 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 44, No. 4, October-December, 2007, pp. 157-158 Case Report Radiotherapy-induced depigmentation in a patient with breast cancer Munshi Anusheel, Jain Sandeep, Budrukkar Ashwini, Jalali Rakesh, Sarin Rajiv Department of Radiation Oncology, Tata Memorial Hospital, Parel, Mumbai
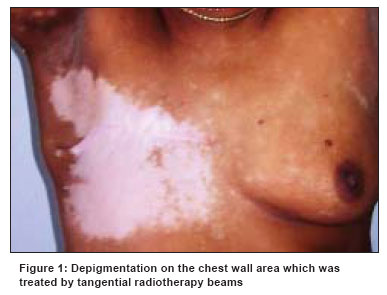
Code Number: cn07029 Abstract Vitiligo is a common dermatological disorder. A middle-aged woman with preexisting vitiligo was diagnosed with breast carcinoma. After surgery and chemotherapy she received regional radiotherapy. Six months after the completion of radiotherapy she developed depigmentation in the irradiated area. This article discusses the etiology for this phenomenon and the literature in this regard.Keywords: Breast cancer, depigmentation, radiotherapy Vitiligo is a common skin disease that is reported to affect approximately 1% of the population worldwide. [1] Though not a life-threatening disease, the effects of vitiligo can be cosmetically and psychologically devastating, resulting in a low self-esteem and poor body image. The cause of this condition is uncertain but seems to be dependent on the interaction of genetic, immunological, and neurogenic factors. [2] Here, we report a case of a patient with vitiligo who developed depigmentation in the irradiated area after radiotherapy for breast cancer. We further discuss radiation-induced Koebner's phenomenon and its molecular mechanisms. Case Report A 42-year-old perimenopausal woman presented with a painless lump of 3 months duration in her right breast. She had a 10-year history of untreated vitiligo on the lips and hands [Figure - 1]. She was investigated and diagnosed as having an infiltrating ductal carcinoma of breast of stage T 4B N 1 M 0 . She received four cycles of neoadjuvant chemotherapy [cyclophosphamide, adriamycin, and 5-flourouracil (CEF) regime] which resulted in a partial clinical response. She underwent modified radical mastectomy followed by two cycles of adjuvant chemotherapy with CEF. Subsequently, she received adjuvant external-beam radiotherapy (EBRT) with tele-cobalt γ-rays to the chest wall and lymphatic drainage sites up to a dose of 45 Gy in 20 fractions over 4 weeks. She had hyperpigmentation and dry desquamation (grade 2 skin reactions, according to the common toxicity criteria) in the radiotherapy portal at the time of completion, which is an expected phenomenon. On the first follow-up after 6 months she complained of progressive white discoloration of the chest wall on the irradiated side. On examination, a depigmented macular area was found, which closely matched the bitangential radiotherapy portals [Figure - 1]. On palpation, there was minimal skin atrophy, with no induration/fibrosis or change in skin elasticity.Discussion Vitiligo is an acquired hypomelanotic disorder characterized by circumscribed depigmented macules in the skin that result from the loss of functional melanocytes. Vitiligo patches can appear anywhere on the skin but common sites are usually around the body orifices, the genitals, or any sun-exposed areas, such as the face and hands. [1] Radiotherapy to the skin results in acute radiation injury to the skin, which is primarily a consequence of the loss of cells from the basal layer of the epidermis, and late injury, which is primarily a function of radiation effects on the vasculature. Commonly, this leads to hyperpigmentation of the skin at the completion of the radiotherapy course. Patients with collagen vascular diseases are known to have an increased radiation sensitivity of normal tissues to radiation damage, and cases of severe radiation skin sequelae, including severe fibrosis and/or necrosis, after breast or chest wall irradiation, have been reported. [3] However, there is no evidence for increased severity of acute or chronic reactions in patients with vitiligo. Fresh depigmented lesions in the radiation portals have however been previously reported in patients with vitiligo who underwent radiation for breast cancer or other cancers. [4],[5],[6],[7] Our patient developed hypopigmentation 6 months after completion of radiotherapy, which is in contrast to the 2 months interval reported by Weizen et al. [6] Furthermore, depigmentation developed in the area irradiated by the tangential portals and not in the skin irradiated by the supraclavicular portal. This is explained by a principle of radiation physics, according to which skin sparing will be more with a direct incident portal compared to an oblique or tangential portal. Tangential portals cause increased electron build-up and consequently increase the dose delivered to the skin. Cases of vitiligo following radiotherapy have been reported in patients with a history of vitiligo, being considered as Koebner's phenomenon (KP). [7] KP, also known as the isomorphic response, is the development of preexisting skin disease following trauma to uninvolved skin. [8] Many forms of environmental stress on skin have been reported as provocating factors for the KP; these include mechanical, chemical, thermal, and infectious stimuli; Ultra-Violet exposure; and various types of dermatitis. The suggested mechanism for this phenomenon is radiation-induced apoptosis of susceptible melanocytes. Loss of melanocytes in the irradiated skin has been demonstrated by Pajonk et al. and correlated with the dose-dependent decrease in the red/green and yellow/blue saturation and overall increase in brightness on colorimetry. [9] Free radical-mediated damage, induced by radiotherapy, may be the initial pathogenic event in melanocyte degeneration in the irradiated skin. The early cell death of melanocytes in vitiligo is related to their increased sensitivity to the oxidative stress caused by irradiation, which may arise from complex processes of abnormal synthesis and processing of tyrosinase-related protein-1 and its interaction with calnexin. [10] Keratinocyte apoptosis can cause lower expression of keratinocyte-derived factors, including stem cell factors and basic fibroblast growth factor. [11] These factors might be responsible for passive melanocyte death, leading to their detachment and transepidermal elimination, and may explain the KP in the vitiligo patients. Recently, however, inhibition of thioredoxin reductase by the high extracellular calcium levels observed in the keratinocytes of vitiligo patients has been also proposed. [7] In patients with preexisting vitiligo, the risks and benefits of radiation therapy should be carefully weighed in order to prevent undesired cosmetic results, particularly in the setting of breast conservation therapy. Preserving the skin by using megavoltage beams and low dose per fraction might improve the cosmetic results of radiation therapy in patients with a history of vitiligo. Study of radiotherapy-induced KP may prove useful in understanding the pathophysiology of vitiligo since the etiology of the disease is still elusive. The choice of therapeutic modality in this radiosensitive group of patients should be made on a case-by-case basis. References
Copyright 2007 - Indian Journal of Cancer Indian Journal of Cancer, Vol. 44, No. 4, October-December, 2007, pp. 157-158 Case Report Radiotherapy-induced depigmentation in a patient with breast cancer Munshi Anusheel, Jain Sandeep, Budrukkar Ashwini, Jalali Rakesh, Sarin Rajiv Department of Radiation Oncology, Tata Memorial Hospital, Parel, Mumbai
Code Number: cn07029 Abstract Vitiligo is a common dermatological disorder. A middle-aged woman with preexisting vitiligo was diagnosed with breast carcinoma. After surgery and chemotherapy she received regional radiotherapy. Six months after the completion of radiotherapy she developed depigmentation in the irradiated area. This article discusses the etiology for this phenomenon and the literature in this regard.Keywords: Breast cancer, depigmentation, radiotherapy Vitiligo is a common skin disease that is reported to affect approximately 1% of the population worldwide. [1] Though not a life-threatening disease, the effects of vitiligo can be cosmetically and psychologically devastating, resulting in a low self-esteem and poor body image. The cause of this condition is uncertain but seems to be dependent on the interaction of genetic, immunological, and neurogenic factors. [2] Here, we report a case of a patient with vitiligo who developed depigmentation in the irradiated area after radiotherapy for breast cancer. We further discuss radiation-induced Koebner's phenomenon and its molecular mechanisms. Case Report A 42-year-old perimenopausal woman presented with a painless lump of 3 months duration in her right breast. She had a 10-year history of untreated vitiligo on the lips and hands [Figure - 1]. She was investigated and diagnosed as having an infiltrating ductal carcinoma of breast of stage T 4B N 1 M 0 . She received four cycles of neoadjuvant chemotherapy [cyclophosphamide, adriamycin, and 5-flourouracil (CEF) regime] which resulted in a partial clinical response. She underwent modified radical mastectomy followed by two cycles of adjuvant chemotherapy with CEF. Subsequently, she received adjuvant external-beam radiotherapy (EBRT) with tele-cobalt γ-rays to the chest wall and lymphatic drainage sites up to a dose of 45 Gy in 20 fractions over 4 weeks. She had hyperpigmentation and dry desquamation (grade 2 skin reactions, according to the common toxicity criteria) in the radiotherapy portal at the time of completion, which is an expected phenomenon. On the first follow-up after 6 months she complained of progressive white discoloration of the chest wall on the irradiated side. On examination, a depigmented macular area was found, which closely matched the bitangential radiotherapy portals [Figure - 1]. On palpation, there was minimal skin atrophy, with no induration/fibrosis or change in skin elasticity.Discussion Vitiligo is an acquired hypomelanotic disorder characterized by circumscribed depigmented macules in the skin that result from the loss of functional melanocytes. Vitiligo patches can appear anywhere on the skin but common sites are usually around the body orifices, the genitals, or any sun-exposed areas, such as the face and hands. [1] Radiotherapy to the skin results in acute radiation injury to the skin, which is primarily a consequence of the loss of cells from the basal layer of the epidermis, and late injury, which is primarily a function of radiation effects on the vasculature. Commonly, this leads to hyperpigmentation of the skin at the completion of the radiotherapy course. Patients with collagen vascular diseases are known to have an increased radiation sensitivity of normal tissues to radiation damage, and cases of severe radiation skin sequelae, including severe fibrosis and/or necrosis, after breast or chest wall irradiation, have been reported. [3] However, there is no evidence for increased severity of acute or chronic reactions in patients with vitiligo. Fresh depigmented lesions in the radiation portals have however been previously reported in patients with vitiligo who underwent radiation for breast cancer or other cancers. [4],[5],[6],[7] Our patient developed hypopigmentation 6 months after completion of radiotherapy, which is in contrast to the 2 months interval reported by Weizen et al. [6] Furthermore, depigmentation developed in the area irradiated by the tangential portals and not in the skin irradiated by the supraclavicular portal. This is explained by a principle of radiation physics, according to which skin sparing will be more with a direct incident portal compared to an oblique or tangential portal. Tangential portals cause increased electron build-up and consequently increase the dose delivered to the skin. Cases of vitiligo following radiotherapy have been reported in patients with a history of vitiligo, being considered as Koebner's phenomenon (KP). [7] KP, also known as the isomorphic response, is the development of preexisting skin disease following trauma to uninvolved skin. [8] Many forms of environmental stress on skin have been reported as provocating factors for the KP; these include mechanical, chemical, thermal, and infectious stimuli; Ultra-Violet exposure; and various types of dermatitis. The suggested mechanism for this phenomenon is radiation-induced apoptosis of susceptible melanocytes. Loss of melanocytes in the irradiated skin has been demonstrated by Pajonk et al. and correlated with the dose-dependent decrease in the red/green and yellow/blue saturation and overall increase in brightness on colorimetry. [9] Free radical-mediated damage, induced by radiotherapy, may be the initial pathogenic event in melanocyte degeneration in the irradiated skin. The early cell death of melanocytes in vitiligo is related to their increased sensitivity to the oxidative stress caused by irradiation, which may arise from complex processes of abnormal synthesis and processing of tyrosinase-related protein-1 and its interaction with calnexin. [10] Keratinocyte apoptosis can cause lower expression of keratinocyte-derived factors, including stem cell factors and basic fibroblast growth factor. [11] These factors might be responsible for passive melanocyte death, leading to their detachment and transepidermal elimination, and may explain the KP in the vitiligo patients. Recently, however, inhibition of thioredoxin reductase by the high extracellular calcium levels observed in the keratinocytes of vitiligo patients has been also proposed. [7] In patients with preexisting vitiligo, the risks and benefits of radiation therapy should be carefully weighed in order to prevent undesired cosmetic results, particularly in the setting of breast conservation therapy. Preserving the skin by using megavoltage beams and low dose per fraction might improve the cosmetic results of radiation therapy in patients with a history of vitiligo. Study of radiotherapy-induced KP may prove useful in understanding the pathophysiology of vitiligo since the etiology of the disease is still elusive. The choice of therapeutic modality in this radiosensitive group of patients should be made on a case-by-case basis. References
Copyright 2007 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn07029f1.jpg] |
| |||||||||

{kind=link}
{kind=link}