 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
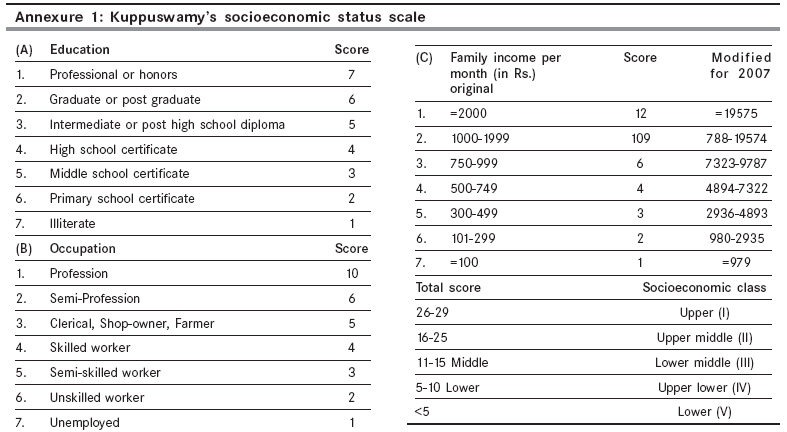
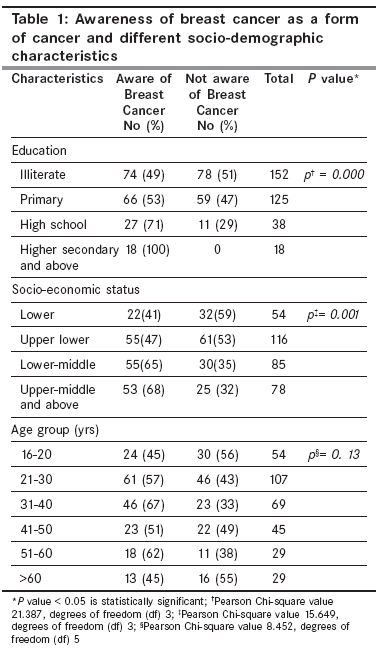
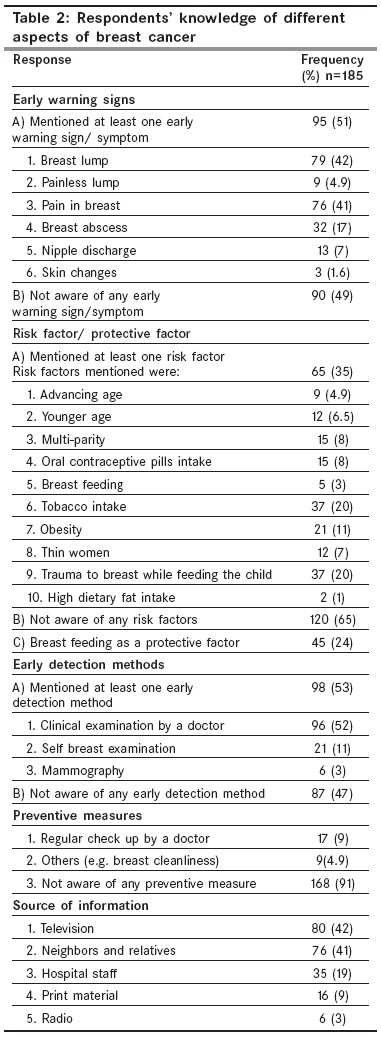
Indian Journal of Cancer, Vol. 45, No. 4, October-December, 2008, pp. 149-153 Original Article Awareness of breast cancer in women of an urban resettlement colony Somdatta P, Baridalyne N Centre for Community Medicine, AIIMS, New Delhi-110 029 Code Number: cn08044 Abstract Background: Breast cancer accounts for 19-34% of all cancer cases among women in India. There is a high mortality due to late stage diagnosis as patients usually present at an advanced stage because of lack of awareness and non-existent breast cancer screening programs. Keywords: Awareness, breast cancer, India, urban resettlement colony Introduction In India cancer prevalence is estimated around 2.5 million, with over 0.8 million new cases and 0.5 million deaths occurring each year. [1] The common sites for cancer in India are oral cavity, lungs, esophagus and stomach in males and cervix, breast and oral cavity among females. Breast cancer accounts for 19-34% of all cancer cases among women in India. [2],[3],[4] According to National Cancer Registries and Regional Cancer Centers, it is the commonest cancer amongst women in Delhi, Mumbai, Ahmedabad, Kolkata and Trivandrum. [2],[3],[4],[5],[6] In all other cancer registries, it is listed as the second most common cancer among women. Moreover, data from national and regional cancer centers from 1984 to 2002 also show that there is an increase in the incidence of breast cancer and found to be gradually overtaking cancer of the cervix. Most of the patients seek medical advice when the disease is fairly advanced. Over 70% of the cases report for diagnostic and treatment services in advanced stages of the disease, resulting in poor survival and high mortality rates. [7] Early Breast Cancer (EBC) constitutes only 30% of the breast cancer cases seen at different cancer centers in India whereas it constitutes 60-70% of cases in the developed world. [8] In India the incidence/mortality ratio is 0.48 compared with 0.25 in North America. [9] Late diagnosis is a major factor for this high mortality as most patients present in advanced stage of the disease. This is attributed to lack of awareness and non-existent breast cancer screening programs in India. As breast cancer is a topic that is not freely discussed in India because of cultural taboo, there is an urgent need for information and education on awareness of breast cancer and its early detection measures. Keeping in mind that October is observed worldwide as Breast Cancer Awareness Month, this study was planned in October 2007 to find out the awareness about breast cancer among women in an urban resettlement colony in Delhi. Materials and Methods A cross-sectional community based survey was conducted at Dr Ambedkar Nagar, New Delhi, which is a resettlement colony. (A resettlement colony is defined as a colony created by removing a group of households from the congested city core or an encroachment in public places and locating them generally in the periphery of the city). The study area is the field practice area of Department of Community Medicine of a Medical College of Delhi. The urban health program of this medical college runs in a resettlement colony in south Delhi, which is around eight kilometers from this medical college. Six blocks in this area have been adopted by this college. Every morning the urban health team consisting of doctors, Public health Nurse, pharmacist, Medical Social Worker and laboratory technician, run a mobile clinic and thus provide medical services in this region. Besides, regular home visits are made by multipurpose workers in the assigned blocks. One block out of the six blocks was randomly selected for the study. In order to calculate the sample size, we referred to a study carried out in an urban slum area of Delhi, [10] which reported that 51% of the participants had some knowledge regarding cancer in general. Therefore, based on this study, as we could not find any data about awareness of breast cancer, we assumed a prevalence of 50%, and an absolute error of 5%, the sample size was calculated to be 400 with power 80% and confidence level 95%. The study participants included all women aged 15 years and above, residing in the selected block for the last six months. Data were collected from October 2007 to December 2007. The study participants were recruited from the consecutive houses. A pre-tested semi-structured interview schedule was administered to collect information regarding various aspects of breast cancer such as early warning signs, risk factors, early detection measures and their source of information. The Modified Kuppuswamy scale [11] was used for assessing the socio-economic status (SES) of the family [Annexure 1]. Ethical issues Analysis of data Results A total of 358 women were contacted for the study. Twenty-five women (6.9%) refused to participate. Thirty-two houses were found locked and in another eighteen houses no respondents were found. Out of 333 women who participated in the study one third were in the age group of 21-30 years [Table - 1]. The mean age of the study participants was 36 years ±15.1, the range being 16 to 80 years. Forty-six percent of the study participants were illiterate. About one third (34%) of the population, belonged to the upper-lower socioeconomic status. Awareness about breast cancer Knowledge of signs and symptoms Knowledge about risk factors Knowledge about early detection methods Knowledge about preventive measures Source of information Discussion Till now there is no established national screening program for breast cancer in the country. In the present study we found that only 56% of the respondents were aware of breast cancer as a disease. Those who were aware were of higher socio-economic strata or the more educated. It has been shown that women of low SES have a low incidence of breast cancer compared to women of higher SES, but they experience a higher mortality rate, due to higher late stage diagnosis. [12] Reports from other studies also show that educated women are more aware of breast cancer. [13],[14] In this study very few women correctly identified early warning signs of breast cancer; especially such sign as a painless lump which is similar to results of studies done in Nigeria. [13],[15] Knowledge and awareness of early detection measures of breast cancer such as breast self-examination (BSE) is also low. The findings show that few of the participants knew about BSE as an early detection measure, and hardly very few women practice it. It is established that screening by mammography can substantially reduce mortality from breast cancer, especially in women over the age of 50 years. [16] But this technique is expensive and for this reason difficult to adopt in a country like India as a routine public health measure. A cohort study in Finland [17] and a case-control [18] study in Canada suggested BSE to be beneficial (reduction in breast cancer mortality) at all ages. Recently there is a debate on the role of regular self-examination of the breast in preventing breast cancer mortality. [19] However the teaching of BSE can help women to be alert to any abnormal changes in their breasts and seek medical advice immediately. One study carried out in Karnataka has suggested that this can be used as a strategy for creating breast health awareness among women, and female health workers can be trained to teach the women to carry out BSE. [20] The World Health Organization stresses on promoting awareness in the community and encouraging early diagnosis of breast cancer, especially for women aged 40-69 years who are attending primary health care centers or hospitals for other reasons, by offering clinical breast examinations. [21] We acknowledge certain limitations of this study: Firstly, we do not have information about women who refused to participate in the study or who were not available at the time of study. If the women who were not included in the study were different from those who were interviewed in some characteristics like age, the results of the study may have been different, since age is expected to be an important determinant of awareness but it has not come out to be significant in our study. Secondly, though we had calculated a sample size of 400, due to time constraints and logistic reasons we could only enroll 358 women. Thirdly, as this study was done in one of the blocks of a resettlement colony of south Delhi, the findings of this study could not be generalized to Delhi. In conclusion, this study has shown that women of this resettlement colony have poor knowledge about breast cancer be it about risk factors, warning signs, or early detection procedures. Therefore it is important to create awareness and educate the community and to remove the misconceptions associated with ignorance through community based educational/awareness campaign. Early warning signs, significance of a painless lump need to be emphasized. Educating health care workers is also very important aspect. We also have to keep in mind only campaigns will not be enough, information need to be disseminated in a form which is appealing to the community. We recommend the establishment of policy guidelines that will enhance adequate and urgent dissemination of information about breast cancer to all women. References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08044t2.jpg] [cn08044a1.jpg] [cn08044t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}