 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
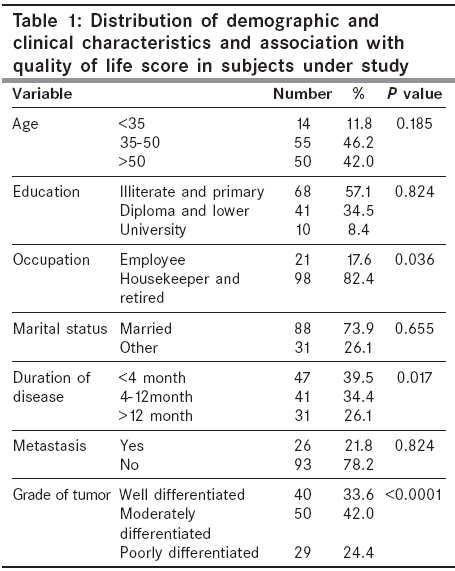
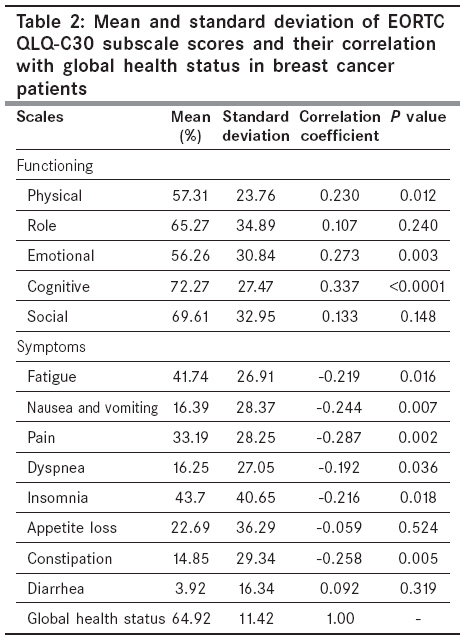
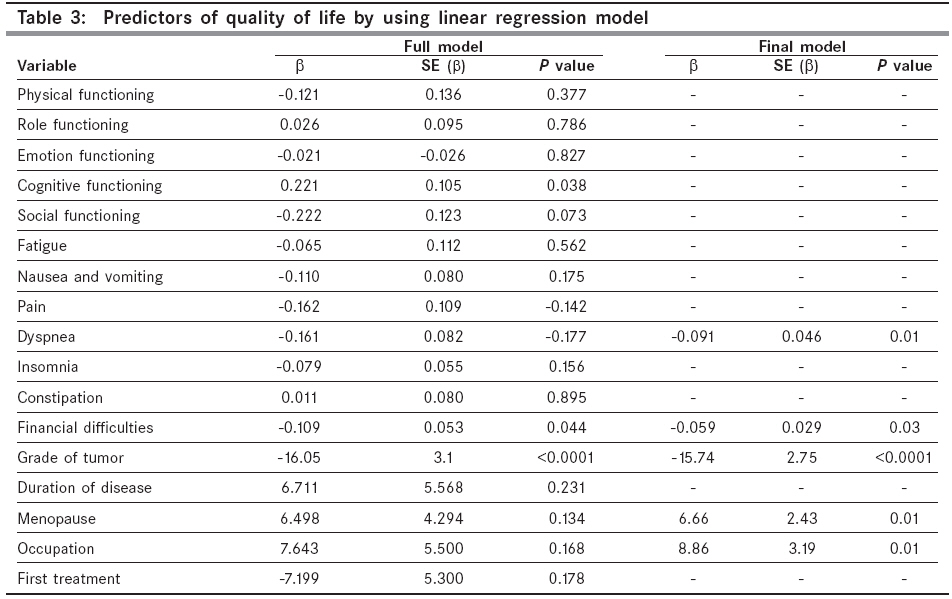
Indian Journal of Cancer, Vol. 45, No. 3, July-September, 2008, pp. 107-111 Original Article Predictors of quality of life in breast cancer patients under chemotherapy Safaee A, Moghimi-Dehkordi B, Zeighami B, Tabatabaee HR, Pourhoseingholi MA Department of HSR, Research Center of Gastroenterology and Liver Diseases, Shahid Beheshti University (MC), Tehran Code Number: cn08033 Abstract Background: Today, the quality of life studies has an important role in health care especially in chronic diseases. Breast cancer has third order among women's malignancies. Now, survival rate for this cancer is long. However breast cancer has several complications that affected the patient's life.Aims : The aim of this study was to assess the quality of life in Breast cancer patients under chemotherapy. Setting and Design: A cross-sectional study conducted on 119 breast cancer patients that were admitted and treated in chemotherapy ward of Namazi hospital in Shiraz city, south of Iran, between Jan and Feb 2006. Materials and Methods: The QLQ-C30 questionnaire was used to assess quality of life in these patients. Statistical Analysis: We used univariate methods. A multiple regression analysis was performed to identify predictors of quality of life. Results: Mean age of patients was 48.27±11.42 with quality of life total score 64.92±24.28. All symptoms scales had reverse association with quality of life except appetite loss (P>0.05) and diarrhea (P=0.752). The results of the regression analyses showed that only grade of tumor, occupational status, menopausal status, financial difficulties and dyspnea were statistically significant in predicting patients' quality of life. Conclusion: In conclusion, this study demonstrates the strength of the relationship between clinical and sociodemographical factors and breast cancer patients' quality of life. Psychological and financial support for women experiencing breast cancer diagnosis may improve quality of life. Keywords: Breast cancer, functioning scales, symptoms scales, quality of life, QLQ-C30 Introduction Quality of life (QOL) is a very frequently applied concept nowadays. [1] It is a subjective concept and its definitions and the sub concepts involved have varied. QOL has been defined as the subjective evaluation of life as a whole or the patient′s appraisal and satisfaction with their current level of functioning compared with what they perceive to be possible or ideal. [2] In a simple way, QOL is individual imaginations or thoughts from life style according to his/her objectives, expectations, standards and preferences. QOL is a multidimensional construct encompassing perceptions of both positive and negative aspects of dimensions such as physical, emotional, social and cognitive functions, as well as the negative aspects of somatic discomfort and other symptoms produced by a disease or its treatment. [2] Today, quality of life survey is an important issue in health care, especially oncological researches .Cancer affects on different aspects of QOL and at present time, cancer disease is a major problem in Iran and whole of the world. Among these cancer diseases, breast cancer is the most common cancer in women. [3] During last decades, survival rates for breast cancer have increased as a result of earlier detection and increased use of adjuvant therapy. [4] Women may also receive radiation therapy and/or chemotherapy plus systemic hormonal therapy for breast cancer treatment depending on stage and estrogen receptor status at diagnosis. Long-term consequences of therapy include painful and often debilitating lymph edema due to surgery or radiation therapy consequently, these patients are engaged with cancer and its outcomes and effects, for a long time. Therefore, it is critical for health care professionals to become familiar with the impact of a breast cancer diagnosis and its treatment on patient′s QOL. [3] The aim of this study was to assess breast cancer patients′ QOL and recognize the factors that affect QOL. Materials and Methods We conducted a cross-sectional study on 119 random samples of breast cancer patients that were admitted and treated in the chemotherapy ward of Namazi hospital in Shiraz city, south of Iran between December 2005 to February 2006. This center is a referral center in south of province. Any patients with a new diagnosis of breast cancer, according to pathology report, under chemotherapy were eligible to enter the study. The exclusion criteria were: cancer diagnosis less than two months; recurrent of breast cancer cognitive impairment; other previous or concurrent malignancies. We used QLQ-C30 questionnaire to assessment QOL in these patients. This questionnaire is a valid and reliable questionnaire for evaluation of quality of life in Iran. [5] The QLQ-C30 questionnaire is a self-report multidimensional general cancer-specific questionnaire, which was designed to assess QOL in cancer patients. The QLQ-C30 proved useful in many clinical trials, because it assesses the main factors influencing HRQOL of patients with cancer. [5],[6],[7] The QLQ-C30 is multidimensional, made up of 30 items (five functional domains: physical, role, emotional, cognitive, and social, one global QOL domain, three symptom domains: fatigue, nausea-vomiting, pain, and six single items). The scores are transformed into 0-100 point scales. In the case of the five functional scales and the global QOL scale, the high score means: ′high level of functioning or global QOL′. On the other hand, in the case of symptom scales and single items, the higher score implies the higher level of symptoms or problems. [8],[9],[10] Sociodemographic data included age, education, occupation and marital status, and Clinical data including grade of tumor, metastasis, type of treatment, type of first treatment, co-morbidity, type of treatment, type of first treatment, duration of disease and status of menopause gathered by additional questionnaire. The study protocol has been approved in ethical committee of Shiraz University of medical science. Before the interview survey, the interviewer explained the purpose of these questions to all eligible individuals and requested their participation. We used univariate methods such as Kruskalwallis, Mann-Whitney U and Spearman correlation tests. A multiple regression analysis was performed to identify predictors of QOL. For this procedure, the global QOL score of the EORTC QLQ-C30 was treated as the dependent variable. Sociodemographic, medical characteristics and symptom of disease were entered as explanatory factors in the model. [11],[12],[13] All calculation performed using SPSS.V.13. Results Total of 119 patients with breast cancer were interviewed. The demographic and clinical characteristics of the baseline sample are shown in [Table - 1]. The mean age was 48.27 (SD=11.42) years, and most of the patients were married (73.9%). The level of education in our study sample was relatively low concerning employment status, most of women were housekeeper or retired and only 17.6% were employed before the cancer was diagnosed. The mean score for the global health status for breast cancer patients was 64.92±11.42. The best functional outcomes were found for the cognitive and social functioning subscales and emotional functioning scored the lowest. Breast cancer patients were suffered from insomnia, fatigue and pain. Other symptoms such as diarrhea, constipation, dyspnea, nausea and vomiting and appetite loss were reported less severity [Table - 2]. In univariate analysis, among demographic factors (such as age, education, marital status and occupation) only occupational status was associated with Global Quality of life, and employed women had better QOL ( P =0.036). Duration of disease was significantly related to QOL score of patients. In other words, those with duration of disease less than four months reported significantly lesser global QOL score ( P =0.017). Results of univariate analysis show significant differences in global QOL scores, where patients with poor grade have the worst ( P < 0.0001). No significant association observed between QOL and other clinical factors (such as metastasis of tumor, type of treatment, type of first treatment, comorbidity, duration of disease and status of menopause). All symptoms scales had reverse association with QOL except appetite loss ( P =0.285) and diarrhea ( P =0.752). Also, QOL in breast cancer patients was affected by financial difficulties ( P =0.019). The results of the regression analyses showed that only grade of tumor, occupational status, menopausal status, financial difficulties and dyspnea were statistically significant in predicting patients′ QOL [Table - 3]. Duration of disease, and other symptom scales were not significant. Discussion This study demonstrates the consistency and strength of the relationship between grade of tumor, occupation, dyspnea, menopause status and financial difficulties and breast cancer patients′ quality of life. The strongest influence on QOL in our study was grade of tumor. These assessments showed that the emotional functioning score and the physical scores were lower compared to the other QOL subscale scores. This might be due to the fact that patients were informed about their cancer diagnosis. Facing a life-threatening illness and the uncertainty of treatment outcomes is psychologically distressing. During the active phase of treatment physical functioning has an enormous impact on QOL. Patients may experience acute side effect of the treatment in addition to cancer-related symptoms which can be emotionally distressing and debilitating. Previous studies have demonstrated the relationship between physical factors and emotional distress. [14],[15],[16] After the completion of cancer treatment, patients are usually able to return to a level of physical functioning consistent with that of their pre-cancer diagnosis. [16] Concerning demographic factors (age, education, and marital status) the subgroups did not differ from one another. Some research, but not all, indicates that younger women may suffer poorer QOL following a breast cancer diagnosis. [17],[18] Unfortunately, age definitions vary across studies. This association wasn′t seen in our study. In line with other findings, in the present study, employment status was significantly associated with QOL. [4],[16] Postmenopausal women had better QOL. This relation may be confounded by effect of age. Our findings suggest that financial status may also play an important role in determining QOL. Developing a chronic illness or having a spouse with chronic illness like cancer would mean loss of that day′s income, and extra expenditures and influence many aspects of life. [19],[20] However, the regression model explained only 73.6% of the variance. There may be other variables, such as toxicity or symptom distress, which have not been sufficiently considered in this study. Interpretation of our data must consider some limitations (e.g. sample size and study design). The cross-sectional design allowed identification of several factors associated with QOL, although causal inferences could not be made. Factors related to QOL impairment were identified (e.g. grade of tumor, occupation, financial difficulties, and etc.). The findings of this study should be the target of further research, emphasizing the need for interventional studies that minimize the negative impact of the disease symptoms on the QOL in women with breast cancer. Prospective studies are needed to evaluate the influence of other factors (education, socioeconomic status, type of surgery, quality of partner relationship) on QOL. Future research should include a comparable group of women without breast cancer, seeking to identify whether QOL and its associated factors are similar among women with and without breast cancer. Conclusion In conclusion, this study demonstrates the consistency and strength of the relationship between clinical and sociodemographical factors and breast cancer patients′ quality of life. Psychological and financial support for women experiencing breast cancer diagnosis may improve QOL.Acknowledgments We would like to thank the staff of the Chemotherapy ward of Namazi Hospital for their valuable collaboration in this study and EORTC quality of life group for their permission to use of QLQ-C30 questionnaire.References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08033t1.jpg] [cn08033t2.jpg] [cn08033t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}