control or survival. Considering the short comings of some of the studies and the inconsistent results, a meta-analysis of 19 trials comparing concurrent chemo-radiation with radiation alone, observed that the over-all benefit demonstrated in the chemo-radiation group should be cautiously extrapolated to the women with locally advanced tumors.[9] Higher incidence of acute toxicities, specially leucopenia and gastrointestinal side-effects, is a major concern in the patients receiving chemo-radiation. The afore-mentioned meta-analysis observed a significantly increased occurrence of both the toxicities in the chemo-radiation group, in all the studies. Therapy- induced anemia can be a major rate- limiting factor in treating the cervical cancer patients in the developing countries, who already have poor nutritional status and low hemoglobin reserve. Kirwan et al in a systematic review of the randomized trials comparing concomitant CT-RT with radiation alone, observed significantly higher Grade 3 and 4 haematologic toxicities and gastrointestinal complications, in the CT-RT group.[10] Many of the centers in India and other developing countries, find it difficult to administer chemotherapy, due to acute shortage of hospital beds, even on day care basis. Clearly, there is a pressing need for a suitable and effective combination therapy for advanced cervical cancer that has less toxicity and can be administered on out-patient basis. Anti-neoplastic and Radiation Sensitizing effects of IFN-α and RA Interferons are secreted after stimulation of cells with virus. They bind specifically to receptors on the target-cell membrane and trigger the synthesis of proteins that can inhibit viral replication. Interferon-α is a type 1 interferon, that can directly affect immune function by stimulating B-cell (antibody-producing cell) proliferation and natural-killer-cell activity and also by enhancing major histocompatibility complex (MHC) class I expression. IFN-α has shown significant effect in cell differentiation and apoptosis, in some hematological and solid tumors. It can induce the expression of cyclin-dependent kinase inhibitor p21 that has anti-proliferative effect.[11] IFN-α can potentiate the cytotoxicity of ionizing irradiation in various malignant cells in vitro, such as human colon carcinoma cell lines, human bronchogenic carcinoma cell lines and cervical cancer cell lines. The available experimental evidence supports the hypothesis, that the radio-sensitizing effect of IFN-α, might be due to a blockage in the G2-M transition of the cell cycle.[12] However, the detailed mechanisms are yet to be elucidated. Retinoids are natural or synthetic derivatives of vitamin A. They are prototypical differentiation agents, which have a critical role in normal cellular function. They modulate differentiation, inhibit growth and induce programmed cell death in a wide variety of cancer cell lines.[13] Retinoids inhibit cervical cancer cell growth through mechanisms involving repression of activator protein 1 (AP1) transcription factor activity, down-regulation of epidermal growth factor expression and augmentation of Fas/Fas ligand mediated apoptosis. Retinoic acid, together with the cyclin-dependent kinase inhibitors p16, p21 and p27, can alter proliferation of malignant cells.[14] Vitamin A and its derivates are also known to enhance the sensitivity of experimental animal tumors, as well as human SCC cell lines (of head and neck and cervical cancer origin), to radiation.[15],[16] Synergism between IFN-α and RA to Control Cell Proliferation Experimental data prove the interaction between Retinoic acid and IFN-α in the regulation of cell proliferation. Combination of Interferon and Retinoic acid leads to an additive antiproliferative effect on the cell growth of cervical cancer, in vitro .[17] In an early stage model of cervical carcinoma, Retinoic acid was found to reduce dysplastic differentiation and IFN-α to induce apoptosis.[18] This observation lead the authors to propose, that the combined treatment can be effective in early cervical lesions. Similar synergistic effects of these two drugs in the inhibition of HPV, induced transformation of squamous cells in vitro and were demonstrated on cervical cancer cell lines by a series of experimental studies. The combination increases the level of Interferon regulatory factor 1 (IRF-1) causing growth arrest. Retinoic acid has been demonstrated to enhance the expression of Interferon-induced proteins. In vitro data reported by Frey et al have revealed, that the combination of 13-cis-Retinoic Acid (13cRA) with IFN-α, exerts substantially more antiproliferative activity than either retinoids or IFN-α alone.[19] In an in vitro study, treatment of various human squamous cell carcinomas (cell lines derived from head and neck cancers, cervical cancers) with all trans retinoic acid (ATRA), 13-cis-RA, or IFN-α, in concentrations achievable in clinical settings, resulted in a pronounced inhibition of clonogenic activity.[20] As compared to the single-drug treatment, combined treatment with ATRA and IFN-α, or with 13cRA and IFN-α, was found to be more effective. Synergism between IFN-α and RA to Enhance Radiation Sensitivity Both IFN and retinoids have been demonstrated to potentiate the radiation toxicity on the human squamous carcinoma cells and there is a synergistic action between the two agents.[20] The combined treatment with retinoids and IFN-α leads to a pronounced radiosensitization of all cell lines, including cervical and oral carcinoma cell lines. The mechanism of potentiation of the radiobiologic effect of radiation by interferon and retinoic acid, was demonstrated by Dunst et al , in an interesting phase II prospective study involving stage IIB-IVA cervical cancer patients.[21] One group of patients received standard radiation therapy and the other group received cis-Retinoic acid combined with Interferon α-2b, along with radiation. All the patients had polarographic measurement of tumour tissue pO 2 prior to radiation, after 20Gy of radiation and after completion of radiation. They observed a more pronounced increase of the median pO 2 in tumour tissues of patients treated by combination therapy, compared to those treated by radiation alone. Median enhancement of pO 2 was from 7.0 mm Hg to 40.9 mm Hg, in the combined treatment arm. The enhancement was significantly less (5.7 mm Hg to 14.7 mm Hg) in the control arm. Higher tissue oxygenation in the tumour tissue of the combination treatment group, can explain the higher rate of complete response in that group. Clinical Trials Evaluating IFN-α, RA and RT Combination in Cervical Cancer Till date, few clinical trials have evaluated the combination of interferon alpha, retinoic acid and radiation, that has demonstrated such significant antiproliferative, immunomodulatory and antineoplastic activities, in in-vitro and in-vivo models. Except one, all the clinical trials have reported, that the combination of retinoic acid and interferon is effective against cervical cancer. The clinical trial that did not observe any benefit, used the combination on recurrent cervical cancer patients, most of whom have already received radiation that rendered them refractory to the drugs.[22] Of note, recurrent cervical cancer after radiation is refractory to chemotherapy also. Some of the studies have used the two drugs without radiation, in previously untreated cervical cancer cases. In one such phase II trial, 13-cis-Retinoic acid plus Interferon α-2a, were used to treat 32 locally advanced cervical cancers.[22] They were treated for at least 2 months with oral 13-cis-Retinoic acid (1 mg/kg/day) and Interferon α-2a (subcutaneously, 6 million units daily). Even without radiation, 50% major response was observed, that included 4 complete responses. Toxicity to treatment was manageable. A Mexican prospective trial treated 17 consecutive patients of advanced stage cervical cancer (stages III and IV), with a combination of radiation and Interferon α-2b, at a dose of 5x10 6 IU/M 2 3 times a week, for 6 weeks.[23] They observed a complete response rate in 64%, of whom 24% were alive after 10 years of follow up. Another pilot study in Korea observed significantly better response rate in locally advanced cervical cancers treated by radiation, interferon and retinoic acid combination, as compared to historic controls treated by chemo-radiation.[24] They observed 33% complete remission in the trial arm and 17% complete remission in the controls. Only one phase III randomized trial compared the efficacy of radiation and Interferon α-2b against radiation alone, in the primary treatment of stage IIIB cervical cancer.[25] The radiation protocols in both the arms were similar. The patients in the interferon arm, received Interferon α-2b (3 x 10 6 IU/M 2) subcutaneously daily, starting from day 1 of radiation. At a median follow up for all patients of 17 months, the disease free survival in the Interferon group was 50% (18/36) and in the radiation alone group was 39.5% (18/38). The number of cases in this study was too low to comment on the statistical significance of their observation. Toxicities of IFN-α, RA and Radiation Combination Almost all the clinical trials involving interferon and retinoic acid have observed minimal toxicities, that can be ascribed to this combination. The commonest side effect of the drugs is fever, that can be observed in upto 60% of the patients, followed by fatigue and flu-like syndrome. All the side effects can be easily managed by simple medications. A prospective trial evaluated the toxicities of 13-cis-retinoic acid and IFN-α, used concomitant with radiation to treat different squamous cell cancers, including that of uterine cervix (n = 27).27 Only 3 patients (2 out of 13 cervical cancer patients) had WHO grade-3 hematological toxicity (leucopenia only), that lead to interruption of trial medication. None of the patients required blood transfusion or antibiotics and none had grade-4 hematologic toxicities. Among the non-hematologic toxicities, fatigue and flu like syndrome were the most common and occurred in 35% of all cases. However, the fever associated with Interferon injection was always transient and could be easily controlled with paracetamol, 500 mg, given orally, thrice a day. Of the 13 cervical cancer patients, 5 had diarrhoea (grade-1: 3, grade-2: 1, grade-3: 1). Other gastrointestinal toxicities were mild and transient. Dry skin desquamation was observed in 10 out of 13 cervical cancer patients and all of them were either grade-1 or grade-2 in severity. Some of the studies have observed myelo-toxicities and proctitis with interferon/retinoic acid and radiation. Rarely, the toxicities are more than grade 2, requiring interruption of treatment or transfusion. Conclusion The survival advantage of chemo-radiation in early stage cervical cancer, is not equally applicable to stage III or IV disease. The biggest challenge to the oncology centers in India, is to offer a reasonable survival to the huge number of stage III and IV cervical cancer cases registered with them every year. There is clearly a need for a therapeutic modality alternative to chemo-radiation, that can improve the survival of these patients. In this setting, immunotherapy combined with radiation represents the obvious treatment of choice for cervical cancer, a cancer that is initiated due a deficiency in the normal immune mechanisms of the body. The encouraging data from the in vitro studies and the early clinical trials, justify the need for a phase III randomized controlled study to establish the effectiveness of the combination of retinoic acid and Interferon alpha, along with radiation in the management of locally advanced cancer of uterine cervix. This is particularly relevant in the underdeveloped countries, because of the far advanced stage of the disease at diagnosis. Fewer toxicities and no requirement of hospitalization, are the other attractive features of the IFN-α, RA and radiation combination therapy. However, the early and late normal tissue reactions of such a combined treatment have to be investigated further. The cost of the drugs is still a limiting factor in resource poor countries. There is a possibility that with the innovations in large scale production systems (e.g., from transgenic plants), the cost of Interferons will come down within affordable range[26]. References
Copyright 2006 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn06009t1.jpg] [cn06009t2.jpg] |
| |||||||||

{kind=link}
{kind=link}