 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
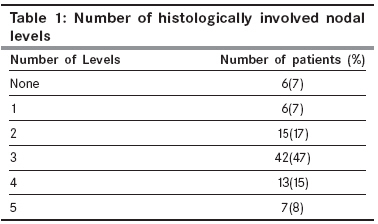
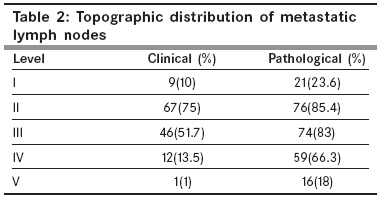
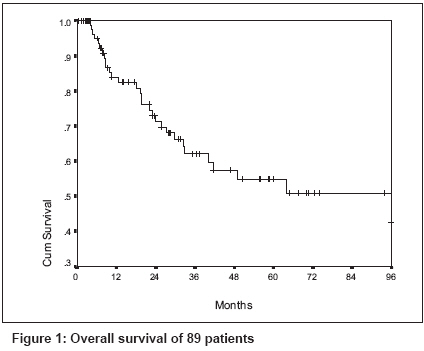
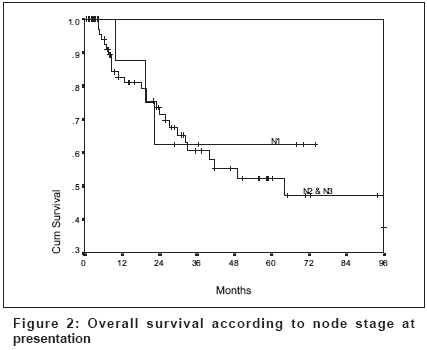
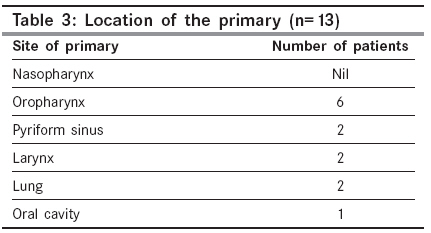
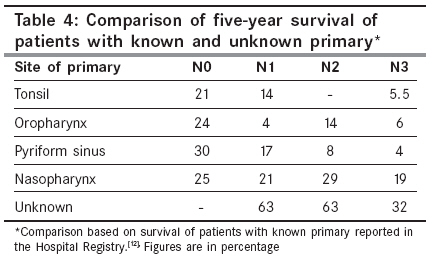
Indian Journal of Cancer, Vol. 45, No. 2, April-June, 2008, pp. 54-58 Original Article Cervical lymph node metastases of squamous cell carcinoma from an unknown primary: Outcomes and patterns of failure Mistry RC, Qureshi SS, Talole SD, Deshmukh S Department of Head and Neck Services, Tata Memorial Hospital, Ernest Borges Road, Parel, Mumbai Code Number: cn08015 Abstract Context: Management of cervical lymph nodes metastases of squamous cell carcinoma (SCC) from primary of unknown origin (PUO) is contentious and there is insignificant data from India on this subject.Aims: To present experience of management of these patients treated with curative intent at a single institution. Settings and Design: Retrospective study of patients treated between 1989-1994 in a tertiary referral cancer centre. Materials and Methods: Eighty-nine patients were evaluated in the study period and their survival compared with patients with common sites of primary in the head and neck with comparable node stage. Statistical analysis used: Kaplan-Meier method. Results: The clinical stage of the neck nodes at presentation was N1 in 11%, N2a in 28.5%, N2b in 22.5%, N3 in 35% and Nx in 3.4% patients. All patients underwent surgery and 70 patients received more than 40Gy postoperative radiotherapy. Twenty-nine (32.6%) patients had relapse of which 19 (21%) were in the neck. Postoperative radiotherapy did not influence the neck relapse (p=0.72). Primary was detected in 13 patients (14.6%) on subsequent follow up. The overall five and eight-years survival was 55% and 51% respectively. The overall five-year survival was better compared to patients with known primary with comparable node stage. Conclusions: Patients with cervical lymph nodes metastases of SCC from PUO have reasonable survival and low rate of development of subsequent primary when treated with surgery and radiotherapy. The overall survival is comparable to that of patients with known primary and hence an attempt at cure should always be made. Keywords: Cervical metastases, head and neck, squamous cell carcinoma, unknown primary Introduction Metastases of squamous cell carcinoma (SCC) to cervical lymph nodes from primary of unknown origin (PUO) represent 1% to 2% of head and neck cancers. [1],[2],[3] The explanations for this unusual form of presentation are of speculative nature: spontaneous regression of the primary and inability to detect a small primary particularly in the nasopharynx, which is known to metastasize to nodes at an early stage. Unlike metastatic lymph nodes from PUO at other body sites, the prognosis in metastatic cervical nodes is not discouraging. The five-year overall survival rates range between 40% to 60% in recent series. [3],[4],[5],[6],[7] However, the optimal management of these patients remains controversial. The lack of randomized studies comparing treatment options has led to therapeutic decision based on retrospective non-randomized studies involving patients managed with various diagnostic and therapeutic procedures and institutional policies. [2],[4],[5],[8],[9] Although sufficient data exist in the literature on the subject, reports from India are deficient. [10] The paper presents the experience at the Tata Memorial Hospital with treatment of patients with SCC metastatic to cervical lymph nodes from PUO. Materials and Methods The study included 89 patients with metastases of SCC to cervical lymph nodes from PUO treated with curative intent between 1989 to 1994. The study excluded patients who received palliative therapy because of advanced or comorbid disease, with histology other than SCC and distant metastases at the time of diagnosis. The median age of patients was 55 years (range 28 to 84 years). There were 78 men and 11 women. Forty-six patients had involvement of right sided cervical nodes and 43 had left sided nodes. The frequency of metastatic lymph nodes at various neck levels were as follows: level 1, 9 patients (10%); level 2, 67 patients (75%); level 3, 46 patients (51.7%); level 4, 12 patients (13.5%); level 5, 1 patient (1%). All patients were staged according to the 2002 American Joint Committee on Cancer (AJCC) system for nodal disease in the head and neck region. [11] The clinical stage of the neck at presentation was N1 in 10 patients (11%), N2a in 25 patients (28.5%), N2b in 20 patients (22.5%), N3 in 31 patients (35%) and Nx in 3 patients (3.4%). The diagnosis of SCC in neck nodes was confirmed by FNAC in 50 patients (56%) and by open biopsy performed elsewhere in 39 patients (44%). The provisional diagnosis of neck node metastases with unknown primary was made after a comprehensive clinical examination of the upper aerodigestive tract failed to detect a primary lesion. All patients underwent chest X-ray, barium swallow, X-ray of the nasopharynx and paranasal sinuses. Computerized Tomography (CT) was performed as a routine in the later years of the study. Subsequently patients underwent a meticulous examination under anesthesia with panendoscopy (direct laryngoscopy, oesophagoscopy, nasopharyngoscopy and bronchoscopy) and palpation of nasopharynx and base of tongue. Random biopsies and washings for cytology from tonsil, base of tongue and/or nasopharynx was not performed. If these investigations failed to reveal the primary tumor, diagnosis of cervical node metastases from PUO was established. All patients underwent neck dissection and were advised postoperative RT. Ten patients did not take RT and nine patients did not complete RT for various reasons. Thus 19 patients (21%) had none or less than 40 Gy and the remaining 70 patients (79%) had 40 Gy or more of postoperative RT. The RT portals were unilateral, bilateral or antero-posterior depending on the discretion of the treating radiotherapist. Patients were followed-up at regular interval; endoscopy and/or imaging were performed if patient was symptomatic or clinical examination raised suspicion of primary. Follow-up were completed by letters, telephone calls and home visits. The survival was measured from the date of diagnosis to the last day of follow-up or to death. The data was analyzed using SPSS for windows version 11.5 statistical software. Survival was computed by the Kaplan-Meier method and compared by log-rank testing. Results In six (7%) patients none of the nodes were metastatic; all of them had open biopsy before neck dissection. In six (7%) patients nodes were involved at a single level and in seven (8%) patients, nodes were involved at all levels in the neck [Table - 1]. Details of the level at which nodes where involved is listed in [Table - 2]. Extra nodal disease was reported in 59(66%) patients. Fifty-one patients were alive at the time of review. Ten patients died due to recurrent disease, ten died of subsequent primary, nine patients died of distant metastases, one patient had recurrent disease and distant metastases and in eight patients the cause of death was not known. The five and eight-year overall survival for all patients was 55% and 51% respectively, with median survival of 98 months [Figure - 1]. Patient with N1 neck stage at presentation showed a trend towards better survival as compared to N2 and N3 together at 30 months [Figure - 2], although this was not statistically significant ( P =0.16). Similarly extra nodal spread also showed a weak evidence of having an impact on survival (P= 0.07). However, postoperative radiotherapy, prior open biopsy of the node and involvement of nodes at multiple levels in the neck did not have any impact on the survival. Twenty-nine patients (32.6%) had relapse of disease. The site of relapse was neck in 19 patients (21.3%), distant in nine (10%) patients and neck with distant failure in one patient. Four of the 19 patients (21%) who received less than 40 Gy postoperative RT and 15 of 60 (25%) patients who received more than 40 Gy of post-operative RT developed a neck relapse (P= 0.72). Only three of the 29 patient with relapse of disease were alive. The primary was detected in 13 patients (14.6%) on follow-up. Two of these patients received less than 40 Gy and 11 had more than 40 Gy of RT. The mean time to detection of the primary was 24 months. In two patients, the primary was detected in less than a year and could represent missed primaries. The commonest site of the primary was oropharynx; none presented with primary in nasopharynx [Table - 3]. All, except three with primary in hypopharynx, larynx and oral cavity, died of disease. The survival of patients with known primary site treated in Tata Memorial Hospital is reported in the Hospital Registry. [12] The five-year survival of patients with common sites of primary in the head and neck area was compared with the patients reported in this study. For comparable node stage the overall survival was better for patients with unknown primary [Table - 4]. Discussion The diagnosis of cervical node metastases from PUO is made after thorough assessment fails to reveal the presence of tumor in the upper aerodigestive tract. In addition to the array of investigations, many reports have advocated tonsillectomy, blind biopsies and/or washings for cytology from nasopharynx, and base tongue. [1],[13],[14],[15] However, none of the patients reported in this study underwent routine blind biopsies and yet the rate of detection of primary on subsequent follow-up was no higher than reported in the literature, thus questioning the role of these investigations in the work up for PUO. Similar conclusion can be drawn for CT scan. In gastrointestinal cancers CT is considered to be less sensitive in identifying small peritoneal deposits and superficial liver metastases. Hence the importance of laparoscopy, wherein there is direct visualization of the abdominal cavity is substantial. [16] Akin to this in cervical metastases from PUO, the primary, if there is one, is likely to be small the best investigation would be thorough examination of all the mucosal areas in the upper aerodigestive tract rather than relying on CT scan which is not ideal for detecting small lesions. Hence we believe that imaging of the neck, if performed, should be to define the extent of nodal disease and its resectability rather than search for a primary. However, Sinnathamby et al and other authors recommend routine imaging so as to avoid missing an occult primary and unnecessary radiation to mucosal areas. [2] Lately newly introduced diagnostic methods have also been endeavored. Fluorodeoxyglucose (FDG) positron emission tomography (PET) or single-photon-emission computed tomography (SPECT) have been utilized. However, limited data has suggested that they are useful only in small subsets of patients. [1],[14],[15],[17] Laser-induced fluorescence imaging, Epstein-Barr virus (EBV) evaluation in metastatic lymph nodes by in situ hybridization, Human papilloma virus (HPV) detection by polymerase chain reaction, microsatellite mutation analysis of metastatic nodal tissue and samples of normal pharyngeal mucosa were also proposed. [18],[19],[21] The management of patients with cervical metastases from PUO evokes considerable controversy and has not been standardized. Nieder et al , [1] in their review have suggested surgery alone in selected patients with N1 disease without extracapsular extension and with no history of incisional or excisional biopsy based on their finding of an appearance rate of the primary tumor of 25%, median nodal recurrence rate of 34% and overall five-year survival rate of 66%. The application of RT has ranged from RT alone to postoperative RT and the portals included spanned from ipsilateral neck nodes to bilateral neck nodes and the putative primary sites. [2],[3],[4],[5],[6],[7],[22] There is evidence that patients receiving postoperative RT to bilateral neck nodes and potential primary sites have higher reported control odds and survival rate than patients receiving postoperative ipsilateral RT or RT alone. [5] Nevertheless, considering the lack of comparative studies, the optimal radiotherapy strategy remains to be delineated. Similarly, the role of chemotherapy in the management of PUO with cervical metastases is also indistinct. In fact, in the review by Nieder et al , [1] substantial data supporting the use of chemotherapy was deficient. The incidence of subsequent primary in our series (15%) is in agreement with incidence reported by other studies where postoperative RT was routinely administered. [1],[4],[5],[6],[7],[22] We did not include any patient with metastases of undifferentiated carcinoma in the study. This could explain why none of the primary was found in the nasopharynx. As reported in the literature, patients in whom primary was detected later did poorly as compared to those who continued to be free of disease. [5],[14] Postoperative RT did not help in controlling the disease in the neck for 21% patients who had less than 40 Grays versus 25% in those who had 40 Grays or more of radiation (P= 0.72). This is contrary to the experience at the Memorial Sloan Kettering Hospital where postoperative radiation failed to influence the overall survival but helped in improving the local control. [23] Iganej also described a similar experience with postoperative RT. [7] Numerous factors have been recognized influencing the overall survival including node stage, number of histologically involved nodes, grading, presence of extra nodal disease and performance status. [1],[2],[3],[4],[24] In our study presence of extra capsular disease had a minor impact on survival and nodal stage at presentation showed a trend towards better survival although it did not achieve statistical significance. None of the other factors studied (open node biopsy, presence of metastatic nodes at multiple levels, tumor grade and postoperative radiotherapy) had impact on the overall survival. The five-year survival of 55% is comparable to published results. [3],[5],[6],[23],[24],[25] We compared the overall survival of these patients with that of patients with known primary at common sites in the head and neck region as reported in the hospital registry. [12] For comparable node stage, patients with occult primary appear to fare better than patients with known primary. This observation should be interpreted with caution as the comparison is with historical data. Jones et al , on similar comparison did not find any difference in the survival between the two groups. [26] The limitation of this study is its retrospective nature. However all the patients had similar histology and treatment was uniform in all patients. Based on this, it appears that routine blind biopsies from upper aerodigestive tract may not be necessary. Nodal stage at presentation and extra capsular disease has a role in outcome of these patients. In conclusion, the optimal diagnostic and therapeutic approach still eludes us. The first randomized trial proposed by the European Organization for Research on Treatment of Cancer (EORTC), Radiation Therapy Oncology Group (RTOG), and other cooperative groups from Australia, Canada, Denmark and Germany (study 24001-22005) is ongoing. [1],[14] The results of this trial will help in expounding several questions regarding passable management of cervical metastases from PUO References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08015t4.jpg] [cn08015t2.jpg] [cn08015f2.jpg] [cn08015t3.jpg] [cn08015t1.jpg] [cn08015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}