 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
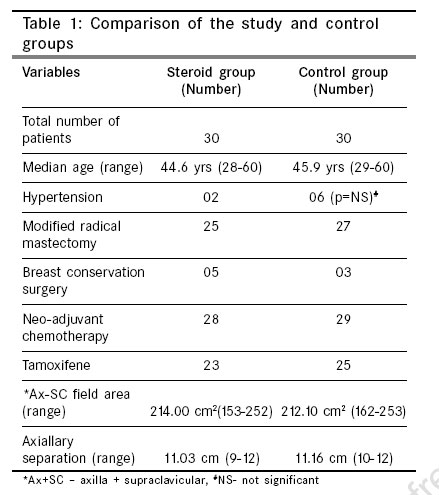
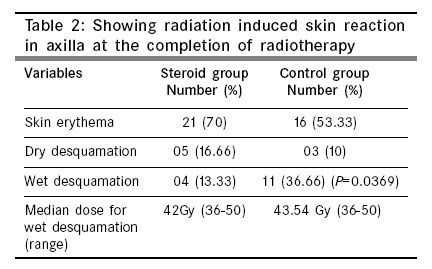
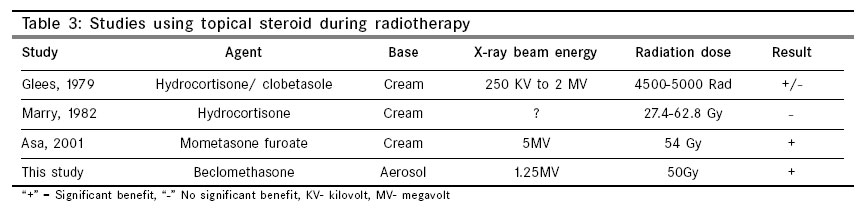
Indian Journal of Cancer, Vol. 43, No. 4, October-December, 2006, pp. 180-184 Original Article Prophylactic beclomethasone spray to the skin during postoperative radiotherapy of carcinoma breast: A prospective randomized study Shukla PN, Gairola M, Mohanti BK, Rath GK Department of Radiation Oncology, Ratan Cancer Hospital and Research Institute, 113/103A, Swaroop Nagar, Kanpur - 208 002 Code Number: cn06029 Abstract Background and Aims: Radiation induced wet desquamation of skin in carcinoma breast patients is a painful condition. In this study topical beclomethasone dipropionate spray was used as prophylaxis with the purpose of reducing risk of the wet desquamation of skin in irradiated field.Materials and methods: Sixty patients of carcinoma breast were planned for postoperative loco regional radiotherapy (50 Gy in 25 fraction over five weeks) were prospectively randomized into two groups (1) steroid group-patients were advised to use beclomethasone dipropionate spray in irradiated axilla from day one of radiotherapy, (2) control group-patients were not allowed to use any topical agent in irradiated area. Radiation induced skin reaction was noted in terms of erythema, dry desquamation and wet desquamation weekly till end of prescribed 50Gy dose of the radiation therapy. Statistical Method: Chi-square test was used to see the statistical significance of the difference in wet desquamation between two arms of the study. Chi-square value and P -value was calculated for the difference of wet desquamation in two study arms. Result: In steroid group 4/30 (13.33%) patients developed wet desquamation of the axillary skin at the end of the radiotherapy. For the control group, this figure was 11/30 (36.66%). The difference in wet desquamation of the axillary skin in the two groups was statistically significant ( P -value= 0.0369). Conclusion: Topical steroid (beclomethasone dipropionate spray) for skin during radiotherapy significantly reduces the risk of wet desquamation of the skin. Keywords: Breast, carcinoma, dermatitis, radiotherapy, steroid Introduction Radiotherapy plays an important role in the loco-regional management of the operable breast carcinoma. External beam radiotherapy reduces loco-regional recurrence and it also has some acute and late radiation morbidity, wet desquamation of the irradiated skin is one of them. Wet desquamation of the skin, although significantly less in incidence with megavoltage beam than kilo voltage beam, but it still continues to be a painful condition for the patient of carcinoma breast receiving external beam radiotherapy. This painful wet desquamation mainly spreads over axilla for a period of 4-12 weeks. This study was started with the aim to further reduce the risk of wet desquamation in these patients. Some studies have been done in this direction but only few of them were conclusive in the positive direction. Steroid was chosen as an agent because it is already in practice for the management of radiation dermatitis and aerosol was chosen to avoid the bolus effect.Materials and Methods Patients of carcinoma breast with an indication for postoperative loco-regional radiotherapy (LRRT) were eligible for entry in to this study. Eligibility criteria for randomization to steroid spray or not, included clinico-pathological indication of axillary lymphatic drainage area irradiation after modified radical mastectomy or breast conservation surgery with axillary lymph nodes dissection. Patients with skin disease or abscess in the area to be irradiated were excluded from study. Patients had to be of the KPS level more than 70 with no evidence of distant metastasis. The gap between the last dose of chemotherapy and beginning of radiotherapy was kept as more than seven days and patients were not allowed to take chemotherapy during radiotherapy. Patients required adequate bone marrow reserve with hemoglobin more than 10 gm dl -1; total leucocytes count greater than 3X10 -9 l -1 and platelets greater than 100x10 -9l -1. Patients were also required to have a normal kidney function test and liver function test. Any woman of child bearing potential had to have a negative pregnancy test prior to the onset of radiotherapy. The protocol was discussed in the Department of Radiotherapy All India Institute of Medical Sciences, New Delhi; all patients gave written informed consent. Postoperative LRRT was considered for patients with primary tumor size more than 4 cm or T 4 disease and / or more than 4 lymph nodes positive for tumor or N 2 lymph node disease. ER/ PR positive patients were started with tamoxifene 20 mg once a day. Sixty patients, fulfilling the inclusion criteria were randomized into two arms. (There was no specific reason to keep the sample size small), Arm - 1 (steroid group) patients were advised to use beclomethasone dipropionate spray on irradiated axilla, two puffs each time over morning and evening, seven days a week from day one of radiotherapy. We started steroid spray from day one to have the maximum possible effect, although radiation effect on skin is visible from third week of radiation but actually it starts with first exposure of radiation. Each puff of the spray contained 100 µgm of beclomethasone dipropionate (BMD) which means 200 µgm BMD was applied in the morning and 200 µgm in the evening to the irradiated axilla. The gap of time between use of spray and irradiation was not fixed. Arm -2 (control group) patients were refrained from applying anything in the irradiated area. Both groups of patients were advised not to shave hairs of irradiated axilla and use of soap, oil and cream in the irradiated area was restricted. Patients were allowed to wear only loose cotton clothes on the irradiated part of body. Radiotherapy was done with tele-cobalt unit. For the chest wall or whole breast two tangent fields were used, whereas axillary and ipsilateral supraclavicular (Ax-SC) area together were included by a single anterior field. Axillary radiation dose was calculated at the mid-point of axillary separation. A total dose of 50 Gy in 25 fractions at 5 fractions per week was delivered to the primary site and lymphatic drainage area over a protracted period of five weeks. In patients with conservative breast surgery an additional radiation dose of 16 Gy in 8 fractions was delivered to the primary site as a boost dose. Toxicity A clinical examination and complete blood count were carried out once every week while on treatment. Skin reaction was assessed weekly by the resident doctors posted in review room of radiotherapy department. Final level of skin reaction was seen on the day of completing the prescribed 50 Gy radiation dose and one month after completion of radiotherapy. Grading of the skin reaction was done in the terms of erythema, dry desquamation and wet desquamation. Skin tenderness was not taken in to consideration as many patients had mild tenderness in the area to be irradiated due to the surgical procedure done before radiotherapy. Treatment was stopped after the development of wet desquamation for a short period and 1% gentian violet was applied in the area. In the steroid arm the beclomethasone spray was stopped after the development of wet desquamation in axilla. Other acute radiation morbidity like oesophagitis was managed symptomatically. Statistical Method The main aim of the study was to see the difference in the occurrence of the wet desquamation on the axillary skin between two arms of the study. Chi-square test was used to see the statistical significance of the difference in wet desquamation between two arms of the study. Chi-square value and P -value was calculated for the difference of wet desquamation in two study arms. Result Thirty patients were randomized in each arm of the study. For one patient of the steroid group, loco regional radiotherapy was stopped at 36 Gy with the development of distant metastasis, but this patient was not excluded from the study because this patient had developed wet desquamation in axilla by that time and main aim of our study was to see the effect of steroid on the incidence of wet desquamation during radiotherapy. Features of two groups are comparable and important factors like adjuvant chemotherapy, irradiated area and treatment depth (axillary separation), which may affect skin reaction are shown in [Table - 1]. In steroid group 4 (13.33%) patients and in control group 11 (36.66%), out of 30 patients developed wet desquamation in axilla at the end of prescribed 50 Gy [Table - 2], P -value and Chi-square value for this difference was 0.0369 and 4.36 respectively. There was no significant difference in median dose of radiotherapy causing wet desquamation (42 vs 43.54 Gy). In the steroid group and control group, number of patients with hypertension was two and six respectively, 50% of these patients in each group developed wet desquamation in axilla; the number of these patients was too small to have any statistical significance.Discussion Currently breast cancer patients need multidisciplinary management including surgery, radiotherapy and chemotherapy;[1] radiotherapy has a significant role in loco regional control of the disease.[2] During kilo voltage teletherapy period, risk of radiation skin toxicity was high, as skin was receiving the maximum dose delivered. After introduction of megavoltage therapy, the risk of radiation-induced skin toxicity reduced markedly because of skin sparing advantage of megavoltage photon therapy. If we compare cobalt-60 and 6 MV photon teletherapy, the d-max are at 5 mm and ~15 mm depth respectively; 6 MV photon has better skin sparing property than cobalt-60. This advantage of skin sparing by the megavoltage photon beam has resulted in inadequate number of studies in this field. However, a large number of breast cancer women in developing countries receive LRRT by tele-cobalt therapy and the issue of skin morbidities (chest and axilla) is relevant. Most of the studies using various topical agents as prophylaxis for radiation-induced skin toxicity have used ointment or gel as base. Ointment or gel is not an appropriate choice for patients receiving radiotherapy on tele-cobalt unit, as it has d-max level at just 5 mm and this may result in risk of loosing skin-sparing advantage to some extent. Therefore, we have used aerosol as base for the topical agent-beclomethasone dipropionate. Steroids are well known for their anti-inflammatory property and for long they have been in use for the management of acute radiation toxicity. Steroids have also been tried in the management of the radiation induced toxicity of the rectum.[3] Although steroids given systemically or topically will have anti inflammatory effect but steroids given systemically will have much more side-effects, of steroid while steroids given topically will have much less systemic effect; more importantly our aim is to have local effect of the steroid. Irradiation shows gradual reddening during the third and fourth week of treatment course. Techniques of irradiating the breast or chest wall largely produce dry desquamation, but in a proportion of patients bothersome moist desquamation appear beyond 35-40 Gy. In patients with involvement of skin or inflammatory changes, it may be necessary to have maximal effect on skin surface and often a wax bolus is applied to increase the dose to skin. Moist desquamation will result and then will heal in a predictable manner in the weeks following completion of irradiation. Most common sites for wet desquamation are axilla and infra-mammary fold. This wet desquamation is a very painful condition for the patient and at the same time the radiation therapy may be interrupted if it appears before the completion of radiotherapy. The patho-physiology of radiation induced skin morbidities is thought to represent a secondary inflammatory reaction, possibly from the release of cytokines from dying cells. Dry desquamation is an atypical keratinization of skin due to reduction in the number of clonogenic cells within the basal layer of epidermis. Moist desquamation is loss of epidermis due to the sterilization of a high proportion of the clonogenic cells within the basal layer of epidermis. Recovery of a patch of moist desquamation depends upon regenerative activity of clonogenic basal cells remaining in irradiated area,[4],[5] larger the area being irradiated the less ability the skin has to regenerate due to an increase in the area of capillary obstruction. The various factors involved in the increase of radiation induced skin reactions include; radiation dose, skin-sparing effect of beam, large area, skin disease in irradiated area, diabetes mellitus and high blood pressure.[6],[7],[8] In our study also 50% of the high blood pressure patients developed wet desquamation in axilla. Various topical agents have been used as prophylaxis to reduce skin toxicity, induced by radiotherapy.[9],[10],[11],[12],[13],[14],[15] We could find only three significant studies using topical steroid as prophylaxis for radiation induced skin toxicity[9],[11],[13] [Table - 3]. In the study by Glees et al[11] patients were randomized to two different topical steroid arms with hydrocortisone and clobetasone respectively. Most of the patients were treated with 250 KV teletherapy machine and risk of skin toxicity was high among these patients, as discussed earlier; but skin toxicity at the end of radiotherapy was significantly less in hydrocortisone arm, although the authors concluded that overall there was not significant difference in the two arms of the study. There were multiple lacunae in study by Marry et al[13] (a) number of patients was small, 21 patients, (b) tumors of various parts of body (head and neck, thorax and abdomen) were included which will result in large variation in field size and depth of the target, (c) large variation in dose delivered- 27.4 Gy to 62.8 Gy. In these two studies, the topical steroid was not prescribed from the beginning of radiotherapy, which may have compromised the efficacy of the steroid, as toxic effect of radiation starts from the first fraction of radiotherapy.[16] Recent study by Asa et al[9] is an important study in this direction, 5 MV photon was used to treat carcinoma breast patients, the patients were randomized to topical corticosteroid cream of mometasone furoate, in steroid arm 4/24 patients had wet desquamation while in control arm 10/25 patients had wet desquamation of skin, this difference was statistically significant. In our study, the aerosol preparation of steroid was chosen to avoid the bolus effect of the topical agent on skin. Since most patients in our center were treated after modified radical mastectomy, steroid was applied only in axilla. The difference in two arms was statistically significant ( P -value 0.0369) for radiation induced wet desquamation in axilla. The decrease in risk of wet desquamation with steroid may be because of (a) anti inflammatory effect, (b) steroid reduces the local irritation and itching which in turn results in lower risk of mechanical irritation (scratching) by the patient. In study of Asa et al , it was seen that steroid arm patients experienced less itching and burning. Conclusion Wet desquamation of skin following radiotherapy is a painful condition for the patient and there is a place for prophylactic measure to prevent this painful condition. Our study shows significant reduction in risk of wet desquamation with topical steroid. Steroid should be used from the onset of radiotherapy to get maximum effect. Bolus forming agents should be avoided, especially with tele-cobalt radiotherapy unit.References
Copyright 2006 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn06029t3.jpg] [cn06029t2.jpg] [cn06029t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}