 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
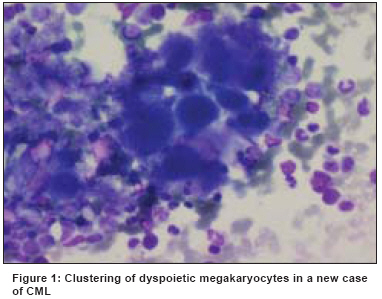
Indian Journal of Cancer, Vol. 45, No. 2, April-June, 2008, pp. 45-49 Original Article Bone marrow morphological changes in patients of chronic myeloid leukemia treated with imatinib mesylate Joshi S, Sunita P, Deshmukh C, Gujral S, Amre P, Nair CN Department of Pathology, Hemato-Oncology Laboratory and Cytogenetics Division, Tata Memorial Hospital, Mumbai Code Number: cn08013 Abstract Background: Imatinib mesylate has shown promising results in chronic myeloid leukemia (CML) in all phases. This drug is an effective treatment for patients with CML in chronic phase as it induces hematological remission in nearly all patients and cytogenetic responses in many. The bone marrow changes produced by this drug are different from the treatment modalities used earlier in CML.Materials & Methods: We studied 80 patients of CML on treatment with Imatinib at doses of 400-800 mg per day. Morphological and cytogenetic evaluation (Ph analysis) of bone marrow aspirates was done at six months of treatment. Result: In our study, 95% (76 out of 80) patients showed complete hematological response and 63.3% showed major cytogenetic response at the end of six months of treatment. The most commonly observed changes in the bone marrow aspirates at the end of six months of therapy were in the form of reduction in the cellularity, reduction in the M: E ratio to a mean of 2:1, presence of relative erythroid hyperplasia, normalization of megakaryocytic morphology and variable increase in the bone marrow lymphocytes. None of these changes had significant correlation with the patient's Ph status. Conclusion: We advise study of trephine biopsies to overcome the often-faced problem of hemodiluted aspirates in these cases and evaluation of sequential bone marrows to check the durability of these morphological changes and their correlation with the cytogenetic response with emphasis on cytogenetic changes other than Ph positivity. Keywords: Bone marrow, chronic myeloid leukemia, imatinib mesylate, morphology Introduction Chronic myeloid leukemia (CML) is a clonal stem cell disorder associated with the reciprocal translocation between chromosomes 9 and 22 resulting in formation of the bcr-abl chimeric protein with tyrosine (abl) kinase activity. [1] The enhanced tyrosine kinase activity has been associated with expansion of the pluripotent stem cells, defective adhesion and decreased apoptosis of the hematopoietic cells. [1] The effects of abl kinase activity have been found to be successfully reversed by a novel molecule STI571 or Imatinib Mesylate which specifically binds to the ATP binding site of the bcr-abl kinases and inhibits them. [2] Imatinib mesylate has shown promising results in chronic myeloid leukemia in all phases. This drug is an effective treatment for patients with CML in chronic phase as it induces hematological remission in nearly all patients and cytogenetic responses in many. [1] Its efficacy, specificity and the safety profile makes it a strong contender for the first line therapy in CML. Bone marrow aspirates in a case of CML at diagnosis typically show hypercellular marrow with marked myeloid hyperplasia and M: E ratio usually more than 10:1.The maturation arrest in the myeloid series is variable with presence of a myelocyte peak and blast percentage varies with the phase of the disease. Megakaryocytes are increased with clustering and presence of dyspoietic changes in the form of nuclear hypolobations and micromegakaryocytes [Figure - 1]. Basophils are often increased. Eosinophilia and presence of sea blue histiocytes are usual findings. Trephine biopsy may show variable reticulin fibrosis. These features are due in part to the abnormal hematopoietic differentiation mediated by bcr-abl kinase activity as well as production of PDGF by the CML cells. [1] We examined the morphological features of bone marrow aspirate samples of patients with CML who received Imatinib in order to assess the effects of bcr-abl kinase inhibition produced by this drug. We also correlated these effects with the persistence of the abnormal Ph positive clone as assessed by the conventional cytogenetic studies. Aims and Objectives
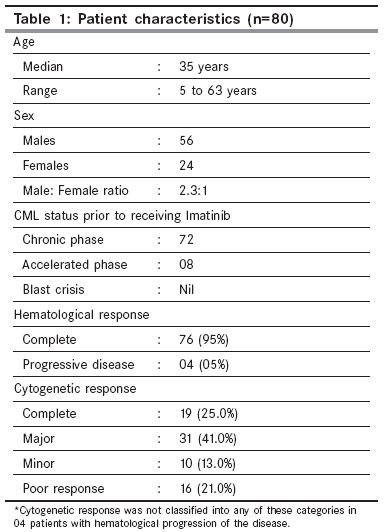
Materials and Methods A total of 80 either pre treated (with hydroxyurea or interferon) or chemo naive patients of Ph positive CML receiving Imatinib were studied retrospectively. A complete clinical data was recorded [Table - 1]. The criteria for the diagnosis of CML were:
Standard criteria were followed to determine the phase of the disease. Dosage schedule Criteria to assess response to therapy
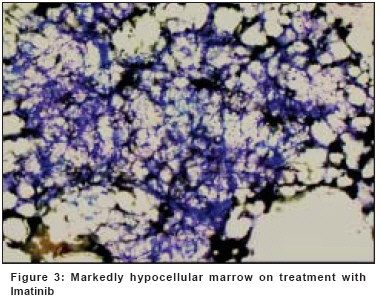
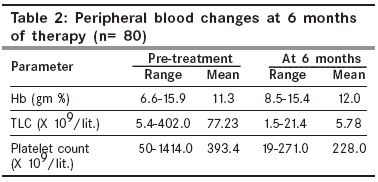
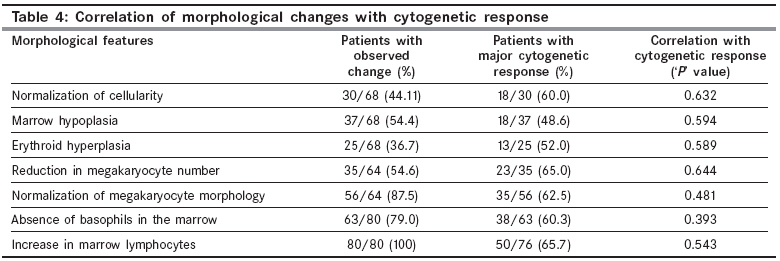
Progressive disease was defined by the increase in the blast percentage and abnormal counts. [1] Criteria for the morphological examination of the bone marrow were: All the aspiration smears were stained by Wright′s stain and independently reviewed (including 500 cell differential count) by the two pathologists. The morphological changes were noted and then correlated with the cytogenetic response. Hemodiluted smears were not considered for assessment of marrow cellularity, M: E ratio and adequacy of megakaryocytes. Adequacy of the aspirate: Presence of at least one marrow particle per smear. Cellularity: Assessed based on the patient′s age and comparison with the pretreatment marrow. Megakaryocyte number: One to three cells per low power field (10 x) were considered adequate. [3] Results 76 out of 80 patients (i.e. 95%) showed normalization of counts with disappearance of blasts from peripheral circulation at the end of six months of therapy thus indicating complete hematological remission (CHR). The manual differential count in these cases showed normalization with variable increase in the lymphocytes. The remaining four patients showed progressive disease in the form of persistently high counts with variable percentage of blasts in the blood. The most commonly observed changes in the bone marrow aspirates at the end of six months of therapy were in the form of reduction in the cellularity i.e. Normocellular [Figure - 2] or hypocellular [Figure - 3], reduction in the M: E ratio to a mean of 2:1, presence of relative erythroid hyperplasia, normalization of megakaryocytic morphology [Table - 2] and [Table - 3] and variable increase in the bone marrow lymphocytes. Apart from these findings all the aspirates showed large a number of degenerated cells, presence of sea blue histiocytes and large granular lymphocytes. 12 out of 80 aspirates (15%) were hemodiluted and hence unsuitable for assessment of marrow cellularity, M: E ratio and megakaryocyte adequacy. Although complete hematological response was associated with major cytogenetic response (Ph positivity in less than 35% of the metaphases studied) in 66% cases, no significant correlation was found between various bone marrow morphological changes and the Ph status in all the cases studied. So, morphological changes in the bone marrow aspirates of Imatinib treated patients of CML are not predictors of the cytogenetic response. Discussion Imatinib mesylate is a novel therapy which has been designed specifically against a selective target (bcr-abl tyrosine kinase). It also inhibits additional tyrosine kinases namely platelet derived growth factor (PDGF) and stem cell factor (c-kit) which might reflect the effects of this drug on non neoplastic marrow elements [4] and hence, the morphological changes which are different from those produced by therapeutic modalities used earlier like Hydroxyurea and interferon alpha which result in the normalization of peripheral counts but the marrow abnormalities persist. [2] There are very few reports in the literature describing the bone marrow morphological changes in patients of CML treated with Imatinib and their correlation with the cytogenetic response. Hasserjihan et al , have described bone marrow changes in 53 patients on Imatinib in the form of reduction in the overall marrow cellularity, M: E ratio, marrow fibrosis and megakaryocyte number and clustering. Patients in their study whose marrow showed a decrease in marrow cellularity to 50% or less were found more likely to experience a cytogenetic response ( P= 0.04 ). However, none of the other changes showed such correlation. [1] None of the morphological changes described in our study had significant correlation with the cytogenetic response [Table - 4] which implies that Imatinib affects the differentiation pattern of precursor cells expressing the bcr-abl fusion gene but may not kill the malignant clone always. This also explains the oft-seen discordance between complete hematological response and complete/major cytogenetic response and hence, raises the possibility of achieving a better synergistic effect with combination therapy. All eight patients in the accelerated phase of CML showed complete hematological remission at six months of therapy. Bone marrow changes in these patients were also similar to those observed in the patients in chronic phase before starting the therapy. Braziel et al , McNamara et al and Frater et al , have also reported that the bone marrow of Imatinib treated patients shows little or no morphologic evidence of CML beyond the first five months of therapy. [2],[5],[6] In our study, 95% (76 out of 80) of the patients were in complete hematological remission and 63.3% (50 out of 76) showed major cytogenetic response at the end of six months of treatment. The incidence of erythroid hyperplasia (25 out of 68 i.e. 36.7%) was lower in our study and this change as an indicator of myelosuppression was not found to have any adverse effect on the cytogenetic response. Sneed et al , have described it as an independent poor prognostic factor for achieving the cytogenetic response. [7] Increase in the lymphocytes in the peripheral blood as well as bone marrow of the patients of CML treated with Imatinib has not been reported in any of the studies mentioned above. All the 80 patients in our study showed increase in marrow lymphocytes in the range of 12 to 75% with a median of 30%. We also noted that this increase in the lymphocytes was absolute, definitely related to the therapy and did not correlate with the Ph status. The exact mechanism for this increase in the lymphocytes is not known. However, since this is a consistent finding, detailed immunological studies are needed to study their role in the tumor immunity. Various bone marrow changes described in our study can be related to the action of Imatinib on the Ph positive as well as Ph negative marrow elements irrespective of the cytogenetic response in these patients. In addition, longterm action of this drug on the bone marrow stem cells may give rise to additional chromosomal alterations as observed with other chemotherapeutic agents need to be studied every time along with the Ph status evaluation. [8],[9] Study of trephine biopsies is essential in all the cases to overcome the often faced problem of hemodiluted aspirates and is also needed for better assessment of marrow cellularity, M: E ratio and megakaryocyte adequacy and morphology. We also emphasize a need for study of sequential marrows to check the durability of the morphological changes and their correlation with drug resistance, disease relapse and clonal evolution. As Imatinib Mesylate is a commonly used drug in all phases of CML, it is essential for all the hematologists to be aware of the morphological changes produced by this drug. References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08013t1.jpg] [cn08013t2.jpg] [cn08013f3.jpg] [cn08013t4.jpg] [cn08013t3.jpg] [cn08013f1.jpg] [cn08013f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}