 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
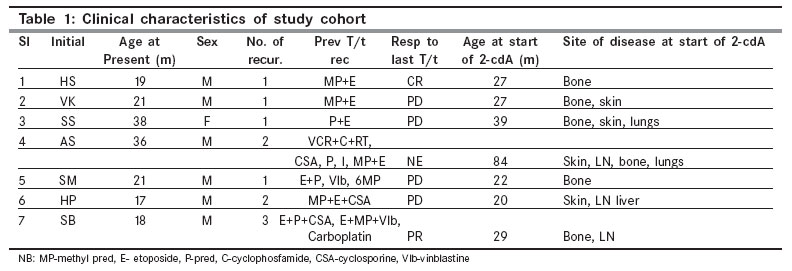
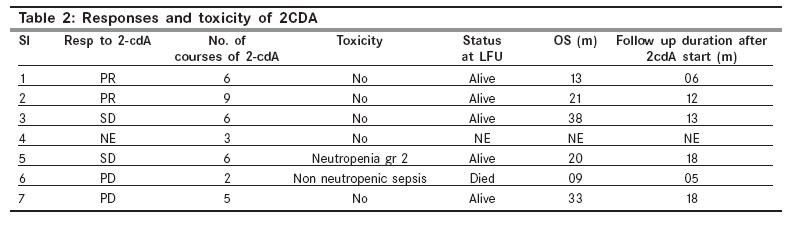
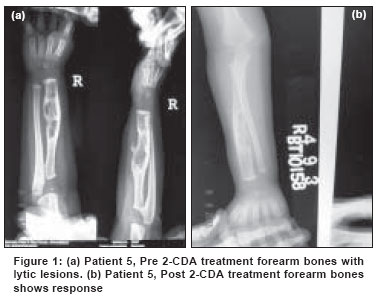
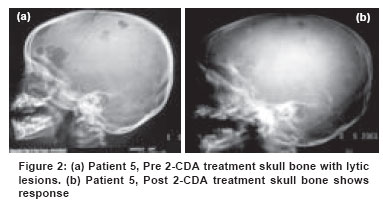
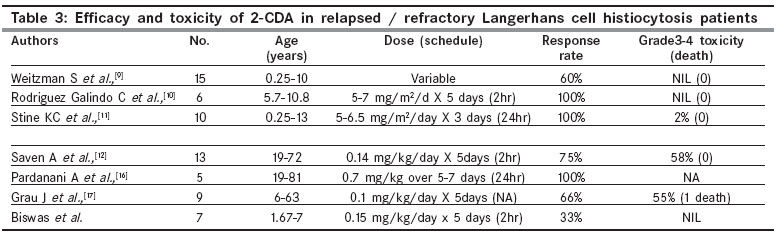
Indian Journal of Cancer, Vol. 44, No. 4, October-December, 2007, pp. 137-141 Original Article Activity and toxicity of 2-CDA in Langerhans cell histiocytosis: A single institutional experience Biswas G, Khadwal A, Arora B, Bhagwat R, Banavali SD, Nair CN, Pai SK, Kurkure PA, Parikh PM Department of Medical Oncology, 808, GJB, Tata Memorial Centre, Parel - 400 012, Mumbai Correspondence Address: Purna A Kurkure, Department of Medical Oncology, 808, GJB, Tata Memorial Centre, Parel - 400 012, Mumbai, E-mail: kurkurepa@tmcmail.com Code Number: cn07025 Abstract Background : Langerhans cell histiocytosis (LCH) is a rare disorder characterized by clonal proliferation of immature and abnormal bone marrow derived langerhans cells. Treatment is usually multimodal. Potent anti-monocyte as well as immunomodulatory activity of 2-CDA and its proven efficacy in many lymphoproliferative disorders has made 2-CDA a rational choice in treatment of LCH. Keywords: 2-CDA, Langerhans cell histiocytosiso Introduction Langerhans cell histiocytosis (LCH) is a rare atypical cellular disorder characterized by clonal proliferation of immature and abnormal bone marrow derived langerhans cells. The nosogenesis of this enigmatic disorder is still unclear. On one end monoclonality suggests a neoplastic process; [1] while spontaneous remissions, benign appearing pathologic lesions and involution in response to immunosuppressants point to a reactive immunologic process. The disease course of the individual patients is highly variable; from indolent to aggressive and from spontaneous remissions to rapid death. [2],[3] The mortality for single or multisystem LCH without risk organ involvement is less than 10%, whereas in risk organ involvement mortality of 30-50% has been reported. [4] In addition to risk of death, more than 50% of patients without risk organ involvement and a larger number with risk organ involvement develop one or more sequale inspite of optimal treatment. [5] Hence there is a pressing need to have novel, more potent and less toxic therapies in LCH. The common origin of monocytes and progenitor cells of LCH, potent anti-monocyte [6] as well as immunomodulatory activity of 2-CDA [7] and its proven efficacy in many lymphoproliferative disorders has made 2-CDA a rational choice in treatment of LCH and other histiocytic disorders. [8] Many small recent studies have shown this drug to have a promising activity in LCH. [9],[10],[11],[12] We, therefore, have evaluated the efficacy and toxicity profile of 2-CDA in children with relapsed or refractory LCH in a pilot study and hereby present the initial data of the first seven patients treated at our institution. Materials and Methods Eligibility criteria All patients less than 15 years of age with relapsed or refractory LCH (irrespective of prior chemotherapy, steroids, radiation therapy) who were off chemotherapy or radiation therapy for more than four weeks were enrolled. Adequate renal (serum creatinine < 2.0 mg/dL) and hepatic function (bilirubin, alkaline phosphatase, serum glutamic oxaloacetic transaminase (SGOT), serum glutamic pyruvate transaminase (SGPT) < 2 times normal) was required. The histopathologic diagnosis was based on the demonstration of CD1a antigenic determinants on the surface of lesional cells or the finding of Birbeck granules in lesional cells by electron microscopy, wherever possible or positive immunostaining with two or more of the following : adenosine triphosphatase (ATPase), S-100 protein or alpha-D-mannosidase. Presumptive diagnosis was made when findings, on study of conventionally stained biopsy material alone, were merely "consistent" with those defined in the literature. Baseline and follow-up evaluation Before the initiation of therapy, patients underwent a complete history and physical examination, complete blood count with differential and platelet count, biochemistry panel, bone marrow aspiration and biopsy, chest X-ray, skeletal survey, ultrasound scan of the abdomen and biopsy of affected tissue or organs wherever feasible. During therapy and subsequent follow-up, patients underwent a complete history, physical examination, complete blood count with differential and biochemistry before each course of cladribine. One month after the completion of the third course of cladribine, patients were clinically assessed for response. Complete blood counts, biochemistry, skeletal survey, bone marrow aspiration and biopsy, ultrasound scan of the abdomen and chest X-ray were repeated after three courses, if previously abnormal and again at maximum response and three monthly thereafter in first year and six monthly in second year. Cladribine therapy Cladribine was administered at 0.15- 0.3 mg/kg per day over two hours intravenously daily for five consecutive days with courses repeated every four weeks, toxicity permitting. If, four weeks after the completion of the third course of cladribine, the patient did not achieve a complete (CR), partial (PR) or stable response (SD), then no further cladribine was administered. The patient was then switched over to alternative therapy. If, four weeks after the completion of the third course of cladribine a CR, PR or SD had been achieved, cladribine was administered until maximum response or prohibitive toxicity was encountered. If a complete response had been achieved, then the patient received no further cladribine until documented disease recurrence, when this occurred . Response and toxicity criteria CR was defined as the absence of active disease on physical examination and imaging studies. Cutaneous lesions did not require repeat biopsy to document histologic resolution. PR was defined as a reduction by more than 50% of all measurable disease for more than one month. PD was defined as more than 25% increase in the measurable disease or appearance of new lesions. SD was defined when neither PR nor PD criteria were met. The National Cancer Institute Common Toxicity Criteria were used for the evaluation of toxicity with grade 3 and 4 being considered significant. The initiation of cladribine therapy was delayed till absolute granulocyte count was > 1.0 x 10 9 per liter and the platelet count was > 100 x 10 9 per liter. Results Patient characteristics [Table - 1] Of the seven patients treated, six were boys and only one was a girl child. The median age at initiation of cladribine was 2.25 years (range, 1.67 to 7.0 years) and the median pretreatment disease duration was 10 months (range, 3 to 62 months). Three patients had received one prior chemotherapy regimen while the rest were heavily pretreated. One patient had received prior radiation also. Using the Risk grouping system as adopted by LCH-III protocol, two patients had Group1 disease (Multisystem risk patients), 2 patients had group 2 disease (Multisystem low-risk disease) and rest three patients had group 3 disease (Multifocal bone disease or localized special site involvement) of which 1 had central nervous system risk lesion. The sites of active disease before the initiation of cladribine were skin in four patients, bone (all multifocal) in six patients, lung in two patients, liver in one patient and lymph nodes in three patients. Responses and toxicities [Table - 2] Only seven patients with histopathological diagnosis of LCH and clinically or radiologicaly measurable disease and symptoms were enrolled from July 2000 to June 2004 due to the cost and non-uniform availability of the drug. Of the seven patients treated, six were evaluable for response and all for toxicity. Patient 4, not evaluable for response, received three courses of therapy and was subsequently lost to follow-up. After a median of 6 courses of cladribine (range, 2 to 9), two (33%) patients achieved PR and two (33%) patients have SD on imaging but are clinically better. The median follow-up duration after 2-CDA start was 12 months (range, 5 to 18+ months). Individual patient responses and their duration are shown in [Table - 2]. The skeletal response of patient 5 is shown in [Figure - 1]ab and [Figure - 2]ab. The principal acute toxicity was hematologic. None experienced grade 3 or 4 hematologic toxicity. In none of these seven patients, neutropenia was complicated by fever necessitating hospital admission for intravenous antibiotics. No patients experienced grade 3 to 4 anemia or grade 3 to 4 thrombocytopenia. The treatment of Patient no.6 was complicated by diarrhea and sepsis requiring admission leading to death. None of the patients had significant hepatic (transaminitis) or renal toxicity (renal tubular acidosis) as reported in other studies. Also, none had peripheral neuropathy reported with higher doses of 2-CDA. At a median follow-up of 19 months (range, 8 to 52 months), five patients remain alive and one patient (patient 6) has died. Discussion Our study shows that single agent 2-CDA is active and well-tolerated in children with relapsed or refractory LCH. These results further confirm and extend the observations made in other studies of 2-CDA in children with LCH. [9],[10],[11] 2-CDA is a purine analog resistant to the catalyzation by enzyme ADA. The metabolite inhibits the DNA synthesis. 2-CDA is active against both resting and actively dividing lymphocytes and is effective in both B and T- cell disorders. [8],[13] The response rates range from 50-90% in various lymphoproliferative disorders with the best results seen in hairy cell leukemia. [8] In children it has been found to be effective in acute myeloid leukemia. [14] It has potent toxicity against monocytes, which have common origin as progenitor cells of LCH. [6] Furthermore, it has strong immunomodulatory activity. [7] Pathological langerhans cells (LCH cells) are actively involved in a immunoreactive cytokine production loop involving T-cells and macrophages. The key nosogenic cytokines involved in this cascade are GM-CSF, IL-1, IL-3 and TNF. [15] The interruption of this loop might be one mode of action of 2-CDA due to its strong immunosuppressive effect. This strong rationale led to the usage of 2-CDA in histiocytic disorders. Many small studies [9],[10],[11],[12],[16],[17] have been conducted which are summarized in [Table - 3]. Most of these studies have been conducted in relapsed or refractory setting with small patient numbers ranging from 5-15. The dose and schedule in these studies have been variable with dose ranging from 5 mg/m2/day CI for seven days to 13 mg/m2/day as CI over five days. The response rate in these studies has ranged from 33% to 100%. [9],[10],[11],[12],[16],[17] The response rate (33%) in our study has been modest which could potentially be due to a small patient number and short follow up as it has been observed that response with 2-CDA may continue to occur even months after the treatment cessation. The dose and schedule is unlikely to have had any impact on the response since studies in adults have shown that moderate doses in 2-h schedule may be as effective as a 24-h continuous schedule. [18] 2-CDA has been shown to be effective in the acute progressive LCH in prior studies but in our study one patient progressed on treatment and died of the disease. 2-CDA has good central nervous system (CNS) penetration and has been shown to be effective in prior studies in patients with CNS disease; [11] but in our study none had CNS parenchymal disease so it could not be confirmed. It has been observed in few studies that patients, who relapse after 2-CDA, may again achieve remission after re-challenge with 2-CDA. [10] The acute toxicity of 2-CDA in all pediatric studies including the present study has been minimal and tolerable. Transient myelosuppression is the most common side effect and significant grade 3-4 toxicity or treatment-related death has not been observed in pediatric studies so far. [9],[10],[11] However in two adult studies> 50% patients had grade 3-4 myelosuppression. [12],[17] One cause for concern regarding 2-CDA usage in LCH is the long-term immunosuppression, which may be more due to higher number of courses of 2-CDA compared to other disorders. This may increase the risk of secondary cancers. [19] However, the data is limited and the follow-up is too short to assess this risk in the studies done till date. Conclusion The present therapeutic options in LCH are limited by modest efficacy and potential for long-term toxicity. 2-CDA as a single agent is active and well-tolerated in relapsed or refractory LCH and warrants further study (either alone or in combination) in high-risk chemo naive patients or relapsed disease. Its synergistic efficacy with other chemotherapy drugs such as cyclophosphamide and cytarabine [20] and its subcutaneous as well as oral bioavailability [18] make it an attractive therapeutic option. The incorporation of this promising agent in the therapeutic armamentarium against LCH may improve the cure rate of this disease with dismal prognosis.References
Copyright 2007 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn07025t3.jpg] [cn07025t2.jpg] [cn07025f2.jpg] [cn07025f1.jpg] [cn07025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}