 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
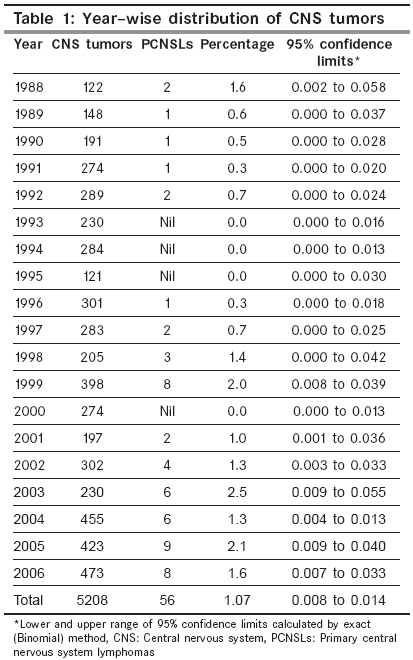
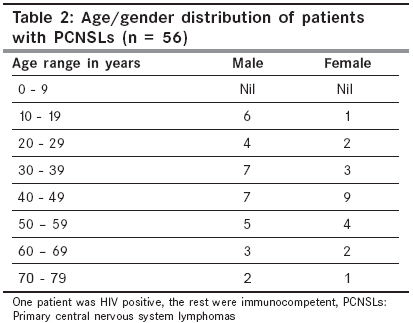
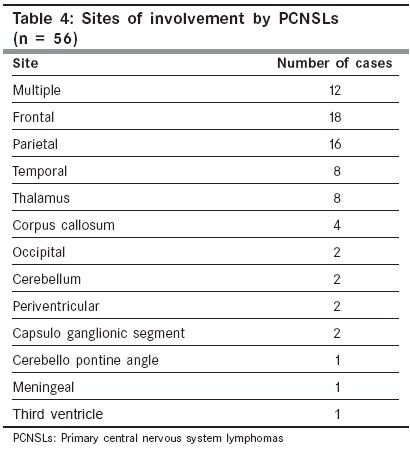
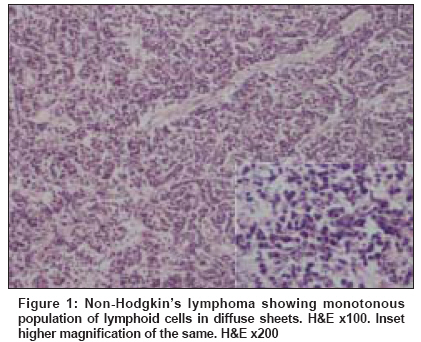
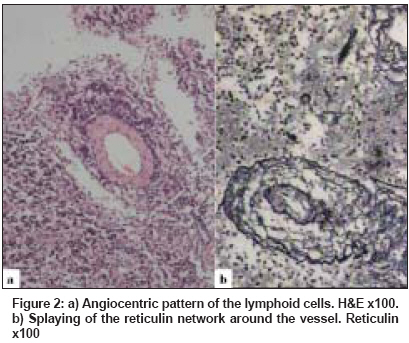
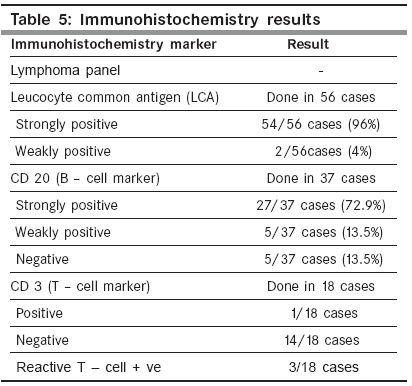
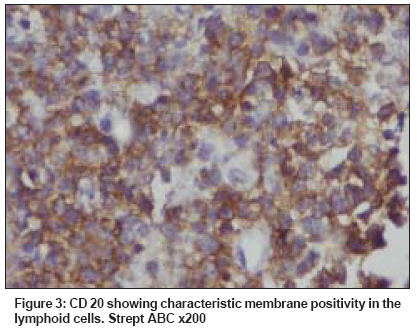
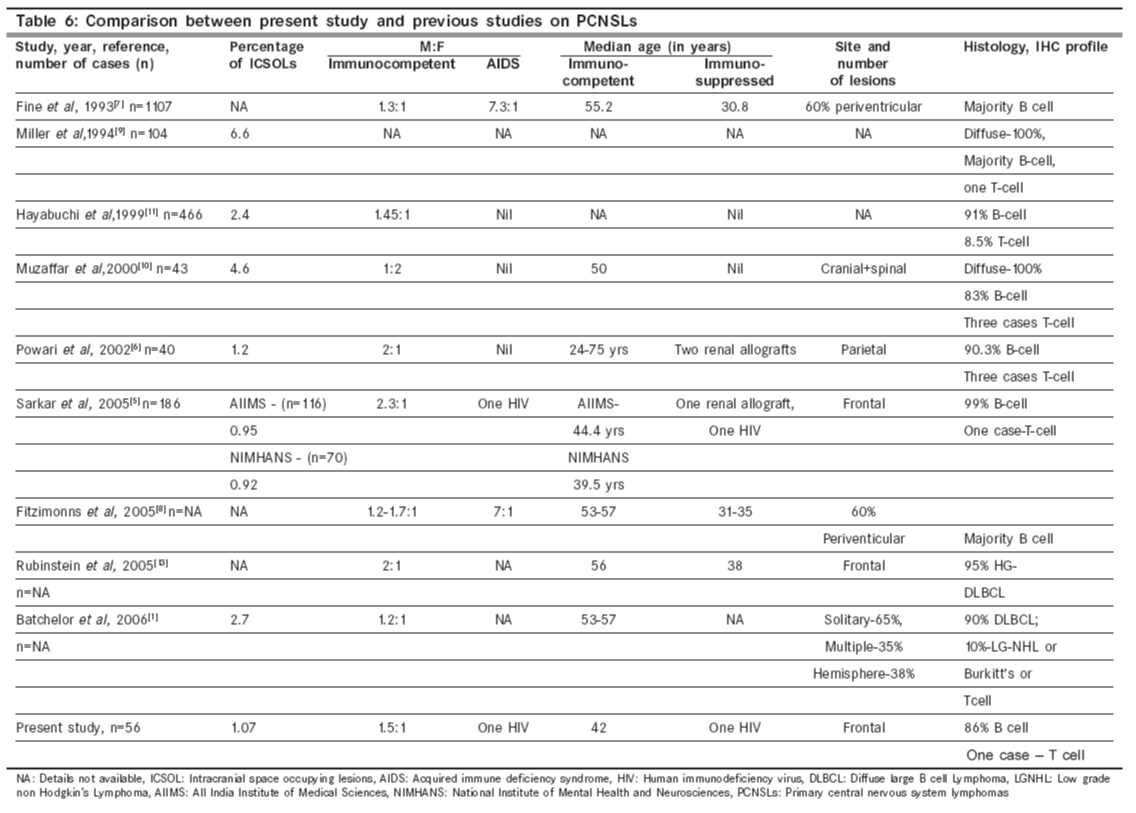
Indian Journal of Cancer, Vol. 45, No. 3, July-September, 2008, pp. 112-118 Original Article Primary central nervous system lymphomas: Indian experience, and review of literature Paul TR, Challa S, Tandon A, Panigrahi MK, Purohit AK Department of Pathology, Nizam's Institute of Medical Sciences, Punjagutta, Hyderabad - 500 082, Andhra Pradesh Code Number: cn08034 Abstract Primary central nervous system lymphomas (PCNSLs) are a rare form of non-Hodgkin's lymphoma which arise within and remain confined primarily to the central nervous system (CNS). They generally account for 1-2% of all primary brain tumors and are reported to be on the rise due to the Acquired Immune Deficiency Syndrome (AIDS) epidemic.Aims and Objectives: To study the clinicopathological and immunophenotypic characteristics of PCNSLs and look for any differences in PCNSLs reported in India from those in other countries. Materials and Methods : All cases of PCNSLs between January 1998 and December 2006 were reviewed. Presence of lymphadenopathy, organomegaly and bone marrow study was done to exclude the possibility of secondary involvement by lymphoma. The diagnosis was confirmed by histopathology with Hematoxylin and Eosin and reticulin stains. Immunohistochemistry (IHC) with leucocyte common antigen (LCA), CD 20 and CD 3 was performed on available blocks. The immune status was evaluated by clinical examination and human immunodeficiency virus (HIV) serology (since 1996). Results : In a 19-year study period, there were 56 patients of PCNSLs, accounting for 1.07% of all intracranial neoplasms. The patients ranged from 10-75 years of age with a median age of 42 years. Barring one patient who was HIV positive, all the others were immunocompetent. All cases were diffuse large cell lymphomas on histopathology. IHC with LCA and CD 20 revealed positivity in 100% and 86.4% cases respectively. There was a single case of CD 3 positive T-cell lymphoma. In the present study, PCNSLs occurred in young immunocompetent patients and majority were diffuse large B cell lymphomas. Keywords: Diffuse lymphoma, immunohistochemistry, PCNSLs Introduction Primary central nervous system lymphomas (PCNSLs) are a rare form of extranodal non-Hodgkin′s lymphoma, that typically remain confined primarily to the central nervous system and involve the brain, leptomeninges, spinal cord or eye. [1] Historically, the first reported PCNSL was by Bailey in 1929, [2] when he used the term ′perithelial sarcoma′. Other terms that have been used are perivascular sarcoma, adventitial sarcoma, malignant reticuloendotheliosis, reticulum cell sarcoma, microglioma. It was much later that PCNSLs were recognized as neoplasia distinct from glial tumors by immunophenotyping and the lymphoid nature of the lesion was established. Reports from the west [3] indicated that there was a three-fold increase in incidence of PCNSLs between 1973 and 1984. The Human Immunodeficiency Virus (HIV) was the main factor responsible for the rise. However, there was also a rise of PCNSLs in the immunocompetent. This increasing incidence could have been due to improved investigative modalities (stereotactic brain biopsies of deep-seated lesions), greater clinical and neuropathological awareness, widespread availability of immunohistochemistry and increase in the number of immunosuppressed patients, who have an increased risk of developing PCNSLs. Later reports [4] suggested that the annual incidence of PCNSL appeared to be stabilizing or in fact declining slightly. Studies published from India [5],[6] indicate that there has been no increase in the incidence of PCNSL and that they tend to occur a decade earlier than the west. The purpose of this study was to determine the clinico-pathological profile of patients diagnosed with PCNSLs at a tertiary care centre, to determine the hospital-based incidence and look for any differences in PCNSLs occurring in India from those in other countries. Materials and Methods All cases of histologically proven PCNSLs, diagnosed at a tertiary care center from January 1988 to December 2006, were included in the study. The complete clinical and imageologic details were obtained from the patient records. Details about lymphadenopathy, organomegaly and bone marrow study were obtained to exclude the possiblity of secondary involvement by a systemic lymphoma. The histopathology of each case was reviewed with Hematoxylin and Eosin and reticulin stain. Immunohistochemistry (IHC) with leucocyte common antigen (LCA), CD 20 (B cell marker), and CD 3 (T cell marker) was performed on available formalin-fixed, paraffin embedded blocks using the standard Avidin-Biotin Complex technique. The antibodies used were monoclonal mouse Anti Human leucocyte common antibody CD 45, monoclonal mouse Anti Human CD 20 cy and polyclonal rabbit Anti Human CD 3.These were supplied by DAKO / Dakocytomation company (the suppliers being J. Mitra and sons, Chennai, Tamil Nadu, India; imported from Denmark.) The immune status was evaluated by clinical examination and HIV serology reports were available in all patients after 1996.Results Incidence Clinical features The most common presenting symptom was headache. The site of involvement is shown in [Table - 4]. Majority of the lesions occurred in the supratentorial region, with multiple lesions being common and frontal lobe being most frequently involved. Imageologic details were available in 36 of 50 patients. In 20 of these patients, CT scans were available and in another 16 cases, MRI scans were also available. The CT scans showed isodense to hyperdense lesions in majority of the patients and four patients had hypodense lesions. The MRIs revealed lesions which were hypointense on T 1 and hyperintense on T 2 with three patients having ring-enhancing lesions. All the patients were assessed for evidence of a systemic lymphoma and the search did not yield a primary. Most of the patients had a bone marrow evaluation as part of a staging work-up, but these were normal. After diagnosis, most of the patients were referred for chemotherapy and/or radiotherapy. They were subsequently lost to follow-up. Pathology Histopathology Immunohistochemistry IHC was performed, whenever the blocks were available. The panel used when lymphomas were suspected were LCA, CD 3 and CD 20. Leucocyte common antigen (LCA) was strongly positive in 42 cases and weakly positive in 2 cases. The B-cell marker CD 20 was positive in 86% cases [Figure - 3]. Due to non-availability of the markers, further typing with CD 79a or PAX 5 for B-cell origin was not done. Three cases of B-cell lymphoma showed reactive T- lymphocytes and one case was diagnosed as a T- cell lymphoma. This patient was a female, immunocompetent with a single lesion in the cerebellum. IHC was performed with other markers when there was a differential diagnosis of lesions like metastasis, small cell glioblastoma and other round cell tumors. The other markers done which were negative, were epithelial membrane antigen (EMA)-3 cases, glial fibrillary acidic protein (GFAP) - 8 cases, and one case each of cytokeratin (CK), neuron specific enolase (NSE) and CD 99. Discussion The results of our findings were compared to other studies - western, Indian and from the far east and are shown in [Table - 6]. The incidence of PCNSLs in India seems to be fairly constant through the years, as seen in previous series [5],[6] as well as in the present study. In literature, the incidence varies in different time periods. One publication from Pakistan, [10] which included both cranial and spinal lymphomas, reported that lymphomas accounted for 4.6% of intra-cranial and spinal neoplasia. There have been two large case-studies from Japan [11],[12] which reported that PCNSLs accounted for 2.4% of all intracranial neoplasms in Japan. The male to female ratio is 1.5:1 in the present series, which is similar to most published series in immunocompetent patients. In patients with AIDS, the disease is much more common in males. In the previous studies from India, [5],[6] majority of the PCNSLs have been reported in the immunocompetent. The present study has only one patient who was HIV positive (35 year old male). Sarkar et al, [5] had one HIV positive patient and one patient of renal allograft. Powari et al , [6] had two patients with renal allografts. In spite of an increasing number of HIV positive patients in India, the incidence of PCNSLs in these patients is low. A possible explanation for this could be that AIDS patients die earlier in India due to opportunistic infections. [5] Though other lymphomas, including those at extranodal sites seem to occur in India in patients with AIDS, PCNSLs are still infrequently reported. The median age of presentation is 42 years in immunocompetent, which is similar to those observed from India like - AIIMS (44.4 years) and NIMHANS (39.5 years). This is a whole decade earlier than those reported in the west. This has been attributed to the demographic pattern of the Indian population. [5] The authors have also observed that other hematologic malignancies like multiple myeloma and chronic myeloid leukemia also present a decade or two earlier in India than in the west. The most common presenting symptom was headache occurring in 57% patients. Seizures at presentation were seen in only 20% patients. This has been attributed to the fact that PCNSLs less often involve excitable cerebral cortex than other tumors do. [14] In this study, majority of the lesions were in the supratentorial region with the frontal lobe being most commonly involved. This is similar to other studies. [5],[13] Of the 56 PCNSLs, 55 were diffuse large cell lymphomas and one was reported as lymphoblastic. Virtually all PCNSLs show a diffuse growth pattern. A follicular growth pattern has not been described in intraparenchymal lesions. There have been occasional case reports of follicular lymphomas of the dura. [15],[16] These lesions have a less aggressive behavior and survive longer than the usual intraparenchymal PCNSLs. Of the cases where immunohistochemistry was performed, 86% were classified as B-cell lymphomas. This is similar to reports, [1] where 90% of the PCNSLs are diffuse large B-cell lymphomas. There was one case of T-cell lymphoma, which occurred in a 51-year-old female in the cerebellum. As per literature, [17] T-cell lymphomas constitute only 2% of all PCNSLs, occur mainly in the immunocompetent, have a higher male to female ratio, are more frequent in the posterior fossa, mainly cerebellum, with a propensity to arise in the meninges. Studies from the east [11],[18] indicate that the incidence of T-cell lymphomas were high in Japan (8.5%) as well as Korea (16.7%). T-cell lymphomas have to be differentiated from T-cell rich B-cell lymphomas. There were three cases of B-cell lymphomas which had reactive T lymphocytes, admixed with the tumor cells. Majority of the patients were further evaluated for lymphadenopathy, organomegaly, and had a bone marrow evaluation to rule out secondary involvement by a systemic lymphoma. None of the patients had marrow involvement at diagnosis. Following the diagnosis of PCNSL, the extent of staging required to evaluate for a systemic lymphoma is controversial. [1],[8],[19] There are those who advocate that it is sufficient to perform a thorough clinical examination, complete blood counts, routine biochemical tests, serum LDH levels and chest radiographs; but there are others who recommend that the patients have contrast-enhanced CT scans of the chest, abdomen, pelvis as well as a bone marrow biopsy, given that 3.9-12.5% of patients with PCNSLs are found to have occult extra neural disease on additional evaluation. Regarding prognosis, [20] it is suggested that an age more than 60 years, performance status more than one, elevated LDH levels, high CSF proteins and involvement of deeper regions of the brain (periventricular, basal ganglia, brain stem and cerebellum) were significantly and independently associated with a worse survival. The exact pathogenesis of PCNSLs in the immunocompetent is still not clear. Various theories of origin have been put forward. [7],[17]
Studies have shown a consistent association of tumors occurring in immunocompromised individuals with Ebstein Barr virus (EBV), suggesting an important role for the virus in the pathogenesis of these tumors. An infrequent association of the virus with PCNSL in the immunocompetent has also been noted. A study from India [22] showed that immunocompetent individuals in developing countries are infrequently EBV associated and possibly a different pathogenetic mechanism is operational in the evolution of these tumors. Systemic diffuse large B cell lymphomas (DLBCLs) are known to be clinically and morphologically heterogenous. They have recently been sub-classified as germinal centre B-cell origin (GCB) and non-germinal centre B-cell types using microarray. The germinal centre B-cell DLBCL is associated with a better prognosis compared to non-germinal centre B cell type. PCNSLs have a poorer prognosis when compared to other DLBCLs. Two studies [23],[24] using an extensive immunohistochemical panel including CD 10, BCL - 6, BCL - 2, MUM 1, etc have shown that PCNSLs are more homogenous than systemic DLBCLs and predominantly express the activated B-cell line (ABC) phenotype. This activated B-cell phenotype is thought to be responsible for the biologic aggressiveness and poor prognosis of PCNSL. Conclusion The present study, like other Indian studies, [5],[6] concludes that there has not been an increase in PCNSLs in India. The PCNSLs tended to occur in young patients, and majority were diffuse large B cell lymphomas. Though there is an epidemic of HIV/AIDS in India, association of PCNSLs with HIV/AIDS is still low.References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08034t5.jpg] [cn08034t3.jpg] [cn08034t2.jpg] [cn08034t6.jpg] [cn08034f3.jpg] [cn08034f1.jpg] [cn08034t1.jpg] [cn08034f2.jpg] [cn08034t4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}