 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 44, No. 4, October-December, 2007, pp. 155-156 Case Report Penile metastasis from rectal carcinoma Murhekar KM, Majhi U, Mahajan V, Satheesan B Department of Surgical Oncology, Cancer Institute (WIA), Adyar, Chennai - 600 020
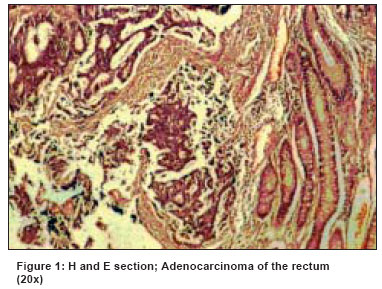
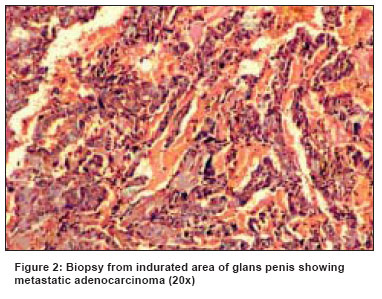
Code Number: cn07028 Abstract Penile metastases are infrequent and often originate from genitor-urinary organs including bladder and prostate. In the present communication, we report an unusual case of penile metastasis from rectal adenocarcinoma. Though uncommon, this presentation is not unknown. A review of literature of penile metastases in colorectal cancers is also summarized here.Keywords: Penile metastasis, rectal carcinoma Introduction Despite its rich vascularization and extensive circulatory communication between the neighboring organs, metastatic involvement of the penis is relatively infrequent. Most of the primary tumors that metastasize to penis originate from pelvic uro-genital organs [1],[2],[3] and rarely from rectum and recto-sigmoid. [3],[4],[5],[6],[7] Patients with penile metastasis usually have widespread metastatic disease. [8] We report here a case of adenocarcinoma of rectum with isolated penile metastasis.Case Report A 78-year-old gentleman presented with tenesmus, bleeding per rectum and altered bowel habits of six months duration in 2004. Clinical evaluation revealed an ulcero-proliferative growth starting at 2 cm. from anal verge extending upwards for 6 cm. involving the three fourth the circumference of the rectum. Biopsy of the lesion revealed adenocarcinoma grade II-III with nuclear grade intermediate [Figure - 1]. Computed tomographic study of the abdomen, pelvis and x-ray chest showed no evidence of distant metastasis. The patient underwent abdomino-perineal resection in January 2004. Intra-operatively there was no detectable metastasis in liver, peritoneum, para-aortic region and other intra-abdominal organs. Postoperative histopathology revealed pathological T3 tumor [TNM Staging system 2002] with metastases in two regional lymph nodes [two out of nine nodes]. Though adjuvant chemo-radiotherapy was advised, patient failed to receive the same due to logistic reasons. He was on regular follow-up. In January 2006 he presented with phimosis and associated urinary difficulty. Clinical examination showed an indurated lesion palpable in the glans penis beneath the covered preputial skin with multiple hard nodules along the penile urethra and right corpus cavernosa close to the root of penis. Biopsy of the glans lesion was done after dorsal slit. It revealed metastatic adenocarcinoma [Figure - 2]. The slides of the primary tumor were compared with the penile lesion and the appearance was similar. Immunohistochemical study demonstrated positive staining of the tumor cells for carcino-embryonic antigen [CEA]. The patient was advised palliative chemotherapy, which he refused. He was subsequently catheterized after a month for urinary obstruction. He developed mild pain in the penile shaft after two months. He is on symptomatic and supportive care. Discussion The first report of rectal carcinoma metastasizing to penis was described in 1870. [8] Since then few reports of metastatic penile carcinoma from primary tumor in rectum have been described in literature. [3],[4],[5],[6],[7] The most commonly accepted modes of spread to penis are through (1) retrograde venous spread (2) retrograde lymphatic spread (3) arterial spread (4) direct extension and (5) secondary embolization. Patients with penile metastasis usually have widespread metastatic disease and thereby poor general health. However, there are reports of delayed penile metastasis years after the primary has been treated and without evidence of any other metastatic lesions, as in the present case. The common presentations of penile metastasis are corporal mass, cutaneous nodule, malignant priapism or nonspecific refractory lower urinary tract symptoms. [9] Diagnosis is usually made by biopsy or corporeal aspiration. Management of penile metastasis is mainly palliative. The management is influenced by size of primary, extent of metastatic spread, general condition of the patient and also prognostic features of the primary tumor. The treatment modalities include radiotherapy, chemotherapy and surgery, with survival ranging from three to 18 months from time of diagnosis. Penectomy is a radical procedure advocated by some authors, [10] although the survival benefit remains controversial. Others have suggested that it should only be reserved for cases where metastases are isolated to only the penis. [11] Prognosis is usually poor and majority of patients presenting this way die within one year. In conclusion, this report is an additional new case of primary rectal adenocarcinoma with isolated penile metastasis. Though penile metastatic lesions are infrequent, it should always be considered in the differential diagnosis in a patient with primary malignancies of urogenital organs and colorectum who is presenting with either synchronous or metachronus penile lesions. References
Copyright 2007 - Indian Journal of Cancer Indian Journal of Cancer, Vol. 44, No. 4, October-December, 2007, pp. 155-156 Case Report Penile metastasis from rectal carcinoma Murhekar KM, Majhi U, Mahajan V, Satheesan B Department of Surgical Oncology, Cancer Institute (WIA), Adyar, Chennai - 600 020
Code Number: cn07028 Abstract Penile metastases are infrequent and often originate from genitor-urinary organs including bladder and prostate. In the present communication, we report an unusual case of penile metastasis from rectal adenocarcinoma. Though uncommon, this presentation is not unknown. A review of literature of penile metastases in colorectal cancers is also summarized here.Keywords: Penile metastasis, rectal carcinoma Introduction Despite its rich vascularization and extensive circulatory communication between the neighboring organs, metastatic involvement of the penis is relatively infrequent. Most of the primary tumors that metastasize to penis originate from pelvic uro-genital organs [1],[2],[3] and rarely from rectum and recto-sigmoid. [3],[4],[5],[6],[7] Patients with penile metastasis usually have widespread metastatic disease. [8] We report here a case of adenocarcinoma of rectum with isolated penile metastasis.Case Report A 78-year-old gentleman presented with tenesmus, bleeding per rectum and altered bowel habits of six months duration in 2004. Clinical evaluation revealed an ulcero-proliferative growth starting at 2 cm. from anal verge extending upwards for 6 cm. involving the three fourth the circumference of the rectum. Biopsy of the lesion revealed adenocarcinoma grade II-III with nuclear grade intermediate [Figure - 1]. Computed tomographic study of the abdomen, pelvis and x-ray chest showed no evidence of distant metastasis. The patient underwent abdomino-perineal resection in January 2004. Intra-operatively there was no detectable metastasis in liver, peritoneum, para-aortic region and other intra-abdominal organs. Postoperative histopathology revealed pathological T3 tumor [TNM Staging system 2002] with metastases in two regional lymph nodes [two out of nine nodes]. Though adjuvant chemo-radiotherapy was advised, patient failed to receive the same due to logistic reasons. He was on regular follow-up. In January 2006 he presented with phimosis and associated urinary difficulty. Clinical examination showed an indurated lesion palpable in the glans penis beneath the covered preputial skin with multiple hard nodules along the penile urethra and right corpus cavernosa close to the root of penis. Biopsy of the glans lesion was done after dorsal slit. It revealed metastatic adenocarcinoma [Figure - 2]. The slides of the primary tumor were compared with the penile lesion and the appearance was similar. Immunohistochemical study demonstrated positive staining of the tumor cells for carcino-embryonic antigen [CEA]. The patient was advised palliative chemotherapy, which he refused. He was subsequently catheterized after a month for urinary obstruction. He developed mild pain in the penile shaft after two months. He is on symptomatic and supportive care. Discussion The first report of rectal carcinoma metastasizing to penis was described in 1870. [8] Since then few reports of metastatic penile carcinoma from primary tumor in rectum have been described in literature. [3],[4],[5],[6],[7] The most commonly accepted modes of spread to penis are through (1) retrograde venous spread (2) retrograde lymphatic spread (3) arterial spread (4) direct extension and (5) secondary embolization. Patients with penile metastasis usually have widespread metastatic disease and thereby poor general health. However, there are reports of delayed penile metastasis years after the primary has been treated and without evidence of any other metastatic lesions, as in the present case. The common presentations of penile metastasis are corporal mass, cutaneous nodule, malignant priapism or nonspecific refractory lower urinary tract symptoms. [9] Diagnosis is usually made by biopsy or corporeal aspiration. Management of penile metastasis is mainly palliative. The management is influenced by size of primary, extent of metastatic spread, general condition of the patient and also prognostic features of the primary tumor. The treatment modalities include radiotherapy, chemotherapy and surgery, with survival ranging from three to 18 months from time of diagnosis. Penectomy is a radical procedure advocated by some authors, [10] although the survival benefit remains controversial. Others have suggested that it should only be reserved for cases where metastases are isolated to only the penis. [11] Prognosis is usually poor and majority of patients presenting this way die within one year. In conclusion, this report is an additional new case of primary rectal adenocarcinoma with isolated penile metastasis. Though penile metastatic lesions are infrequent, it should always be considered in the differential diagnosis in a patient with primary malignancies of urogenital organs and colorectum who is presenting with either synchronous or metachronus penile lesions. References
Copyright 2007 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn07028f1.jpg] [cn07028f2.jpg] |
| |||||||||

{kind=link}
{kind=link}