 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
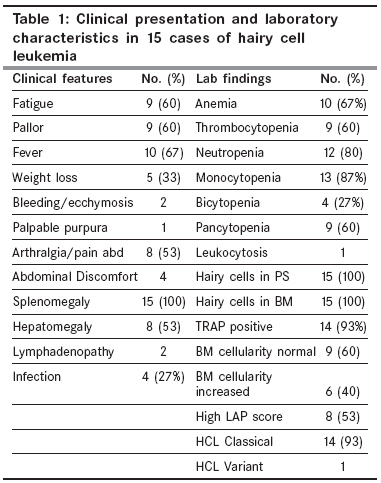
Indian Journal of Cancer, Vol. 45, No. 2, April-June, 2008, pp. 41-44 Original Article Hairy cell leukemia: Clinical, pathological and ultrastructural findings in Asian-Indians Chatterjee T, Panigrahi I, Mahapatra M, Pati HP, Kumar R, Naithani R, Wadhwa S, Choudhry VP, Saxena R Department of Hematology, AIIMS, Ansari Nagar, New Delhi-110 029 Code Number: cn08012 Abstract Background: Hairy-cell leukemia (HCL), lymphoproliferative disease of older age, is characterized by projections from surface of abnormal cells. Keywords: Cladribine, complete response, lymphoproliferative disorder, purine analogs, TRAP test, ultrastructural features Introduction Hairy cell leukemia (HCL) is an indolent, chronic B-cell lymphoproliferative disorder comprising approximately 2 to 3% of all adult leukemias. [1] It occurs more frequently in men (Ratio 4:1) and mean age at diagnosis is approximately 52 years. It is primarily a disease of Caucasians. [2] This series of patients aims at providing an evaluation of clinical presentation, with special emphasis on electron microscopic findings on cladribine therapy.Materials and Methods All HCL cases diagnosed in the Hematology department from December 2001 to January 2004 were evaluated. A histological diagnosis of HCL was done with tartarate-resistant acid phosphatase (TRAP)-positive hairy cells in the peripheral blood or bone marrow. [3] All these patients underwent complete blood counts, liver function tests, renal function tests and skiagram of chest. Clinical details, peripheral blood findings, bone marrow aspirate and biopsies and electron microscopy were reviewed. Bone marrow aspiration was performed by Salah needle and biopsy performed by modified Jenson needle from posterior superior iliac spine. PS and BMA smears were stained by Giemsa stain. Bone marrow biopsy was fixed in formalin, decalcified by formal citrate and stained by hematoxylin and eosin. Cellularity was based on visual examination and graded into three groups; normocellular (30-50% of intertrabecular spaces occupied by hematopoietic cells), hypercellular (>50%) and hypocellular (< 30%). For electron microscopy [LIBRA ® Energy Filtering Transmission Electron Microscopes (EFTEM), Carl Zeiss International], bone marrow aspirates and/or peripheral blood were collected in 2-3 drops of preservative free heparin and processed using standard methods. Ultrathin sections double stained with uranyl acetate and lead citrate. All the pts were treated with 2-chlorodeoxyadenosine (2-CdA) Cladrim (2-chloro-deoxy adenosine; Dabur Pharma Ltd, Chennai) at a dose of 0.09 mg/kg/d continuous iv infusion for seven days; with pump, using a PICC. Complete response (CR) was defined as absence of hairy cells in bone marrow aspirates and biopsy at three and six months after cessation of therapy as well as cessation of symptoms related to pancytopenia as well as normalization of counts of all three cell lineages along with normalization of splenic size. Partial response (PR) meant presence of hairy cells in excess of 5% in aspirates with partial response in spleen size and symptoms. Results There were 15 cases (10 M: 5F) of hairy cell leukemia (HCL), with a median age 47 years (range 32-57 years). Median duration of symptoms was eight months (range 6-14 months). [Table - 1] shows the fraction of patients presenting with various clinical manifestations. Anemia of a variable degree was present in 66% with median haemoglobin (Hb) of 8.6 g% (range of 5-12 g/dl). Median total leucocyte count was 3000/ mm 3 (range 800-17,400) and mean platelet count was 66000/mm 3 (range 30000-120000/mm 3 ). Neutropenia was the commonest presentation (80%) with pancytopenia being present in 60% cases. [Table - 1] shows the laboratory parameters of the patients. There were 14 classical and 1 variant HCL. Bone marrow biopsy was available in all cases. Biopsy was normocellular in 8/15 (53%) and hypercellular in 7/15 (47%) cases. [Table - 2] shows the immunophenotype of the patients. Immunohistochemistry was all-negative in 1 case. DBA 44 was positive in two cases where it was done. Immunophenotypic and electron microscopic findings are listed in [Table - 2]. Symptomatic improvement was seen in all patients on cladribine therapy. Eighty percent of patients obtained a CR (12 patients) remainder showed PR (3) post treatment (3 months). The three patients with PR were re-administered 2-chlorodeoxyadenosine (2-CdA) 0.1 mg/kg/d (cladribine) continuous iv infusion for another seven days; They showed complete response. Electron microscopy showed loss of the finger-like projections, as characteristic bald lymphocytes as well as loss of ribosomal lamellar complexes in all cases, which initially showed presence of these complexes. There was significant reduction in the number of mitochondria as well as vacuoles. Follow-up of all 15 patients is being done now at six-monthly interval and as on date (three-year follow-up) all are doing well with normal counts, absence of spleen and cessation of symptoms. Discussion HCL is a rare malignant disorder of the elderly. The median age at diagnosis reported is usually around 52 years. In a French study, 30 cases of HCL were diagnosed over a 25-year period; the median age was 67.8 years. [2] The median age in our series of 15 patients was 47 years, which is relatively younger. The predominant manifestions in present study were splenomegaly, fever and cytopenias. Splenomegaly was the commonest feature (100%), fever and monocytopenia were also common. However, anemia was present in a significant proportion of cases (67%). In a study from HongKong in 18 HCL cases; fever, splenomegaly and monocytopenia were the predominant manifestations [4] and 14/18 were alive at six-year follow-up. Earlier reports in Indian patients are limited. [5],[6],[7] The bone marrow biopsy has become an additional tool for assessment of prognostic factors. Increasing cellularity has been associated with worse survival. In present study, we found normal cellularity in 53% while in 47% cases it was increased. Pattern of BM involvement in HCL is pathognomic. Classically ′diffuse honeycomb′ appearance with nucleus of each HC surrounded by halo of cytoplasm (fried egg pattern) is seen. NAP score was elevated in eight patients of HCL in present series, regardless of the presence or absence of infection. With response to therapy, NAP score falls, but it rises after treatment is discontinued. NAP score parallels the hairy cell index. TRAP enzyme concentrates primarily in Golgi area and nuclear membrane. [8] TRAP and DBA 44 expression are specific for hairy cell leukemia. [9] A combined DBA 44/TRAP positivity was seen in only 3% of non-HCL non-Hodgkin lymphomas. In the present study we could pick up 14/15 (93%) cases by the TRAP test. Immunophenotyping is very useful in diagnosis of HCL. It differentiates HCL from its variants and other B cell malignancies. The CD19 and Smg positivity was seen in 14/15 (93%) and 15/15 (100%) respectively in present study. Hairy cells can be detected by flowcytometry in peripheral blood of 92% of patients, even if the hairy cells are < 1% of the lymphocytes. Specificity and sensitivity to diagnose HCL by immunohistochemistry is increased when DBA 44 is used in conjunction with 9C5 Ab and anti CD20 Ab. Electron microscopy helped us to confirm diagnosis in one TRAP negative patient, expressing typical cytoplasmic projections. Ultrastructurally the projections are elongated and slender microvilli or broad based ruffles or pseudopods are present. Frequent vacuoles, vesicles and numerous mitochondria are seen. Ribosomal lamellar (RL) complexes (50% cases) appear as rod-shaped structure under light microscopic analysis. Most of these findings were present in our patients. RL complexes are also seen in other chronic B cell lymphoproliferative disorders, acute monocytic leukemias and even non-hematologic neoplasms. The HCL variant makes up 10% of all HCL cases, as was a case in present series (1/15). It differs from typical HCL in patients being older (median age 71 years, TLC> 50 x 109/L) and the hairy cells may/may not be TRAP positive. Hairy cells show high NC ratio, more condensed chromatin and prominent nucleoli. Mitochondrial abnormalities have been seen in different cancers. Since the mitochondrial membrane potentials in cancer cells are frequently reduced in comparison with those of non-neoplastic cells this allows small molecule agents to enter the tumor cell mitochondria and reduce oxygen consumption with activation of a caspase pathway to apoptosis which is cancer cell specific. Thus targeted cancer therapy can be tried by increasing mitochondrially mediated apoptosis. The anticancer drug prodigiosin (PG) acts via mitochondrial pathway. [10] Quantification of plasma mitochondrial nucleic acids may be used to recognize patients with a poor prognosis in advanced prostate cancer. [11] Many colorectal cancers harbor mtDNA mutations that are associated with poor prognosis. [12] The mitochondrial abnormalities including the number and type of mitochondria can be detected by electron microscopy and it is an important research tool. In the present study, there was decrease in number of mitochondria following treatment. Treatment of HCL is indicated in patients with significant neutropenia, anemia, thrombocytopenia, symptomatic splenomegaly, constitutional symptoms or recurrent serious infections. [1] Most patients in present study responded to cladribine therapy. Previous studies from Mumbai have shown responses to alpha-interferon therapy. [4],[5] Pai et al , [6] found an overall response of 88.9% and disease free survival of 83% on interferon therapy. Survivals at 5 and 10 years were 34.4% and 29.6% respectively for untreated patients, 58.8% and 44.1% for patients receiving chemotherapy, steroids or other drugs, 64.1% and 56.1% for splenectomized patients and 88.9% (at 5 years) for alpha interferon (IFN)-treated patients in an Italian study. [13] However, a single dose of cladribine induces a long-term CR. Over 90% of patients are alive 13 years later and over 50% of patients appear to be clinically cured by this treatment in an Italian study. [14] The overall survival (OS) at 12 years after start of cladribine therapy was 79% in German patients. [15] The efficacy of cladribine treatment in present study is reflected in loss of the finger like projections and RL complexes, along with decrease in the mitochondria and vacuoles. Interferon treatment leads to shorter projections, disappearance of RLCs; and appearance of tubuloreticular structures (TRS) and cylindrical confronting cisternae (CCC) in 2.2% and 6.8% of the cells. [16],[17] Addition of monoclonal antibodies may lead to better responses in HCL patients. [18] Strategies for therapy in relapsed disease include retreatment with purine analog, rituximab or the anti-CD22 pseudomonas exotoxin A immunoconjugate, BL-22. [19] In Indian cases with HCL in present study, 3/15 patients with partial response showed a complete response after a repeat course of cladribine. Long-term follow-up of up to 14 years (median: 9.7 years) in a study from USA showed an excellent progression free survival and OS after 2-CdA treatment. [20] In the present series also, all 15 patients are doing well with no progression of symptoms at three years follow-up. The cost of cladribine treatment is around 80,000 to one lakh for a 70 kg adult as one vial (10 mg) costs around Rs. 11,000. Additional costs include the cost of infusion sets, overall around Rs. 1.5 lakh. In contrast the cost of the drug only for alfa-interferon (Roferon-A/Alferon) treatment over 6 months is Rs. 1.5 lakh. Thus, cladribine is a better and cheaper treatment for HCL in Indians. Acknowledgments We thank the staff at the electron microscopy facility of the institute for their help in the EM studies.References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08012t1.jpg] [cn08012t2.jpg] |
| |||||||||

{kind=link}
{kind=link}