 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
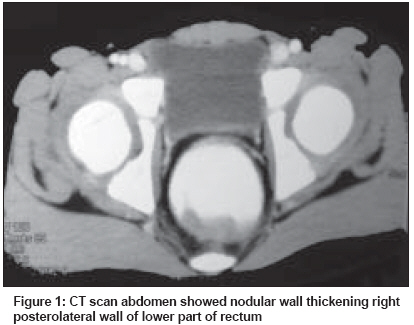
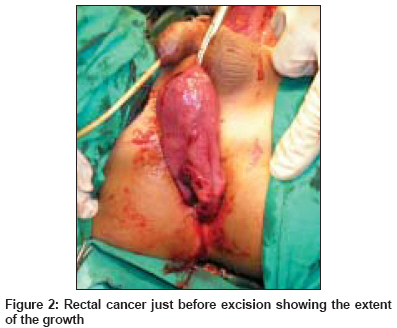
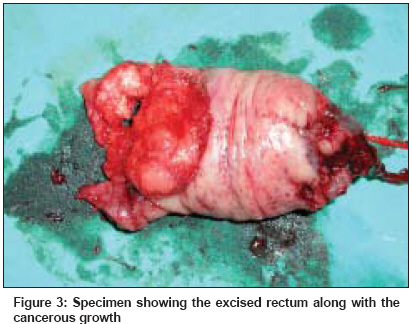
Indian Journal of Cancer, Vol. 45, No. 3, July-September, 2008, pp. 119-122 Original Article Pediatric carcinoma of rectum - Varanasi experience Pandey A, Gangopadhyay AN, Sharma SP, Kumar V, Gupta DK, Gopal SC, Singh RB Department of Pediatric Surgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi, 221005, Uttar Pradesh Code Number: cn08035 Abstract Background : Primary gastrointestinal system malignancies constitute approximately 2% of pediatric neoplasm and of these; colorectal carcinoma is the second most common malignancy. This is one of the rarer diseases in children.Aim : We reviewed our records to study the clinical features, outcome and the follow-up of this condition with evaluation of the prognostic factors. Settings and Design: Tertiary care Pediatric Surgery centre. Retrospective study. Materials and Methods : The data of all patients with diagnosis of colorectal carcinoma from January 1986 to January 2006 were reviewed. The confirmation of the diagnosis was by biopsy from the lesion. The age, sex, family history, clinical features, response to the treatment and follow-up were studied. Results : There were four male patients. All had bleeding per rectum as the presenting complaint. Three patients had advanced disease at presentation. All the patients had signet cell adenocarcinoma. The two patients expired and one was lost to follow-up. One patient is alive after one year of follow up and is receiving treatment. Conclusion : Colorectal cancer in children though rare can be a reality, hence any children presenting with pain in abdomen along with doubtful history of constipation and rectal bleeding should be examined carefully with special emphasis on digital rectal examination. Keywords: Adenocarcinoma of colon in children, colorectal cancer in children, rectal cancer Introduction The adenocarcinoma of the colon and rectum is the most common cancer of gastrointestinal (GI) tract in children. The life-time risk of colorectal cancer in the general population is five to six percent. [1] Primary gastrointestinal system malignancies constitute approximately 2% of pediatric neoplasm and colorectal carcinoma is the second most common malignancy after primary liver tumors. [2] Carcinoma rectum is a very uncommon malignancy in childhood. The incidence of colon cancer is found to be 1.3 cases per million children. [3] In children, there is a higher incidence of involvement of the right and transverse colon compared with adults and a far lower rate of involvement of rectum. [4] Because of the rarity of the disease in children, we reviewed our records to have the clinical features, outcome and the follow-up of this condition with evaluation of the prognostic factors in a developing country like ours. Materials and Methods This was a retrospective study. All the children with diagnosis of carcinoma rectum presenting to the department from January 1986 to January 2006 were included in the study. The confirmation of the diagnosis was by biopsy from the lesion. The parameters studied were age, sex, family history, clinical features, response to the treatment and follow-up. The extent of the disease was determined by using modified Dukes staging scheme. According to this system only the mucosa and submucosa are affected in stage A, the disease is limited to the bowel wall in stage B, the disease is limited to the lymph nodes in stage C, and there are distant metastases or peritoneal implants or direct invasion of other viscera in stage D. Case 1 Case 2 Case 3 Case 4 Results The study period was 20 years. The total number of patients was four and all were males. All the patients had bleeding per rectum as the presenting complaint. The first three patients were Dukes Stage D while the fourth patient was Stage B. In all the patients, the mass could be felt by DRE. Histopathologically, all the patients had signet cell adenocarcinoma. Two patients expired and one was lost to follow-up. One patient is alive after one year of follow-up and is receiving treatment.Discussion Compared to the adults, colorectal carcinoma is rare in children and only 1% of the colorectal malignancies are noted in the patients less than 30 years of age. [5] The incidence drops down further for the children under 10 years of age. [6] There is a report of colon cancer developing in a nine-month-old female infant. [7] The predisposing factors such as familial polyposis of the colon and other polyposis syndromes, ulcerative colitis, familial multiple cancer syndromes are noted in 10% of the bowel cancers arising during childhood, which is far higher than in adult patients. [2] We did not encounter any of the predisposing factors in any of our patients. The common age of diagnosis is in the second decade of life usually from 15 to 19 years. [1] All of our patients were diagnosed during the early second decade which is close to the literature. In children the occurrence is higher in the males in the ratio of 2:1. [1],[5],[8] In our series all the patients were male. There are differences in the duration of symptoms, primary site, pathologic findings, stage and prognosis between the adults and the children. [1],[9] The common presenting symptoms for the children with colorectal carcinoma are abdominal pain and vomiting. [5] Other notable features are change of bowel habits, bleeding per rectum, constipation and weight loss. [1],[10],[11] The initial symptoms of vague abdominal pain and constipation may not be an indicator of malignancy and the physician goes for the more common pediatric surgical disorders such as appendicitis and intussusception, thus, colorectal carcinoma can easily be missed. [8] Anemia is treated as a routine without any suspicion. The adolescents do not relate rectal bleeding to the cancer, and are unlikely to volunteer this information. [9] All of our patients had the problem of rectal bleeding but this was told late in the course of the disease which increases its severity. Moreover they may hide the problem because of embarrassment. [1] In adult patients most of the colonic cancers are located within 25 cm of the anus including the rectosigmoid. [1],[8] In children the site of involvement has been varying. It has been found to be equally distributed in all parts of the colon, [12] transverse colon, [13] right and transverse colon [4] and rectosigmoid. [8] We had however encountered all patients with carcinoma of the rectum, making it as the most common and the only site of involvement in our series. Contrary to the adults who are mostly affected with moderately differentiated adenocarcinoma, the pediatric colorectal cancers are predominantly mucinous adenocarcinoma that makes up to 50% of the total cancers. [5] This type has been noted in only 5% of adult colorectal malignancy. [8] The mucin absorbs water, swells and invades tissues, thereby promoting spread of malignant cells. This tumor may grow to huge size because of the pooling mucin. It also interferes with the immune recognition of carcinoma cells caused by mucopolysaccharide coating. [2],[4],[8] The signet ring subtype has the worst prognosis. It grows so rapidly that regional lymph node involvement and diffuse peritoneal seeding is a common finding at the time of presentation, which leads to poor prognosis. [8] In all of our patients, signet ring subtype was the only variety observed. Vague symptoms, decreased awareness, and increased frequency of mucinous type results in advanced stages at presentation. Thus most of the children present in the Dukes C or D stage. [1],[5],[8],[9],[10],[14] which was also noticed by us. Only one patient in our series was fortunate enough to present with stage B. This delayed presentation ultimately leads to poor prognosis. The diagnosis of colorectal carcinoma is based on a high index of suspicion which can be confirmed by sigmoidoscopy or colonoscopy. It also helps in taking a biopsy under vision. Contrast studies, ultrasonography and computed tomography are essential procedures for detecting the extent of the disease. We could not have done the radiologic investigations such as contrast studies in the first two patients as both were operated as an emergency and full assessment of the extension of the disease was done at the time of laparotomy. The third patient did not receive any treatment or investigation as the attendants refused the treatment, hence only the last patient was fully investigated. The role of carcinoembryonic antigen (CEA) in the diagnosis and follow-up of colorectal carcinoma in children is not established at present. [1],[9] We did not go for the CEA in first three patients because of the non availability of the facility at that time. The value was non informative in the last patient (1ng/ml). The importance of DRE cannot be over-estimated in rectal carcinoma. Simple DRE can decisively improve the survival rate. [15] This simple maneuver however seems to be much neglected in the literature. [1],[5],[8],[9] It is even more relevant in developing countries with limited endoscopic diagnostic modalities especially for the children. We do agree that the proctoscope can also help to evaluate the tumor but we think that the DRE can help better for its assessment such as upper extent and consistency of the mass, status of the mucosa and enduration etc. In the study by Karnak et al , [8] all the seven patients having rectal carcinoma presented in the Dukes stage D and all of them expired within one year of diagnosis. We suggest that any child having even a single episode of rectal bleeding should be offered a DRE. Surgery is the most effective treatment for colorectal cancer. [1],[2],[5],[8],[9] It is to be stressed that the survival is dependent on the complete resection of the cancer and aggressive surgical procedures can increase the survival rates of these patients. In patients with resectable mass, complete tumor resection that includes the lymphatic basin of the affected colon and/or rectum has the greatest impact on the overall survival. Although adjuvant chemo-radiotherapy has limited value of benefit in most of the cases, a variety of new agents such as irinotecan, oxaliplatin and leucovorin used in association with 5-FU should be considered. [2] Colorectal carcinoma in children is usually a fatal condition, a finding that has also been observed by us. The 5-year survival rate for children ranges from 7% to 12% which is similar in both developed and developing countries. This poor prognosis is related to the delay in diagnosis, greater virulence of these tumors, advanced stage of disease at the time of diagnosis and the mucinous type of histology. [5],[8] All of these factors were noticed by us in all of our patients. To conclude colorectal cancer in children though rare can be a reality, hence any children presenting with pain in abdomen along with doubtful history of constipation and rectal bleeding should be examined carefully with special emphasis on DRE. References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08035f3.jpg] [cn08035f2.jpg] [cn08035f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}