 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
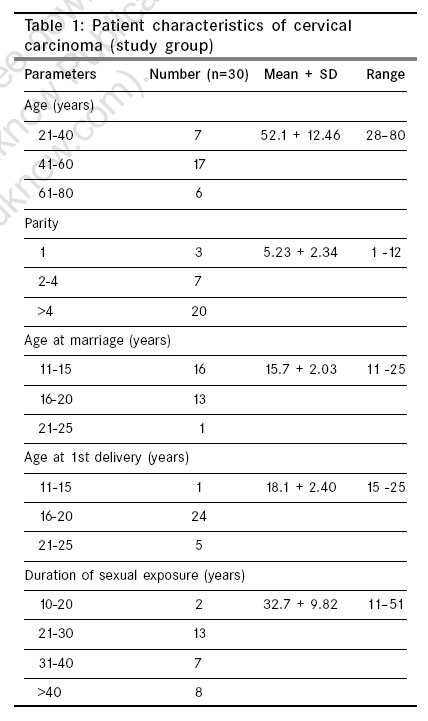
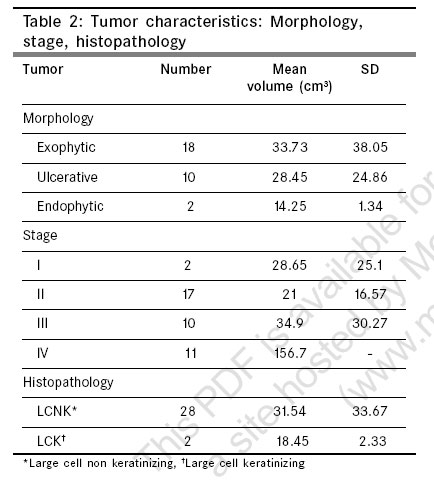
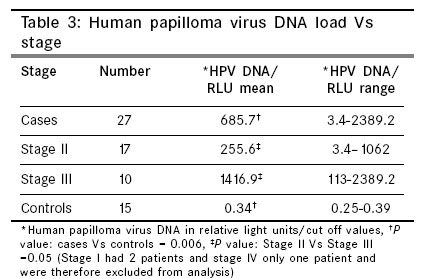
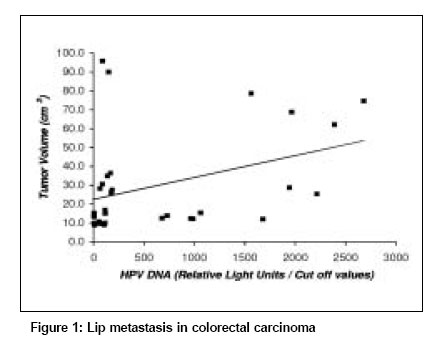
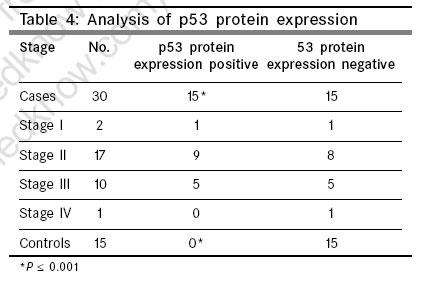
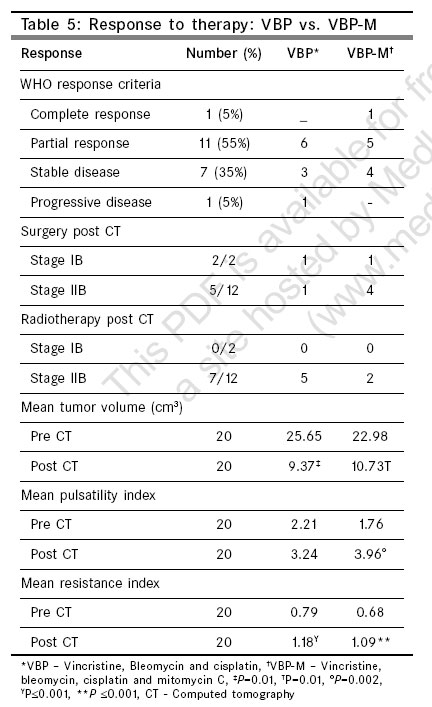
Indian Journal of Cancer, Vol. 43, No. 4, October-December, 2006, pp. 156-162 Original Article High-risk human papillomavirus, tumor suppressor protein p53 and mitomycin-C in invasive squamous cell carcinoma cervix Rajaram S, Gupta G, Agarwal S, Goel N, Singh KC Department of Obstetrics and Gynaecology, Guru Teg Bahadur Hospital and University College of Medical Sciences, Delhi - 110 095 Code Number: cn06025 Abstract Background: Clinical data relating to human papillomavirus (HPV) infection and p53 status in cervical cancer has been sparse and confusing.Aim: To evaluate high-risk HPV and expression of tumor suppressor protein p53 in squamous cell carcinoma of cervix and to assess response to mitomycin-C in neo-adjuvant chemotherapy. Setting and Design : Teaching College Hospital; Gynecologic Oncology Unit and Department of Pathology. Prospective, randomized. Materials and Methods : Expression of p53 protein was assessed, using immunohistochemistry with mouse monoclonal antibody in 30 consecutive patients undergoing radical hysterectomy or admitted for neo-adjuvant chemotherapy. Human papillomavirus DNA (HPV DNA) was assessed using hybrid capture II technology. Patients eligible for chemotherapy were randomized into vincristine, bleomycin and cisplatin (VBP) group and VBP with mitomycin C group. Statistical Analysis : Chi-square test, one-way ANOVA, Pearson's correlation; Mann-Whitney, McNemar and Fischer's exact tests were used for statistical analysis. Results : All patients with cancer cervix were positive for high-risk HPV DNA having relative light units/cut off values ranging from 3.4-2389.21 ( P value = 0.006). High viral load of high risk HPV DNA was seen in advanced stages ( P = 0.05) and an association of viral load with tumor volume was also seen (r=0.361, P =0.05). Analysis of p53 protein in cervical carcinoma patient showed expression in 50% of cancer specimens ( P value < 0.001). McNemar's and Fischer's exact test showed no change in p53 status post-chemotherapy; however 66% of stage II B patients in VBP-M group became operable. Conclusion : High-risk HPV was universally present in all cases of cancer cervix and viral load was associated with stage and tumor volume while p53 protein was expressed in 50% of cases suggesting deregulation. More studies using mitomycin-C in cervical cancer treatment protocols are needed. Keywords: p53 protein, human papillomavirus, squamous cell carcinoma cervix, mitomycin-C Epidemiological evidence suggests that human papillomavirus (HPV) infection, most commonly type 16 and 18 are detected in more than 95% of cases of cervical carcinoma.[1],[2] Evidence from in-vitro cell transformation experiments indicates that DNA from certain high-risk HPV types are capable of transforming epithelial cell lines in co-operation with activated cellular oncogenes, thus mimicking multi-step carcinogenesis.[3] Potential mechanism for cervical carcinogenesis could be viral integration or mutations in HPV E2 such that E2 controlled regulation of E6/E7 protein expression is lost. The inappropriate expression of E6/E7 in a population of cells produces lesions characterized by less orderly squamous maturation and basal like cell overgrowth. These viral proteins (E6/E7) functionally interfere with cell cycle control by inactivating tumor suppressor gene p53 and the retinoblastoma (Rb) protein.[4],[5] The E-6 protein forms a complex with a cellular protein termed E6 associated protein (E6-AP) and E6/E6-AP complex causes degradation of p53 through ubiquitine dependent proteolytic pathway. Cells expressing high risk HPV E6 are therefore deprived of p53 tumor suppressor activities. The role of p53 is thought to be in preventing replication of damaged DNA and loss of this function is associated with genetic instability and accumulation of potentially oncogenic mutations.[4],[6] In instances where cervical cancer does not contain HPV, p53 mutations have been found whereas degradation of p53, the functional equivalent of mutation is found in HPV infected cancers.[7] There are very few Indian studies addressing high risk HPV and p53 in carcinoma cervix. Nagpal et al observed that 69.1% of cervical cancer patients were HPV positive, among which the presence of HPV16, 18 and 16/18 co-infection was 40.9, 8.2 and 13.6%, respectively. They concluded that women with Arg/Arg homozygous allele in the codon-72 of p53 are more prone to infection by HPV16/18.[8] Hence other HPV types and or other etiological factors may be implicated in cervical carcinogenesis. HPV assay by HC II is a cost-effective method for screening for carcinoma cervix and detects 13 different types of high risk HPV types namely 16/18/31/33/35/39/45/51/52/56/58/59/68.[9] In previously published studies, we used neoadjuvant chemotherapy (vincristine, bleomycin and cisplatin) in patients with locally advanced (stage IB2) and advanced cancers because the waiting period for definitive radiotherapy/chemoradiation was six weeks or longer. These studies showed that 28 percent of stage II B patients became operable and patients with advanced cancers showed quality of life improvement with disappearance of foul smelling discharge and bleeding in roughly 85% of patients and no patient showed a progression of disease.[10],[11] The regime was cycled weekly and was non-myelosuppressive. This is of great benefit in developing countries given the high cancer burden and paucity of radiotherapy units. Recent evidence has shown that mitomycin C a cytotoxic chemotherapeutic agent, used in clinical practice is known to induce and stabilize p53 by causing DNA damage in the form of DNA cross-links as well as a variety of DNA monoadducts in cervical cancer cell lines.[12],[13],[14] Thus the potential of utilizing p53 in clinical applications needs to be explored. Other studies have suggested that treatment with genotoxic agents, such as mitomycin C and cisplatin, leads to strong repression of viral E6/E7 oncogene expression in HPV16-and HPV18-positive cervical carcinoma cell lines. HPV-positive cancer cells can exhibit intact cellular responses to genotoxic stress, which may involve p53-dependent and -independent biochemical pathways. The ability of HPV-positive cancer cells to induce apoptotic cell death in response to DNA damage could provide a molecular explanation for the therapeutic effects of genotoxic agents in the treatment of cervical cancer.[15] With this background the primary aim of the study was to evaluate high risk HPV and p53 protein in relation to carcinoma cervix in Indian women and the secondary aim was to assess response to therapy with addition of mitomycin C to a previously used vincristine, bleomycin, cisplatin regime. Materials and Methods Thirty consecutive patients of squamous cell carcinoma cervix (Stage IB2 and above) admitted for Radical Wertheim's hysterectomy or neo-adjuvant chemotherapy were inducted for the study, for a duration of one year, from April 2002 to March 2003. The hospital ethical committee approved the study and an informed consent was obtained from all patients. Thirty patients with proven squamous cell carcinoma of cervix (FIGO Stage I-IV) were assessed for expression of p53 protein in cervical biopsy specimens using immunohistochemistry before therapy. Sample size of thirty was selected as various studies showed a p53 expression of between 10-30%.[3],[16] To demonstrate 20±15% positivity with 95% confidence a sample size of 27 is required. HPV DNA types were assessed in all patients pre-therapy from cervical brush specimens using hybrid capture II technology (Digene; Digene corporation USA). Fifteen cervical biopsies from hysterectomy specimens done for benign indications (DUB, fibroid) served as controls for p53. Fifteen low-risk, sexually active individuals in the reproductive age group comprised controls for HPV analyses. Low-risk women included those with stable monogamous relationships, marriage and childbirth after 18 years of age, parity 2 or below. All controls had a normal Pap smear. Expression of tumor suppressor protein p53 was assessed again one week after completion of neo-adjuvant chemotherapy. HPV-DNA was not assessed post chemotherapy. Of the 30 patients enrolled 20 qualified for neo-adjuvant chemotherapy and were randomized to two groups by computer generated random numbers. Inclusion criteria included those with histopathologically proven, chemotherapy naοve patients, less than 60 years of age with adequate hematological, renal and hepatic functions, with locally advanced and advanced cancer (Stage II B onwards). Patients (n=10) in the VBP group were given three courses of multi-agent neo-adjuvant chemotherapy in the form of vincristine 1 mg/m 2sub and cisplatin 50 mg/m 2 on day 1, bleomycin 15 mg/m 2 on day one and day two on a weekly basis.[10],[11] A standard antiemetic regime consisting of metoclopramide and dexamethasone was administered. Each subsequent course of chemotherapy was administered only when the hematological, renal and hepatic functions were within normal limits. In the VBP-M group patients received mitomycin C (10 mg/m 2) on day one and day 21 in addition to VBP regime. Response was assessed one week after the last course of chemotherapy objectively using standard response criteria (WHO).[17] Complete response: no evidence of disease, partial response (PR) more than 50% of reduction of tumor, progressive disease (PD) 25% or greater increase in size and stable disease (SD) when neither PR nor PD criteria are met. Tumor volume was calculated by measuring dimensions in three planes by transvaginal sonography. Intratumoral blood flow was assessed by transvaginal Doppler sonography pre and post- chemotherapy. Resistance index and pulsatility indices were calculated using standard formulas. All Stage I B2 patients underwent Radical Wertheim's surgery one week after completion of chemotherapy. Operability in stage II B was assessed and patients whose parametrial extension disappeared also underwent radical surgery. All the others were sent for definitive radiotherapy. Assessment of p53 Assessment of p53 protein was done using immunohistochemical staining with anti-human mouse monoclonal antibody (Dakopatts, Denmark) by the method described by Dimitrakakis.[16] Using a semiquantitative technique the percentage of tumor cells staining positive were assessed. Tumors with nuclear p53 positivity in at least 10% of the neoplastic cells were regarded as positive (+), indicating the presence of abnormal p53 protein. Normal or Wild p53 is not stained because of short half-life. With each batch of slides, a negative control was set by replacing mouse-antihuman p53 with buffer. HPV DNA analysis Analysis of HPV DNA was done using hybrid capture II technology in 30 patients of cancer cervix. The Digene HPV test utilizes chemiluminescence for the qualitative detection of five low-risk and 13 types of high-risk HPV DNA in cervical specimens.[9] Light emitted, is measured as relative light units (RLUs) on a luminometer. The RLU of specimen was compared with RLU of positive calibrator and a ratio of> 1 was considered was to be positive. The specimens that were positive for combined probe cocktail were reconfirmed with high risk type HPV DNA probe. Statistical analysis p53 protein expression and HPV DNA analysis between cervical cancer cases and controls was calculated by Chi-square test. HPV viral load was analyzed in relation to the stage of the disease using one-way ANOVA. Association between viral load and tumor volume was evaluated using Pearson's correlation. Mann-Whitney test was performed to study the relation between HPV DNA and p53 status. p53 status pre and post-chemotherapy was tested using McNemar test and comparison of p53, post chemotherapy, between VBP and VBP-M was done using Fischer's exact test. P = 0.05 was regarded as statistically significant. Results Patient and tumor characteristics Patient profile is shown in [Table - 1]. All patients were married and denied a history of sexual promiscuity in self or partner. No patient had ever had cervical screening in her lifetime. 86.7% of patients and partners never used a contraceptive method and the rest i.e., 13.3% underwent tubal ligation. Nine out of the 30 patients were chronic smokers and continued smoking until they reported to hospital. Majority of patients (n=28) presented with advanced stage disease and only 2 patients belonged to stage IB2. Patients with an exophytic tumor had the greatest tumor volume. Histopathologically most tumors were large cell non-keratinizing (n=28) with a mean tumor volume of 31.54 cm 3 [Table - 2]. Analysis of high-risk HPV/viral load All cases of invasive squamous cell carcinoma were positive for high-risk HPV DNA having RLU cut off values ranging from 3.4-2389.2 while all controls were negative for both low-risk and high-risk HPV DNA with RLU < 1. ( P =0.006). [Table - 3] shows HPV DNA viral load in Stage II and III carcinoma cervix. High risk HPV load between stage II and III patients was statistically significant ( P =0.05). There were only two and one patient in stage I and IV respectively and these were excluded from analysis. Tumor volume was correlated with human papilloma viral load using Pearson's correlation. A correlation coefficient of r = 0.361, P =0.05 was obtained indicating an association between the tumor volume and HPV viral load [Figure - 1]. Analysis of p53 protein In cancer cervix cases, 15 out of 30 (50%) expressed p53 protein while all controls (n=15), were negative for p53 protein. ( P < 0.001, Chi-square test). p53 expression in various stages of cancer cervix is shown in [Table - 4]. 50% of specimens were positive and 50% negative for p53 protein in all stages. When p53 was analyzed in relation to tumor volume it was seen that in p53 positive cases (n=15), tumor volume was 22.57 cm 3 (SD20.19) versus 38.79 cm 3 (SD 40.81) in p53 negative cases (n=15) (student's 't' test: P >0.05 (NS) Analysis of p53 protein in relation to high risk HPV DNA load by Mann-Whitney test again showed no association i.e., there was no specific HPV DNA viral load at which p53 was expressed. Response to chemotherapy Out of the 30 patients studied, 20 qualified to receive chemotherapy and were randomized to VBP (n=10) and VBP-M (n=10) regimes. Subjective response to chemotherapy was observed in 73.3% with bleeding per vaginum (n=15), 81.2% with foul smelling discharge (n=16) and in 64.7% with pain (n=17) in the form of complete relief of symptoms. Response to therapy between VBP and VBP-M is shown in [Table - 5]. Pre and post-chemotherapy p53 Cervical biopsy specimens were assessed for p53 protein one week after completion of chemotherapy. Out of the 20 patients who qualified for chemotherapy, 12 showed positive p53 expression pre-chemotherapy versus positive p53 in 13 patients post-chemotherapy. McNemar test was applied to samples preand post-chemotherapy and no difference was found between the groups using 2-tailed binomial distribution ( P =1.000). Using Fischer's exact test for Intergroup comparison (VBP vs. VBP-M) no difference in p53 expression was found post- chemotherapy ( P =0.5). Discussion Indian studies have reported presence of HPV 16/18 in 69.1 to 87.8% of invasive cervical carcinoma.[8],[18] A study from Chennai reported 99.5% presence of high risk HPV in invasive cervical cancer and 23 different HPV types were found although HPV 16 and 18 were most common.[19] In the report from Andhra Pradesh, the most frequently detected HPV types in the Medchal community were HPV 52 and 16.[18] Thus regional variations of high risk HPV may exist. The prevalence of high risk HPV in small screening programs in normal women in India was roughly 10% as compared to 43 and 94% in normal women and CIN respectively in western women.[18],[20],[3] The sensitivity of HPV in the detection of CIN 2 and 3 from various centers in India varied from 45.7 to 80.9% by the HC II assay.[21] In the present study, high risk HPV by HC II assay was found in 100% of cervical cancer cases and none of the controls and adds to the current limited literature from India. In this study HPV viral load was found to be directly proportional to stage as well as tumor volume. In a study by Clavel et al , it was found that; women with high-grade lesions had significantly higher signal strengths for high risk HPV than the rest of the population.[9] HPV viral load has been studied extensively in cervical intraepithelial neo-plasia and less so in invasive cervical carcinoma. A dose-response relationship between HPV viral load and both LSIL (low grade squamous intraepithelial lesion) and HSIL (high grade squamous intraepithelial lesion) has been reported but Lorincz et al suggest that presence of high risk HPV rather than viral load strongly increases risk of CIN 3 or cervical cancer.[22],[23] High viral loads predicting risk of invasive cervical carcinoma was also reported by Moberg.[24] HPV viral load for prognosis for cervical cancer has not been studied sufficiently. We believe this may be the only other study evaluating HPV viral load in invasive cancer cervix and may be useful for predicting prognosis and recurrence. In a recent report, Singh et al suggested that the presence of HPV and HPV viral load in exfoliated cervical cells post radiotherapy can be used for early detection of patients at increased risk for disease recurrence and progression.[25] However a limitation of the present study is that HPV was not evaluated post chemotherapy and the study was a short term response to chemotherapy. During the past decade, molecular mechanisms involved in the pathogenesis of cervical cancer have been explored extensively. The present study demonstrated high risk HPV DNA in all cervical cancer cases and p53 expression in 50% of cases but when high risk HPV DNA load was analyzed with p53 (McNemar's test) no association between the two was found, i.e., there was no precise viral load (RLU/cut off value) at which p53 was deregulated implying that p53 may be affected early in the course of disease. Dimitrakakis et al ,[16] found that immunoreactive p53 was detected in 29% of cells in cancer cervix patients while no p53 expression was found in normal cervices and 3 out of 20 cases of CIN III stained positive for p53 protein. In the present study 50% of cancer cervix cases expressed p53 protein while normal cervical tissue was negative in all cases. Sahu et al in their study concluded that rearrangement of p53 rather than mutation results in expression of p53 in cervical cancer and a 50% expression by immunohistochemistry and Western blot analysis was found.[26] In another study by Borresan et al , 69 cervical cancer cases were examined for evidence of over expressed, deregulated p53 protein using DO-7 monoclonal antibody.[27] Seven (10%) cases showed the evidence of altered p53 proteins. All the cases were positive for HPV 16. They concluded that mutations in p53 resulting in deregulated p53 protein, is infrequent in cervical cancers. However in another study using the same monoclonal antibody, DO-7, all cases of cervical cancer cases showed overexpression of p53.[28] Thus p53 expression is variable may be due to deregulation rather than mutation as was seen in this study. Dimitrakakis based on limited samples, indicate that bcl-2 expression (apoptosis control gene) may provide additional and independent prognostic information to predict clinical course of cervical cancer and have recommended more extensive series.[16] Grace et al suggest a significant direct correlation between p53 and bcl-2 expression in a study of 105 cases cervical cancer.[29] While analyzing p53 in patients with invasive cervical cancer stages IB to IIB, Kainz et al , reported no prognostic significance of p53 in surgically treated cervical cancer.[30] However, some studies have demonstrated an association between p53 protein accumulation and aggressive behavior of carcinoma, including a genetic propensity towards metastasis and recurrence.[31] Tilting the balance in favor of p53 by novel treatment protocols might reestablish the tumor suppressor function of p53 in cervical carcinoma cells. The present study could not demonstrate any change in p53 pre and post-chemotherapy. A major limitation of this study was the limited numbers available for chemotherapy randomization and study. Response rates were similar in both groups [Table - 5]. However a higher operability rate was seen in the VBP-M group (66%) in stage II B cervical cancer. Five out of twelve patients of stage IIB had disappearance of parametrial extension and became operable; of these four received VBP-M chemotherapy and one VBP. One patient of VBP-M had a pathologically proven complete response. The effect of mitomycin-C in HPV infected cells may be both p53 dependent and independent and must be explored in chemotherapy and chemoradiation protocols in cancer cervix.[15] Both regimes showed a 'quality of life improvement' post chemotherapy in the form disappearance of foul smelling discharge, bleeding and pain and this was noted in previously published reports.[10],[11] Conclusion In conclusion HPV viral load, p53 assessment and use of mitomycin-C as a chemotherapeutic agent in cancer cervix have potential implications in management of invasive squamous cell carcinoma of cervix and need to be explored in larger trials.References
Copyright 2006 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn06025t3.jpg] [cn06025t2.jpg] [cn06025f1.jpg] [cn06025t5.jpg] [cn06025t1.jpg] [cn06025t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}