 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
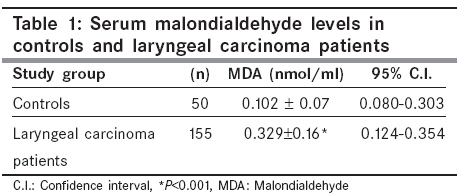
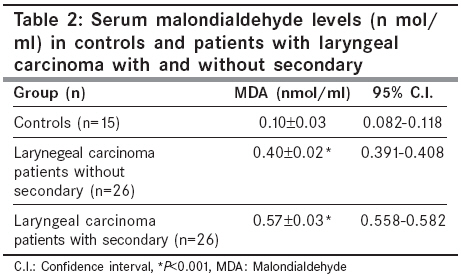
Indian Journal of Cancer, Vol. 45, No. 3, July-September, 2008, pp. 97-99 Original Article Oxidative stress in patients with laryngeal carcinoma Dwivedi RC, Raturi DP, Kandpal N, Dwivedi RC, Singh RP, Puri VN Department of Otorhinolaryngology, K.G.M.U., Lucknow, India; Head-Neck Unit, Royal Marsden Hospital, Fulham Road, London, SW3 6JJ, UK Code Number: cn08031 Abstract Background : Cancer is a multifactorial disease. Repetitive cumulative damage of cellular organelles by oxy-free radicals are few of the important causative factors.Aim : To assess the role of oxidative stress in the laryngeal cancer patients in Indian population. Setting and Design : Case control study. Materials and Methods : Level of malondialdehyde (MDA) as a marker of oxidative stress was examined in large cohort of control (50) and laryngeal carcinoma patients (155) from North India. Both the controls and laryngeal carcinoma patients were smokers. Results : In control healthy subjects MDA levels were 0.102±0.07 (0.080- 0.303, 95% CI) n mol/ml, as compared to 0.329±0.16 (0.124-0.354, 95% CI) n mol/ml in the cases of laryngeal carcinoma patients. Three times higher serum MDA levels indicated that there was significant oxidative stress in the subjects having laryngeal carcinoma lesions. In addition patients with secondaries were having MDA levels of 0.4±0.02 (0.391-0.408 95% CI) n mol/ml, as compared to 0.57±0.03 (0.558-0.582 95% CI)n mol/ml in group of patients without secondaries. These two values were statistically significant as compared to control values (P<0.01). Conclusion : These findings suggest that in case of laryngeal carcinoma patients, there is increase in the level of oxidative enzyme MDA. The oxidative stress might be due to the modulation of pro-oxidant or anti-oxidant systems in laryngeal carcinoma. Keywords: Laryngeal carcinoma, malondialdehyde, oxidative stress Introduction More than 5,00,000 new cases of head and neck cancers including laryngeal carcinoma are reported annually worldwide. Oxidative stress involvement in several types of cancers and cardiovascular diseases has been reported from several countries around the globe. [1],[2],[3],[4],[5],[6],[7],[8] Laryngeal cancer in Indian population is among one of the highest reported in Asian sub continent. [9] Free radicals and excess of electrons are known to modulate cell membrane and nuclear reactions inside the living cells. Cancerous cells have been shown to express higher activity, resulting in rapid growth of cells. Pro-oxidants are known to modulate pro-oxidant genes, which are related to cell growth and differentiation. These changes lead to changes in DNA structure, which initiate and maintain carcinogenic process even in cases of laryngeal cancers. [10] Several nutrients and environmental factors are shown to be involved in the initiation and progression of cancers. In Indian subjects it has been reported that vitamin A levels are lowered in patients of laryngeal carcinoma as compared to controls. [11] In our institution, similar kind of observations have been made in North Indian subjects. In addition we have also reported higher angiogenic activity in these patients. [5] Taysi et al, have reported that oxidative stress is increased in advanced laryngeal cancer patients. [4] Materials and Methods Patients attending the out-patients department of Otorhiolaryngology and head and neck surgery and/ or those, admitted in the surgical/ medical wards with histopathologically proven laryngeal cancer were included in this study. Approval of this project proposal was obtained from the ethics committee of the medical school. Present study included control group (n=50), 41 males and 9 females with men age of 49±4.4 years. Patients group consisted of (n=155) patients of laryngeal carcinoma, 128 males and 27 females with mean age of 53±6.9 years. Controls as well as laryngeal carcinoma patients were smokers. In men in controls and laryngeal cancer subjects there was positive history of tobacco chewing or smoking or both for more than 20 years. Five women in both the groups were also reported addicted to smoking Beedis (15-20/day) or chewing tobacco for over 20 years. All the patients were from north Indian cities and their nutrition history was approximately the same. Hemoglobin, blood sugar and blood urea in controls and study groups were done by standard methods. Patients with associated illness (hypertension, myocardial infraction, renal, hepatic, pancreatic and pulmonary diseases), which are known to alter the reactive oxygen species were excluded from study. Patients were staged and classified as described in TNM classification (UICC). From this chart we made 2 groups of patients. [12] Laryngeal carcinoma with nodal involvement (with secondary) and those without nodal involvement (without secondary), 26 patients were included in the either group. Estimation of MDA Statistical analysis Results Fifty control subjects (41 males and 9 females) with mean age 49±4.4 years and one hundred and 55 laryngeal carcinoma patients (128 males and 27 females) were included in this study. Eighty eight percent male patients were addicted to tobacco (Beedi, cigarette) for 20 years or more, while 12% male were not addicted. Female patients were not addicted except two females who smoked Hukka, Beedis and tobacco for the last 20 years. Control subjects were also addicted to similar type of tobacco products for 20 years or more. Control and patients groups were either vegetarian or non-vegetarian. Caloric intake in control subjects was about 2400 calories while in patients group it varied from 1200 to 1600 calories. In 50 control subjects serum MDA levels were 0.102±0.07 nmol/ml, with 95% CI.(0.080-0.303) while MDA levels were three times higher 0.329±0.16 nmol/ml with 95% CI.(0.124-0.354), in the patients with carcinoma of larynx, the difference between the two groups was statistically highly significant ( P < 0.001) [Table - 1]. In two groups of patients (n=26) without secondary and with secondary according to TNM classification were included in this study. Serum MDA levels in control and Laryngeal Carcinoma patients are shown in the [Table - 2]. In control subjects serum MDA levels were 0.10±0.03 nmol/ml with 95% CI. (0.082-0.118) while there times higher levels were found in laryngeal carcinoma patients without secondaries 0.40±0.02 nmol/ml with 95% CI. (0.391-0.408), the differences between control and laryngeal carcinoma patients were statistically highly significant ( P < 0.001). However, serum MDA levels in patients with secondaries were 0.57±0.03 nmol/ml with 95% CI. (0.558-0.582) and values were statistically highly significant when compared with values observed in control subjects ( P < 0.001). Discussion The TNM (Tumor, Node, Metastasis) classification of laryngeal carcinoma integrates clinical presentation including that obtained by pathology, endoscopy and radiological evaluation in our cohort. Increased production of reactive oxygen species (ROS) has been reported in different cancers in several studies. [2],[3],[4],[5],[6],[7],[8] Increased levels of ROS could be due to increased production or reduced activity of antioxidant enzymes (Glutathione & catalase). In laryngeal carcinoma it has not been worked out as yet that which is the first stage and how the molecular events get started. In most of the studies malondialdehyde as a marker of ROS, has been measured, so as to conclude their involvement in laryngeal cancers. In our previous study in small number of patients, increased serum MDA level were observed. From this study where we have large cohort it is once again confirmed that MDA levels are higher in Laryngeal carcinoma patients probably for the first time. We have observed that laryngeal carcinoma patients have lower levels of anti oxidant (Vit A), suggesting that higher MDA levels could be due to decreased activity of anti oxidant system. However, no of patients included in our study were small so there is need to expand such studies in bigger cohort. [5] We separated two group of patients one with nodal involvement and the other one without the secondaries. It was observed that there was not significant difference in the two groups. These findings suggest that ROS starts up regulating during the process of tumor initiation. It will be interesting to have continuous studies with different stages of cell cycle and ROS production. We do not have any study to show the role of antioxidant in the treatment of laryngeal carcinoma patients. However, several studies have shown that beta carotene has a curative effect on different cancers. [14] Beta carotene, vitamin A and other vitamins like C and E have antioxidant activity, therefore it has been reported from international studies in the cancer that retinoids have cancer preventing capabilities. [14],[15],[16] Tumor invasion, metastasis and angiogenesis are the important events in carcinogenesis and how antioxidants modulate these processes still needs to be explored in detail. Now even in our previous study we reported that serum Angiotensin Converting Enzyme (ACE) activity is enhanced in cases of laryngeal carcinoma suggesting that renin angiotensin peptides might also be playing some important role in angiogenic process of tumor progression. [5] We have already started clinical trials with ACE inhibitors in our laryngeal carcinoma patients and the results are eagerly awaited. Tobacco consumption in various forms by oral intake or inhalation is the strong exogenous source for the generation of ROS. Oxidative stress activates the production of procarcinogenic compounds ex. Benzopyrenes. In addition these reactants also damage the cellular DNA Pryor. [17] It could be concluded that these factors are operative in initiation of laryngeal carcinoma in our cohort. It will be very interesting to address the many questions related to the area of mutagenesis and biomarkers. It thus concluded that patient of laryngeal carcinoma from Northern India have increased burden of reactive oxygen species. However, mechanism related to oxidant stress and antioxidant system remains to be clarified. Acknowledgments The authors would like to thank Dr. Namita Kanwar, Dr. Sumit Kumar and Dr. Ehtesham Siddiqui for their support in manuscript preparation.References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08031t1.jpg] [cn08031t2.jpg] |
| |||||||||


{kind=link}
{kind=link}