 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
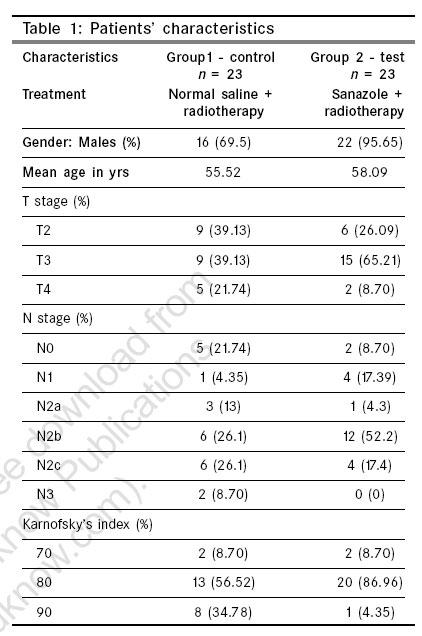
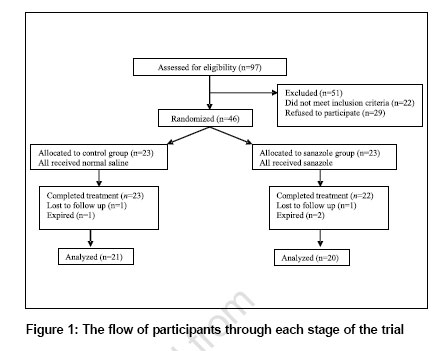
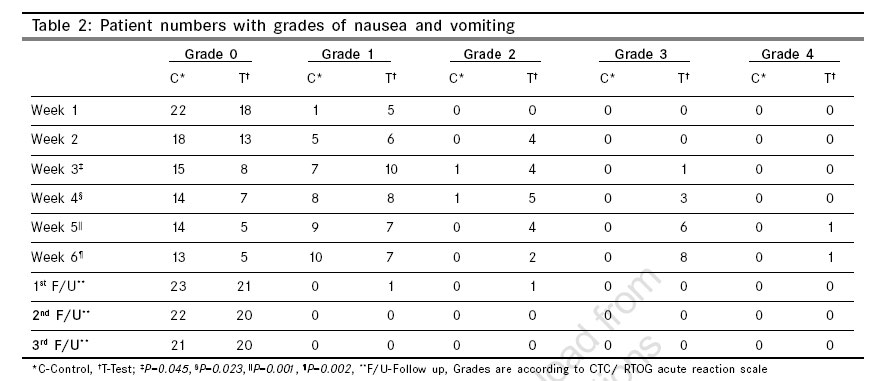
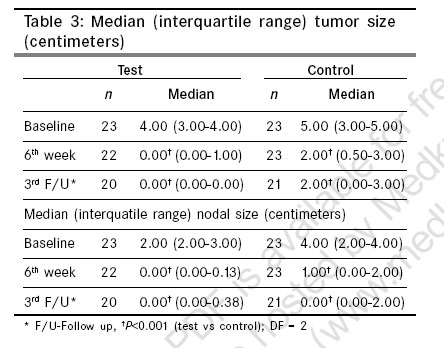
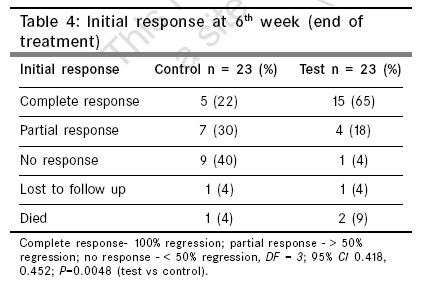
Indian Journal of Cancer, Vol. 43, No. 4, October-December, 2006, pp. 151-155 Original Article Safety and radiosensitizing efficacy of sanazole (AK 2123) in oropharyngeal cancers: Randomized controlled double blind clinical trial Ullal SD, Shenoy KK, Pai MRSM, Chowta MN, Adiga SMN, Dinesh M, Kamath A, Kotian MS, Pai DK Department of Pharmacology, Kasturba Medical College, Mangalore, Manipal Code Number: cn06024 Abstract Oropharynx is an important site of cancer in India. Global comparison indicates higher incidences in India. Radiotherapy remains an important treatment modality. Efforts to improve loco-regional treatment and prolong survival are areas of focus. Radiosensitizers in hypoxic tumors have shown promise.Aim: To study the safety and radiosensitizing efficacy of sanazole in oropharyngeal squamous cell carcinoma (stage T2-4, N0-3, M0) as phase-II double blind controlled trial in patients treated with conventional radiotherapy. SETTINGS AND DESIGN: Single institutional, randomized, double-blind, placebo-controlled trial. MATERIALS AND METHODS: Group 1 (control; n =23) received normal saline infusion, group 2 (test; n =23) received sanazole biweekly 1.25 g intravenous infusion 15 minutes before radiotherapy. Surrogate end points of efficacy were tumor and nodal size; safety parameters were mucositis, salivary and skin reactions, dysphagia, vomiting, dysgeusia and neurological deficit. Investigators blinded to the trial evaluated patients, weekly during treatment for six weeks and thereafter monthly for three months. STATISTICAL METHODS: Non-parametric, Friedman's, Chi square, Mann-Whitney U tests. RESULTS: In the test, 15 (65%) patients had complete response, five (22%) partial/no response, two (9%) died, one (4%) lost to follow up. In the control, five (22%) patients had complete response, 16 (70%) partial/no response, one (4%) died, one (4%) lost to follow up. Short-term loco-regional response was better in the test ( DF = 3 , 95% Confidence Interval 0.418, 0.452, P=0.0048 ). In the test group significant vomiting and one case of grade 3 neurological deficit was observed. CONCLUSION: The study validates the usefulness of sanazole for initial loco-regional control in oropharyngeal cancers. Keywords: Radiosensitization, oropharyngeal cancer, sanazole Patient records over the past five years in our hospital indicate that head and neck cancer accounts for around 40-43% of all cancers. Population based cancer registries under National Cancer Registry Program of Indian Council of Medical Research and global comparisons indicate similarly, that these malignancies are among the most important sites of cancer in India.[1] In the above context the onus of improving loco-regional treatment remains with us. Radiotherapy as a therapeutic modality in oropharyngeal cancers has its advantages and disadvantages; the main disadvantages being acute and late effects on normal tissue, limiting the dose of radiation and reduced radiation sensitivity induced by hypoxia in the tumor cells that have outgrown their vasculature.[2] Hence radiosensitizers would sensitize the resistant hypoxic tumor cells and make them more susceptible to radiotherapy. However, radiosensitizers have had a checkered history. Phase III studies on the first generation radiosensitizer, misonidazole showed promise but it did not gain popularity due to its toxicity,[3] while second generation etanidazole produced no global benefit on long term survival.[4],[5] A third generation radiosensitizer, sanazole, a nitrotriazole, has demonstrated to possess radiosensitizing potential, in-vitro, in-vivo[6] and in phase II clinical trials.[7] The present study was undertaken to evaluate the safety and radiosensitizing efficacy of sanazole in patients of oropharyngeal squamous cell carcinoma (stage T2-4, N0-3, M0) as phase II double blind, controlled clinical trial, to expand the limited existing data on sanazole. Materials and Methods Patients between the ages of 18 and 70 years with histologically proven, untreated oropharyngeal squamous cell carcinoma, any grade, stage T2-4, N0-3, M0, at a tertiary care hospital were considered for inclusion in this study. Eligibility criteria included Karnofsky's Index (KI) of 70% and above, adequate renal and liver functions, WBC > 4000/ mm 3, platelets > 100,000/ mm 3 and hemoglobin > 10 g/dl. Work up of the patients also included chest roentgenography. Patients with tumors of the nasopharynx and hypopharynx were excluded as these sites are inaccessible for objective documentation of measurable disease by inspection and/or palpation. Patients with central nervous system disease or peripheral neuropathy were excluded. Similarly patients with systemic illnesses such as hypertension, diabetes, severe allergic disease or previous treatment with radiation were not included in the study as these patients are predisposed to neuropathy either due to disease or drugs which may lead to additive toxicity and influence the true incidence of neuropathy expected with sanazole. Oropharyngeal sites included posterior one third of tongue, tonsils, soft palate, vallecula and posterior oropharyngeal wall. Patients were transfused when necessary to maintain a hemoglobin level of at least 10 g/dl throughout radiotherapy. Approval from the institutional ethics committee was obtained prior to starting the study. Written informed consent was obtained from the patient in the vernacular language after the nature of the procedure was explained. Patients were randomized based on a computer generated randomization list (drawn up by the statistician) and allotted to two groups, Group 1 (control n =23) and Group 2 (test n =23) as shown in [Table - 1]. This randomization list was concealed till the end of the study from the investigators involved in the clinical assessment of the patients. The study was double blind and the code broken only at the end of the study. An investigator not involved in the clinical assessment of the patients, allocated the next available number on the randomization list on entry into the trial and also administered the drug, either placebo or sanazole. Patients in the sanazole group received sanazole in the dose of 1.25 g (in 50 ml of normal saline) as an intravenous infusion over ten minutes, 15 minutes before radiotherapy, twice a week. A total dose of 12.5 g sanazole was administered. Patients in the control group received 50ml of normal saline administered as an intravenous infusion in an identical manner to patients in the test group. Thus blinding of patients was achieved. All patients received external beam radiation therapy on telecobalt machine at 80 cm source-skin distance with appropriate technique of bilateral parallel opposed portals. Fractionated doses were given daily, Monday through Friday in equal doses of 2 Gy for a total of 10 Gy per week. A total of 60 Gy in 30 fractions were delivered over a period of 6 weeks. The target volumes included the entire palpable tumor with 2 cm margins and entire neck. Spinal cord was shielded after 46 Gy. The trial was conducted over a period of three years. The efficacy parameters were tumor and nodal response. The primary end points for efficacy were complete regression of both primary tumor and nodes. The tumor and nodal size was clinically assessed in millimeters before treatment, every week for six weeks during treatment and every month for three months during follow up. The overall efficacy was assessed and recorded as complete response- no clinically detectable disease or 100% regression; partial response - > 50% regression and no response - < 50% regression. The secondary end point was the assessment of safety (drug toxicity). The parameters for safety included mucositis, salivary reactions, skin reactions, dysphagia, nausea and vomiting, dysgeusia and neurological status. These were graded according to CTC/RTOG acute reaction scale. Hematological parameters namely WBC count, platelet count and hemoglobin were assessed before and after the study to rule out hematological toxicity with sanazole. Patients who developed signs of neuropathy underwent an evaluation by a neurologist. Clinical investigators blind to treatment protocol assessed the patients for efficacy and safety parameters. A sample size of 46 was required to detect a difference between the two treatment groups of 32% with a type I error of 0.05 and a power of 80%. Data of efficacy parameters are expressed as median and interquartile range (IQR). IQR is the interval between the values of the upper quartile and the lower quartile for that group. Upper quartile of a group is the value above which 25% of the observations fall. Lower quartile is the value below which 25% of the observations fall. Since the data was not normally distributed the results were compared using the non-parametric test (Friedman's test) for statistical significance. Data of safety parameters were analyzed using Mann-Whitney U test. Results A total of 46 patients were included, 23 in each group. The study was conducted between August 2000 and June 2003. A monthly follow up of a minimum of three months was conducted for each patient. The flow of participants through each stage of the trial is shown in [Figure - 1]. [Table - 1] describes the characteristics of the patient population. As shown in [Table - 2], the test group had significantly more nausea and vomiting in the third ( P =0.045), fourth ( P =0.023), fifth ( P =0.001) and sixth ( P =0.002) weeks of treatment using the Mann- Whitney U test at 5% level of significance. But there were no differences during follow up. One patient in the test group developed grade 3 sensory and motor deficits in the left lower limb, one month after completion of radiotherapy. Other safety parameters which included mucositis, salivary reactions, skin reactions and dysgeusia were similar in both the groups. The hematological parameters (total WBC count, platelet count and hemoglobin) showed no significant difference between the two groups and were maintained through out the study at or above the levels given in the inclusion criteria. [Table - 3] shows the median tumor and nodal size at the baseline, 6th week and 3rd follow up in the test and control groups. As the data was not normally distributed non parametric test was used. The Friedman's test was used for comparison over the time periods. There is a statistically significant difference in the median tumor size ( P< 0.001 ) - the test group faring better than the control at 6th week and at 3rd follow up. A statistically significant difference was also observed in the median nodal size between the two groups over the time points of assessment both at 6th week and 3rd follow up ( P< 0.001 ). [Table - 4] shows the initial response, taking into account both tumor and nodal size at six weeks (end of treatment). There were 15 (65%) patients with complete response in the test group as against only five (22%) in the control. There is a statistically significant difference {degree of freedom ( DF )=3; 95% confidence interval ( CI ) 0.418, 0.452; P =0.0048} according to Chi square test, between the two groups. It is apparent that the initial loco-regional control was better in the test group. Discussion The proliferative capacity of human cells can be destroyed by ionizing radiation and the rate of killing by radiation is approximately three times higher in the presence of oxygen than under hypoxic conditions. Solid tumors often have zones of necrosis and consequently are likely to contain hypoxic yet viable cells. Hypoxia may also be due to discontinuous flow of blood, resulting in cells alternating between hypoxic and euoxic states.[8] The radioresistant tumor cells that survive treatment can become oxygenated and lead to a recurrence of the disease. Over the last three-four decades, procedures designed to increase the radiosensitivity of hypoxic cells within tumors include blood transfusions to anemic patients, use of hyperbaric oxygen chambers, high-linear-energy-transfer radiations and radiosensitizing drugs including first generation metronidazole and misonidazole, second generation pimonidazole and etanidazole and third generation nimorazole and sanazole. Misonidazole, a nitroaromatic drug, though superior to metronidazole as a radiosensitizer was limited by neurological toxicity of varying severity.[3] Etanidazole, a misonidazole analog is better tolerated than misonidazole, but in randomized studies did not afford any global benefit for patients of head and neck cancers.[4],[5] In vitro and in vivo studies comparing nimorazole and sanazole have shown sanazole to be a more efficacious radiosensitizer and a suitable candidate for further clinical trials.[9] Sanazole, a triazole derivative of nitroimidazole, is a slightly less efficient hypoxic radiosensitizer compared to misonidazole,[6] but is considered to be less neurotoxic[7],[10] by virtue of being less lipophilic than misonidazole. The ability of sanazole to produce nitric oxide has been proposed as a probable mechanism for its antitumor and immunomodulating properties.[11] Pharmacokinetic studies of sanazole have shown a two-three times higher plasma concentration with quick elimination after intravenous administration than after oral administration.[12] Hence we chose to administer the drug intravenously. The proportion of acute and intermittent hypoxic cells changes dynamically over time and is determined by diffusion range and perfusion of the tumor. Therefore a hypoxic cell sensitizer should be present in high concentrations during radiation. Hence sanazole was given just 15 minutes before radiotherapy to enable the drug to be present in the tumor at the time of irradiation. This further justifies an intravenous administration. In the present study, in patients in the sanazole group, the primary end points of complete tumor and nodal regression was better at six weeks {DF = 3; 95% CI 0.418, 0.452; P=0.0048} [Table - 4]. Sanazole was also efficacious in improving tumor and nodal control over three months after treatment completion [Table - 3]. As [Table - 2] shows, the secondary end points of safety (mucositis, salivary reactions, skin reactions and dysgeusia) showed no significant difference between the two groups, except nausea and vomiting which were significantly higher in the sanazole group, from the third to the sixth week ( P = 0.045, 0.023, 0.001, 0.002 for the third, fourth, fifth and sixth weeks respectively). Severe vomiting however, responded to therapy with standard injectable anti-emetics. One patient in the sanazole group developed both sensory and motor neurological deficit (grade 3) in the left lower limb, one month after the completion of radiotherapy. The patient improved with glucocorticoid therapy, over a period of three weeks. However, grade 1 neurological motor deficit (but no sensory deficit) persisted but the patient was able to walk without support. Though it is not statistically significant, this adverse effect cannot be ignored. There was no significant difference in the hematological laboratory findings before and after treatment in the two groups. Conclusions The present study focused on the use of sanazole in oropharyngeal cancers which is one of the commonest tumors in India and is known to have a hypoxic core. In studies conducted earlier, using sanazole as radiosensitizer combined with conventional fractionated radiation in head and neck and cervical cancers, the results have been encouraging.[7],[13],[14] Our study endorses the positive results of these previous studies in their totality, inspite of having a reasonably larger sample size and a design of a systematic double blind randomized controlled trial (hence eliminating bias) as against the earlier study on oropharyngeal cancers (Huilgol et al ),[7] which was an open study with a limited number of patients. Hence we conclude that in patients of oropharyngeal cancers treated with conventional fractionated radiation, sanazole is effective in improving short-term loco-regional control, however its ability to improve long-term disease free period and survival is yet to be confirmed. Further studies with larger sample sizes and longer follow up periods are needed to validate the finding obtained from several studies on the efficacy of sanazole as an effective radiosensitizer in locoregional control of solid tumors and on long term survival.References
Copyright 2006 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn06024t4.jpg] [cn06024f1.jpg] [cn06024t1.jpg] [cn06024t2.jpg] [cn06024t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}