 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
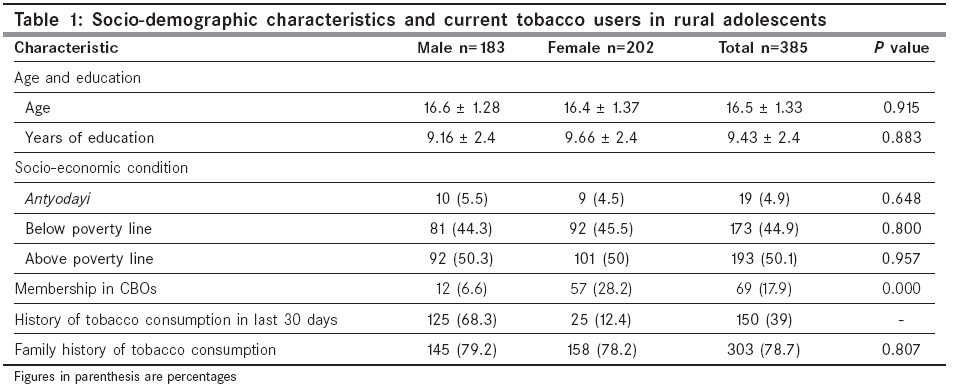
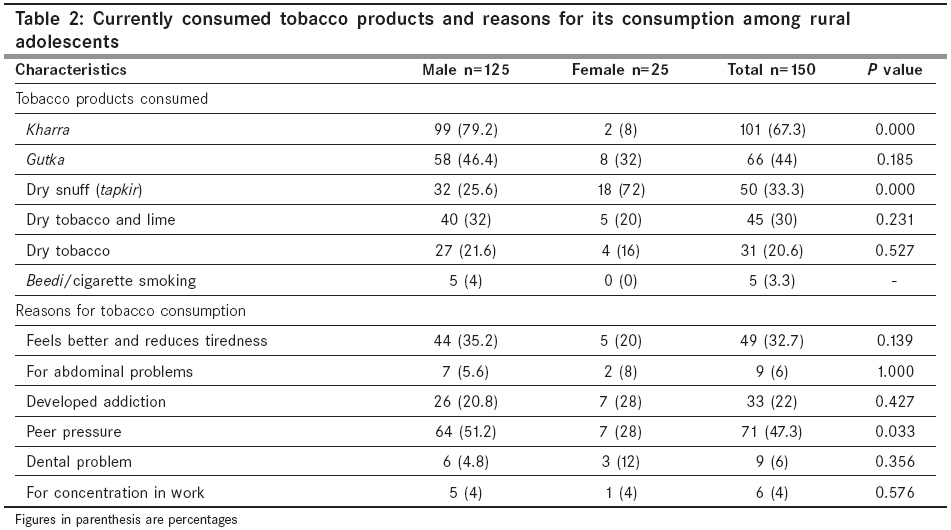
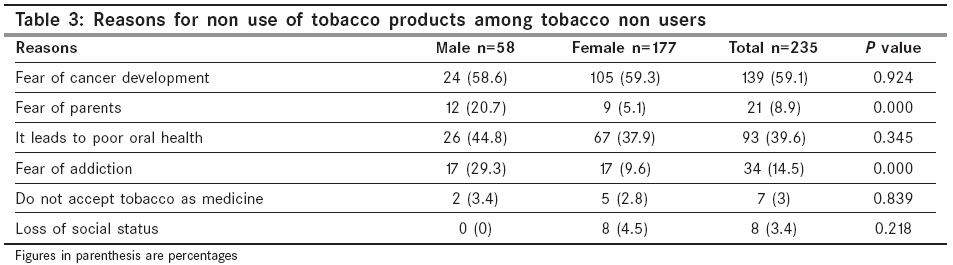
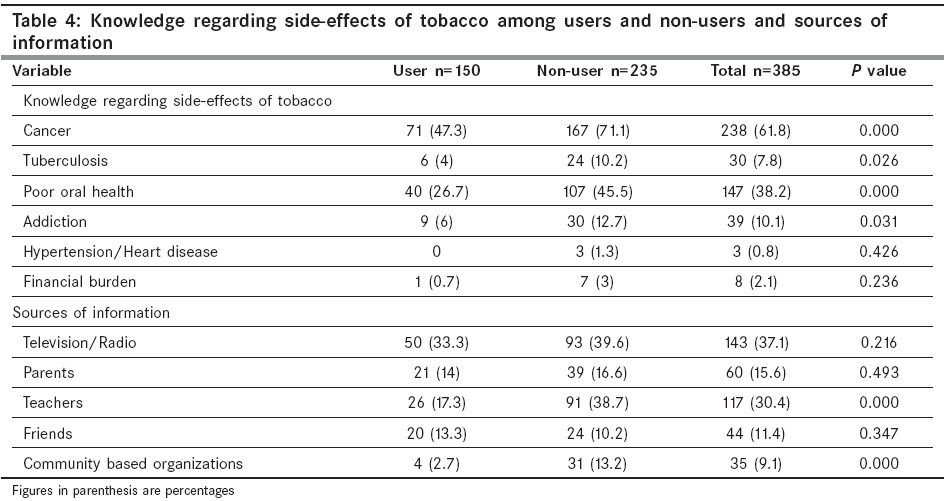
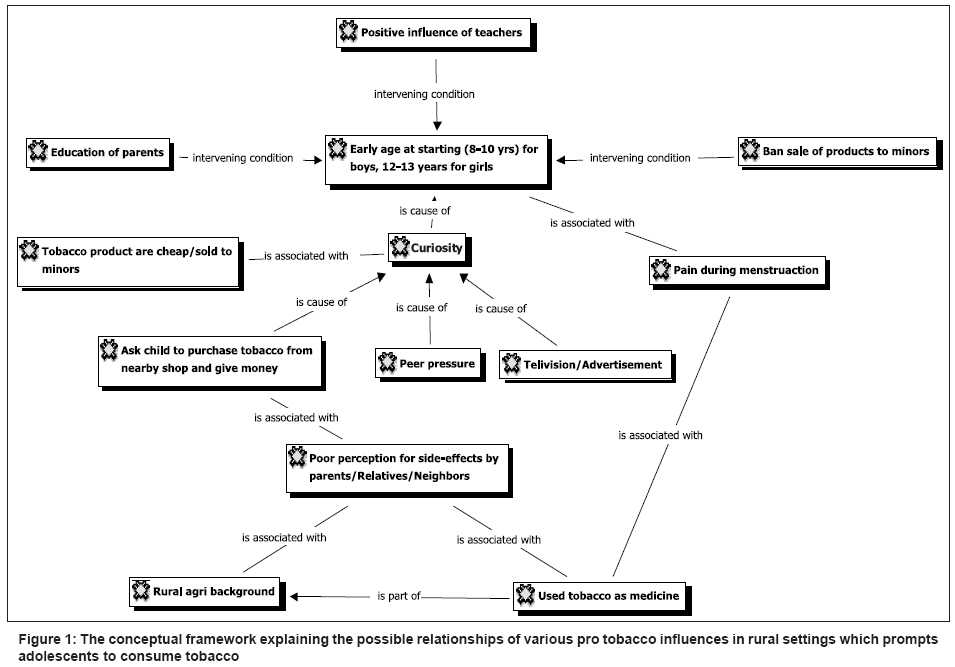
Indian Journal of Cancer, Vol. 45, No. 3, July-September, 2008, pp. 100-106 Original Article Tobacco consumption among adolescents in rural Wardha: Where and how tobacco control should focus its attention? Dongre AR, Deshmukh PR, Murali N, Garg BS Dr. Sushila Nayar School of Public Health, Mahatma Gandhi Institute of Medical Sciences, Sewagram - 442 102 Code Number: cn08032 Abstract Objectives: The objectives of the present study were to study the pattern of tobacco use among rural adolescents (15-19 years) and to find out reasons for use and non use of tobacco products.Materials and Methods : In the present community-based research, triangulation of qualitative (free list, focus group discussions) and quantitative methods (survey) was undertaken. The study was carried out in surrounding 11 villages of the Kasturba Rural Health Training Centre, Anji during January 2008 where 385 adolescents were selected by simple random sampling and interviewed by house to house visits. After survey, six focus group discussions were undertaken with adolescent boys. Results: About 68.3% boys and 12.4% girls had consumed any tobacco products in last 30 days. Out of boys who had consumed tobacco, 79.2% consumed kharra, and 46.4% consumed gutka. Among boys, 51.2% consumed it due to peer pressure, 35.2% consumed tobacco as they felt better, and five percent consumed tobacco to ease abdominal complaints and dental problem. Among girls, 72% used dry snuff for teeth cleaning, 32% and 20% consumed tobacco in the form of gutka and tobacco & lime respectively. The reasons for non use of tobacco among girls were fear of cancer (59%), poor oral health (37.9%). Among non consuming boys it was fear of cancer (58.6%), poor oral health (44.8%) and fear of getting addiction (29.3%). According to FGD respondents, few adolescent boys taste tobacco by 8-10 years of age, while girls do it by 12-13 years. Peer pressure acts as a pro tobacco influence among boys who are outgoing and spend more time with their friends. They prefer to consume freshly prepared kharra which was supposed to be less strong (tej) than gutka. Tobacco is being used in treatment of some health problems. Tobacco is chewed after meals for better digestion, given to ease toothache, pain in abdomen and to induce vomiting in suicidal insecticide poisoning. Conclusion: The current consumption of any tobacco products among rural adolescents was found very high. Hence, the multi-pronged intervention strategy is needed to tackle the problem. Keywords: Adolescents, India, medicinal properties, rural setting, tobacco product use Introduction Addictions developed in adolescence are likely to persist into adult life. Presently, adolescents are increasingly exposed to changing lifestyles that have very negative impact on health. Neither parents nor the community have any clue how to deal with such situations. [1] According to Global Youth Tobacco Survey (GYTS) in Maharashtra, 12.9% adolescents (13-15 years) currently consumed any tobacco products. [2] The most susceptible time for tobacco use in India is during adolescence and early adulthood (15-24 years). [3] Hence, an innovative community-based intervention for reducing primary uptake of tobacco among adolescent (15-19 years) is one of the prioritized research questions. [4] Reasons for tobacco use are fairly clear, but reasons for non-use have not yet been studied. [5] The theme for ′World No Tobacco Day-2008′- Tobacco Free Youth focuses on adolescents and called for formation of youth groups and awareness building. [6] There is a need for locally relevant community based data regarding tobacco use pattern among adolescents, their perceptions and behaviors for designing effective community based intervention strategy. Hence, the objectives of the present study were to generate community based data on tobacco use pattern among rural adolescents (15-19 years) and to find out reasons for use and non use of tobacco products.Materials and Methods Study setting and study subjects: The present community based triangulated research of qualitative (free list and focus group discussions) [7] and quantitative (survey) methods was undertaken in surrounding 11 field practice villages of the Kasturba Rural Health Training Centre (KRHTC), Anji, which is a peripheral centre of Dr. Sushila Nayar School of Public Health, Mahatma Gandhi Institute of Medical Sciences (MGIMS), Sewagram. The total population of 11 villages was 14,708 with 10.5% of adolescent population in 15-19 years age group. The study was undertaken during January 2008 among rural adolescents (15 -19 years). Pre survey qualitative assessment: The various socio-cultural factors that may impact on consumption of tobacco-related products among adolescents were assessed by qualitative methods as our pre-understanding on underlying dynamics in rural settings was limited. The free listing exercise was undertaken with purposively selected key informants (n=10) for exploring locally available tobacco products and various reasons for its use and non use. The analysis of free listing exercise was useful for questionnaire development and deciding the domains of focus group discussions (FGDs). The analysis of free list exercise was undertaken using Anthropac 4.98.1/X software. [8] The findings of qualitative assessment and the GYTS [2] questionnaire were used for development of locally relevant structured questionnaire for the present study. Quantitative assessment (Survey): Assuming the rough estimate of rural adolescents′ proportion, for knowledge and practices of study variables as 0.5, 95% confidence interval and 5% precision, the minimum sample size required was 384. It was further inflated by 10% to cover non-response and thus 420 adolescents (15-19 years) were to be covered. A detailed house listing exercise among all the study villages provided the sampling frame. Finally, the sample was drawn by simple random sampling from enlisted 1,544 adolescents (15-19 years). A team of trained medical personnel interviewed 385 adolescents (92% response rate) using pre-designed and pre-tested questionnaire by paying house to house visits. The interviewer showed the photograph of locally available tobacco products to the respondents while asking its history of consumption in last 30 days. The color of the ration card was considered as an indicator of socio-economic status. Yellow card signified families below poverty line status and Antyodayi signified poorest of the poor. The concept of Community based Organization (CBO) like ′ Kishori Panchayat′ (KP, forum of adolescent girls) mentioned in the study has been reported and explained elsewhere. [9] The data entry and analysis was done by using Epi_info 6.0 software package. Post survey qualitative assessment (Focus group discussions, FGDs): After obtaining informed consent, six FGDs were undertaken with the group (6 to 8 participants) of purposively selected adolescent boys from different socio-economic strata, who are willing to participate and talk freely. The number of FGDs was decided by the saturation point i.e. where it stopped yielding new information. The trained moderator, after obtaining informed consent, facilitated FGDs using structured guidelines and note taker audio recorded it and then transcribed it. The separate consent was obtained from all the participants before audio recording the discussion. The hermeneutic units were created for text data of FGDs. The textual level analysis included activities like segmenting and organizing data files and coding data segments, while the conceptual level (model building activity) focused on activities such as linking codes to form semantic networks. This qualitative content analysis of textual and conceptual level of FGD data was undertaken using Atlas.ti.5.0 software package. [10] The FGD findings were used to bridge gaps in information and develop a conceptual framework explaining the possible underlying complex phenomenon in rural settings which motivates adolescents to consume tobacco. Results Out of 385 adolescents (15-19 years) interviewed, 183 (47.5%) were male and 202 (52.5%) were female. The mean age (± standard error) of male adolescents was 16.6 ± 1.28 years and that of adolescent girls it was 16.4 ± 1.37 years. Only two percent adolescents were illiterate. Overall, 49.8% adolescents were below poverty line. Significantly higher proportion of adolescent girls (28.2%) were members in community based organization like KP as compared to adolescent boys′ (6.6%) membership in CBO ( P =0.000). About 68.3% boys and 12.4% girls had consumed any tobacco products in last 30 days ( P =0.000). Overall, 39% adolescents had consumed any tobacco products in last one month. About 78.7% adolescents had history of tobacco products consumption in their family [Table - 1]. Out of 125 boys (68.3%) who had consumed any tobacco products in last one month, 79.2% consumed kharra, 46.4% and 32% consumed gutka and khaini respectively. About 25.6% used dry snuff ( nus ) for teeth cleaning. Only four percent smoked tobacco in the form of beedi/cigarette. Among tobacco user boys, 51.2% consumed it due to peer pressure, 35.2% consumed as they felt better, 20.8% were reported as addicted to it and 5% boys consumed tobacco for abdominal complaints and dental problem. Out of 25 (12.4%) adolescent girls who had consumed tobacco, 72% used dry snuff ( nus ) for teeth cleaning, 32% and 20% consumed tobacco in the form of gutka and khaini respectively. Among tobacco user girls, 28% did so due to peer pressure or developed addiction to it and 20% girls felt better due to its consumption. Significantly more boys consumed kharra (mawa) and girls consumed dry snuff ( nus ) and boys had more peer pressure than girls ( P =0.000). Overall 47.3% adolescents consumed tobacco products due to peer pressure and 32.7% felt well due to its consumption. Significantly more boys experienced peer pressure than girls ( P =0.033) [Table - 2]. Out of 235 adolescents, who did not consume tobacco, 177 (75.3%) were girls and 58 (24.7%) were boys. The reasons for non use of tobacco among girls were fear of cancer (59%), poor oral health (37.9%). Among non consuming boys it was fear of cancer (58.6%) poor oral health (44.8%) and fear of getting addiction (29.3%). Only three percent did not accept tobacco as medicine for pain in abdomen, toothache and wound dressing etc. Significantly more non user boys had fear of parents and development of addiction as compared with girls ( P =0.000) [Table - 3]. [Table - 4] shows knowledge regarding side-effects of tobacco consumption among tobacco users and non-users and its source of information. Significantly more non-users knew that it causes cancer, tuberculosis, poor oral health and development of addiction. The major sources of information for non-users were school teachers and community-based organizations. ( P =0.000). Overall, their major sources of information were Television/Radio (37.1%), School teachers (30.4%), Parents (15.6%) and friends (11.4%). No tobacco consumer knew that tobacco use leads to hypertension/heart disease and less than one percent adolescents were concerned about financial burden due to tobacco consumption. Six FGDs with adolescent boys explored the commonly used tobacco products, sources of money to purchase tobacco, reasons for its use and non-use, current use of tobacco as medicine for health problems and some solutions to reduce primary uptake of tobacco by adolescents. The FGD findings have also been expressed in the form of conceptual framework explaining the underlying pro tobacco factors for adolescents [Figure - 1]. According to FGD respondents, few adolescent boys taste tobacco by 8-10 years of age, while girls do it by 12-13 years. Peer pressure acts as a pro tobacco influence among boys who are outgoing and spend more time with their friends. They prefer to consume freshly prepared kharra which was supposed to be less strong ( tej ) than gutka. Adolescent boys knew that gutka consumption subsequently leads to problem of difficulty in opening mouth, which is locally termed as Jabda basne . In rural settings, family members and neighbors who often ask young children to get tobacco from nearby shops, local media advertisements and colorful attractive packing of tobacco products acts as another pro tobacco influences for new children to take up tobacco habit. As tobacco was said to reduce tiredness and bring excitement in body, farmers/laborers frequently consume it after heavy work. Apart from this, tobacco is being used in treatment of some health problems. Tobacco is chewed after meals for better digestion, given to ease toothache, pain in abdomen and to induce vomiting in suicidal insecticide poisoning. The mixture of dry tobacco & lime is applied to stop bleeding of fresh wounds caused during farm work. It is also believed that tobacco consumers are protected from poison of snake and scorpion. Some children start using tobacco as infant, when their mothers apply tobacco leaf soaked in castor oil over chest of rapidly breathing child with pneumonia. Sometimes, mothers and grandmothers gave tobacco to adolescent girls to ease abdominal pain during menstruation. Some school going children get pocket money by their parents and guest (other social source) and non school going/school drop-out boys arrange money through their daily wages. In some families, tobacco is purchased like other household grocery items from shops in cheap village level weekly market. The statuary health warning on tobacco products in small print is often ignored and it is said to be the subject of fun among peer groups of rural adolescents. According to FGD respondents, few adolescents do not consume tobacco as they fear their family members and their parents do not give them money. Some children themselves do not like sense of giddiness, nausea and other side-effects of tobacco. They fear habit forming, developing cancer and heart diseases as a result of school health education and their parent′s control. FGD respondents suggested ensuring education of parents, strict ban on tobacco sale to minors and school-based health education program targeting primary school children to reduce primary uptake of tobacco products. Discussion In the present community-based study, the rural adolescent consumed tobacco products like kharra (mawa), gutka , dry tobacco/ and lime, dry snuff ( nus ) and beedi/cigarette. Significantly more boys (79.2%) had consumed kharra (mawa) and girls (72%) had consumed dry snuff ( nus ) in last one month. The adolescents mostly consumed smokeless forms of tobacco products and only four percent boys smoked beedi /cigarettes. The FGD findings revealed medicinal use of tobacco and its socially accepted status in rural settings. The triangulation of quantitative and qualitative information obtained in the present study is useful for development of locally relevant health education material and intervention strategy. According to school-based GYTS in India, current use of any tobacco product among school children (13-15 years) was found to be 14.1% (17.3% boys, 9.8% girls). The prevalence was highest among male students in North East (34%) and the lowest was 4.9% among female students of western states. [11] In Maharashtra, 12.9% adolescents (13-15 years) currently consumed any tobacco products. [2] About 58% of tea plantation youths (15-24 years) in Assam were found to consume at least one tobacco products. [12] In the present community-based study, 39% adolescents (15-19 years) currently consumed tobacco products. Among tobacco users, 33% adolescents (26% boys and 72% girls) used dry snuff for teeth cleaning. Sinha et al have reported the use of tobacco products as dentifrice among adolescents (13-15 years) which ranges from 6% (Goa) to 68% (Bihar). [13] The Government of India has defined legislative measures, which prohibits the use of tobacco as an ingredient in dental care products and sale of tobacco related products to minors but there is no national level program or campaign to advocate it. [14] In the rural settings, where parents and neighbors asking young children to purchase tobacco products from nearby shop and use tobacco as home remedy for certain health problems brings its own stamp of authenticity regarding safety of these products and weakens the seriousness of side-effects of tobacco products among children. It was found that adolescents ignore the statuary health warnings written on tobacco products. The government of India has agreed to put evidence based pictorial depictions of ill effects of tobacco use on health on tobacco products. [15] It will help adolescents to visualize the seriousness of side-effects which is often ignored in peer groups. Apart from the strict enforcement of legislative measures, the tobacco demand from parent/relative/neighbors side should decline to reduce primary uptake of tobacco by young children. These efforts would require strong political commitment, effective community mobilization and health education of community members and adolescents. The reasons for tobacco use were clear but little information was available regarding its non-use. In the present study, the reasons for non use of tobacco among girls were fear of cancer (59%), poor oral health (37.9%). Among non consuming boys it was fear of cancer (58.6%), poor oral health (44.8%), and fear of getting addiction (29.3%). Significantly more non user boys had fear of parents and developing addiction as compared with the girls. Notably, only three percent did not accept tobacco as medicine for pain in abdomen, toothache and wound dressing etc. The non-users were aware that tobacco causes various side-effects like cancer, tuberculosis, poor oral health and development of addiction. The major sources of information for non-users were school teachers and Community based groups. The conceptual framework explained the possible relationships of various pro-tobacco influences which prompt rural adolescents to consume tobacco. This approach to obtain information is crucial for building theory based health education intervention strategy for behavior change which is a definitive need for health education intervention in India. [16] Thus, there is a need of behavior change communication strategy based on indigenous concerns and addressing socio-cultural barriers by reinforcing locally existing channels of communication to break away isolation and build interactive village level networks. [17] The intervention strategy focusing on advocacy and implementation of anti tobacco law, community based health education of parents & non school going children/ school drop-outs and school based education through teachers would be appropriate for rural settings of developing countries. Sinha et al found that community centered mass approaches with minimal sustained intervention was more effective than clinic centered, intensive, individual approach. [18] World Health Organization has suggested to design, implement and evaluate community based intervention intended to prevent primary uptake of tobacco among youths. [3] Sandford has also recommended a comprehensive approach to tobacco control. This should include a range of measures, notably: a total ban on tobacco advertising and promotion; restrictions on smoking in public places and in the workplace; sustained increases in tobacco taxation combined with measures to curb smuggling; large, bold health warnings on tobacco products; smoking cessation and health education campaigns; and the regulation of tobacco to standards agreed by the health community rather than those set by the tobacco industry. [19] To conclude, the current consumption of any smokeless tobacco products among rural adolescents was found very high. A multi-pronged community based intervention strategy which ensures enforcement of law and awareness of parents and school children about side effects of consumption of tobacco is required to reduce primary uptake of tobacco especially smokeless tobacco among rural adolescents. The behavior change strategy for target audience should be based on locally relevant data. The limitations of the present study should also be kept in mind. The study was conducted in a small geographical area covering 11 villages. The scope of qualitative data obtained is to offer possible explanations to gaps in information and generate hypothesis for further research. The confirmation of findings at larger scale is recommended. References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08032t1.jpg] [cn08032t4.jpg] [cn08032t3.jpg] [cn08032f1.jpg] [cn08032t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}