 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
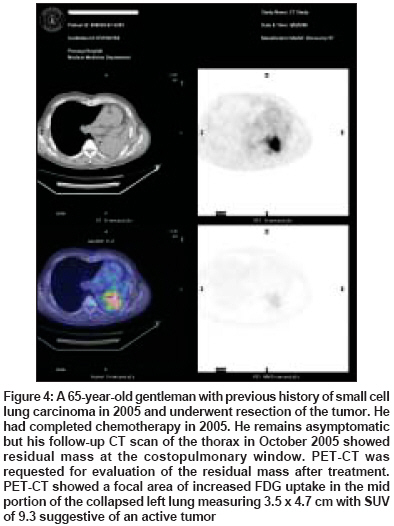
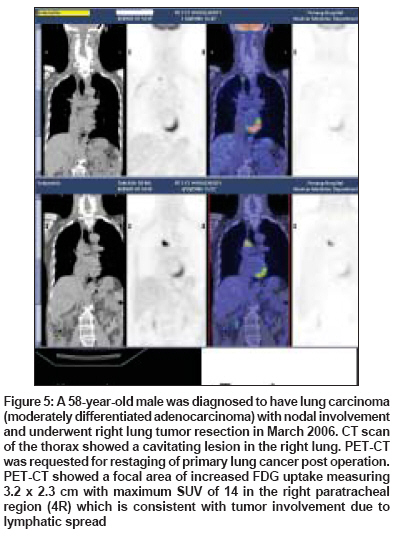
Indian Journal of Cancer, Vol. 45, No. 4, October-December, 2008, pp. 137-141 Review Article Integrated positron emission tomography/computed tomography fusion imaging: An emerging gold standard in lung cancer Joshi SC, Pant I, Hamzah F, Kumar G, Shukla AN Department of Oncology and Radiotherapy, Advanced Medical and Dental Institute, Universiti Sains Malaysia, Penang Code Number: cn08042 Abstract Positron emission tomography (PET) has emerged as an important diagnostic tool in the management of lung cancers. Although PET is sensitive in detection of lung cancer, but FDG (2-deoxy-2- 18 fluro-D-glucose) is not tumor specific and may accumulate in a variety of nonmalignant conditions occasionally giving false positive result. Addition of CT to PET improves specificity foremost, but also sensitivity in tumor imaging. Thus, PET/CT fusion images are a more accurate test than either of its individual components and are probably also better than side-by-side viewing of images from both modalities. PET/CT fusion images are useful in differentiating between malignant and benign disease, fibrosis and recurrence, staging and in changing patient management to more appropriate therapy. With analysis and discussion it appears that PET/ CT fusion images have the potential to dramatically improve our ability to manage the patients with lung cancer and is contributing to our understanding of cancer cell biology and in development of new therapies.Keywords: Lung carcinoma, positron emission tomography (PET), PET/computed tomography fusion images Introduction Positron emission tomography (PET) has emerged as a significant molecular imaging technique in the cancer research. In the management of lung carcinoma its use is increasing day by day with various new innovative approaches. PET has provided quantitative in vivo measurements of the biodistribution of radioactively labeled tracers in the lung tissue which can be labeled with short-lived radioisotopes of the natural elements of the biochemical constituents of the body tissue. [1] This provides PET with a unique ability to detect and quantify the physiological and receptor processes in the lung that is not possible by any other imaging technique. [2] The integration of PET and CT fusion provides, precise localization of the lesions on the FDG PET scans within the anatomic reference frame provided by computed tomography (CT). This increases the specificity of the imaging modality and in addition to this PET/CT fused images are always available at the end of the examination. The first proof of combined positron emission tomography (PET) and computed tomography (CT) (PET/CT) system in clinical practices was started in 1998. Since then PET/CT fusion has developed into the fastest growing imaging modality worldwide. [3],[4] Various recent PET/CT fusion studies on lung carcinoma have clearly advocated its role in the management of lung cancer patients [5] [Figure - 1]. The present article will outline the clinical application and significance of PET/CT in the diagnosis, treatment and follow-up evaluation in the lung carcinoma. General Technical Aspects of PET/CT Fusion Study The most commonly used radionuclide is Fluoride ( 18 F). Fluoride has a long half-life (110 min) for transport radiotracers over limited distances hence most widely used in PET as 2-deoxy-2- 18 fluro-D-glucose (FDG). FDG measures local rates of glucose metabolism of the cells. Since glucose metabolism is increased in lung cancer cells therefore PET with 18 FDG has a sensitivity to detect cacinoma. [6] In the evaluation of lung cancer patients, a very small amount of a biological compound labeled with a positron-emitting radionuclide (usually 18 F-fluoro-2-deoxy glucose, or 18 F-FDG) is injected intravenously and a PET scanner measures the localization of 18 F-FDG in tissue. [7] The PET image acquisition depends on external detection in coincidence of simultaneously emitted 511 keV gamma rays arising from the annihilation of emitted positrons (positively charged beta particles) by applying mathematical reconstruction techniques, data can be transformed into images that embody quantitative physiological, pathological or pharmacological information. [8] Clinically, variable diaphragmatic position or any other patient motion between CT and PET data acquisitions leads to errors in image fusion. This is rarely a diagnostic problem, since one has knowledge about how a PET lesion may be displaced on the corresponding CT image. [9] It has been shown that the use of CT data for transmission correction does not alter the size of the lesion significantly and that the measured standardized uptake values do not differ substantially from those obtained with radioactive source transmission correction. [10] All currently available data indicate that combined PET/CT is more sensitive and specific than either of its constituent imaging methods. In PET/CT fusion probably the most relevant additional effect is that CT data frequently add specificity to the FDG PET data. [5] However, FDG PET data also help to specify CT findings such as lymph nodes with an equivocal appearance. In some situations, such as when disseminated pulmonary metastases are too small to be seen at PET, CT is also able to increase the sensitivity of the PET/CT examination [Figure - 2],[Figure - 3]. Thus, there is general consensus that PET/CT is more accurate in lung tumor staging than PET or CT alone. [11],[12] The advantage of conjoint image viewing is such that authors of a recent study [13] have shown that in approximately two-thirds of patients with lesions seen on PET images; CT data are needed to improve the specificity of the findings. Once PET/CT data have been obtained, lesions identified at PET are localized in the anatomic CT reference frame. It is then a simple task to mentally register anatomic imaging studies performed during a different session to the PET/CT study because of the anatomic details available on the latter. Clinical Role of PET/CT in Lung Carcinoma It is reported that FDG PET is useful in differentiating between malignant and benign disease, [14] most accurate non-invasive method to detect and stage disease, [2],[4],[10] monitoring treatment response, [15] and restaging in case of suspected recurrent disease. [12] Integrated PET/CT adds important clinical information in comparison to PET alone, CT alone, or separate comparison of PET and CT images, owing to better lesion identification and localization and fewer overlooked lesions in tumors that do not consistently accumulate FDG [12],[16] This has major implications in terms of improving the planning of treatment and avoiding unnecessary treatment and its associated morbidity and cost. [5],[17] The establishment of diagnosis, staging, delivery of accurate treatment and its response including reduced costs and morbidity are the variables that should be measured to evaluate the efficacy of PET in lung cancers.PET in Solitary Pulmonary Nodules The advantage of PET/CT over PET in characterizing pulmonary nodules has not yet been defined. There have been many studies examining the accuracy of 18 F-FDG-PET in evaluating indeterminate solitary pulmonary nodules discovered by chest X-ray or CT scanning. [18] Analysis of these studies, involving over 500 patients, has shown a high sensitivity (average 96%) and accuracy (average 94%) for determining malignancy. [2],[7] Although FDG-PET is sensitive in detection of lung cancer, FDG is not tumor-specific and may accumulate in a variety of nonmalignant conditions also that may occasionally give rise to false negative result. [19] Conventional PET is unsuitable for tumor staging (T staging), because it cannot help anatomically define the tumor confines. Recently, it has been shown that in tumor staging of patients with lung cancer, analysis of integrated PET/CT images is superior to that of CT images alone, PET images alone, and PET and CT images viewed side-by-side [20] [Figure - 2],[Figure - 3]. Owing to the exact correlation between the extent of FDG uptake and anatomy, focal chest wall infiltration, mediastinal invasion, and differentiation of tumor from atelectasis are improved. The latter is particularly important for the planning of radiation therapy in patients with lung cancer associated with atelectasis. [21] However, PET/CT with non-enhanced CT is unable to distinguish contiguity of tumor and mediastinum from the direct invasion of the walls of mediastinal structures, and one still must rely on contrast-enhanced CT to help define mediastinal vascular invasion. The specificity is high but the variation is slightly greater and is dependent on the local prevalence of the known causes of false positive cases, particularly in granulomatous diseases such as tuberculosis and histoplasmosis. In carcinoid tumors, bronchioloalveolar lung carcinoma, and malignant effusions, diagnosis can sometimes only be based on the CT findings. The use of 18 F-FDG PET for solitary pulmonary nodules should at present be reserved for the cases where CAT Scan guided fine needle biopsy is technically difficult or has been non-diagnostic.PET/CT in Staging of non-small Cell Lung Carcinoma 18 F-FDG PET CT fusion is emerging as a standard preoperative assessment test in patients with non-small cell lung carcinoma (NSCLC). [22] In patients with known NSCLC the results of staging both within and outside the thorax are keys in determining operability. Demonstration of unilateral hilar lymphadenopathy is not a contraindication to surgery if the nodes can be resected with the primary tumor. Conversely, extensive mediastinal involvement of contra-lateral lymph nodes, as well as presence of distance metastases, should contraindicate surgery due to high surgical morbidity and the poor prognosis. The sub-optimal sensitivity, specificity and accuracy of conventional imaging techniques including CT and MRI, for staging of lung carcinoma has been demonstrated repeatedly. [23] FDG PET is more accurate than CT for identifying the metastasis as it is dependent not on size but on metabolic activity and has an accuracy of> 90% in identifying metastases, recurrent or persistent disease. Presently, PET-CT seems to be a more accurate standard method in the pre surgical diagnosis and staging of lung cancer [23] [Figure - 4]. Through correct staging and diagnosis of disease status by 18 F-FDG PET may not only change the treatment policy in disseminated disease making curative therapies futile but also avoid active treatment in absence of malignancy.PET/CT fusion in Recurrent Lung Carcinoma The ability to evaluate accurately residual masses following surgery or radiotherapy for lung cancer is essential in many patients. Post treatment fibrosis and scarring are common, and 18 F-FDG PET/ CT has been shown in small series to be accurate in detecting residual tumor that allows treatment-planning decisions to be made reliably [Figure - 5]. [24] Preliminary data suggest the superiority of PET for restaging of lung cancer and inferior prognosis for the patients with positive PET findings. The potential role of F-FDG PET/ CT fusion in treatment planning for radiotherapy of unresectable lung cancer has also been explored and may provide improved treatment with a reduced incidence of relapse outside the radiotherapy field. [25] Radiotherapy treatment planning incorporating PET defined target volumes have indicated that accurate dosimetry using PET/ CT fusion defined volumes is highly dependant on accurate target segmentation to improve local tumor control and reduce normal tissue toxicities. [26]PET/CT fusion in Radiation Therapy Planning With regard to radiation therapy, PET/CT may be particularly useful because, in addition to the typically excellent staging afforded by PET/CT before treatment, the CT data from a PET/CT examination can be used for radiation therapy planning, provided the CT data are properly acquired. [27],[28] PET has a considerable effect on the decision-making process prior to radiation therapy planning. These treatment changes include prevention of inappropriate radiation therapy and changes in the intent regarding curative versus palliative radiation therapy, the radiation dose, or the planning target volume. [27] When PET data are used in addition to CT data for planning, there is much better agreement to include known regions of micro metastatic spread and a safety margin. The effect of PET for radiation therapy planning on the definition of the planning volume may be more relevant in lung carcinoma where it is difficult to distinguish tumor from atelectasis. The key question of the effect of PET/CT in radiation therapy planning is whether extension of the planning treatment volume on the basis of PET/CT fusion data will improve patient survival. This is an area to be studied as right now there is no data available currently.Monitoring Response of Tumor to Therapy An emerging area of clinical utility of PET/CT fusion images are in the monitoring of tumor response to therapy, principally with 18 F-FDG. PET/ CT fusion images are more helpful in differentiating fibrosis from recurrent tumor in treated sites and metastatic lung disease as positron emission tomography shows the metabolism of the tumor cells while the computed tomography images show the anatomic localization of the disease. Accurate assessments of response to chemotherapy and radiation therapy often, preceding CT scan changes, have been reported not only in lung carcinoma but also in glioma, colorectal carcinoma, lymphoma, head and neck tumors and soft tissue sarcomas. [28] The implications of this approach are significant in terms of optimizing treatment regimens, minimizing unnecessary morbidity and reducing costs.Conclusion Positron emission tomography with computed tomography fusion (PET/CT fusion) images has emerged as a powerful diagnostic tool in the management of patients with lung cancers. The published literature has provided evidence of the superior utility of 18 F-FDG PET/CT fusion over conventional imaging methods in the staging of lung cancers, in monitoring disease recurrence and in changing patient management to more appropriate therapy. The methods for evaluating the efficacy of PET/ CT fusion remain complex particularly as the evidence based approach of randomized controlled trials may not be appropriate for imaging technologies. With analysis and discussion, it appears that PET/CT fusion has the potential to dramatically improve our ability to manage the patients with lung cancer and is contributing to our understanding of cancer cell biology and in development of new therapies. It also raises issues that need to be further investigated for further advances in the management of lung cancer patients with high risk, characterization of prognostic factors, improved patient selection, and continued refinements in therapeutic approach.References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08042f5.jpg] [cn08042f4.jpg] [cn08042f2.jpg] [cn08042f3.jpg] [cn08042f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}