 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
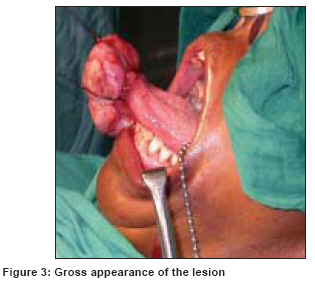
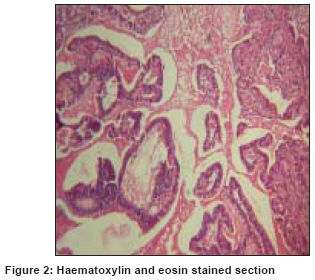
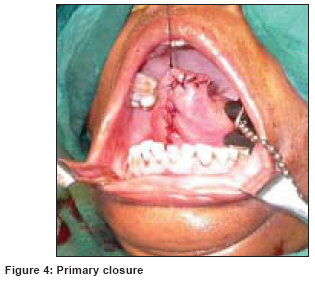
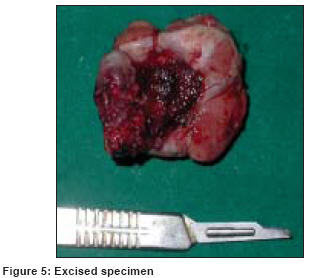
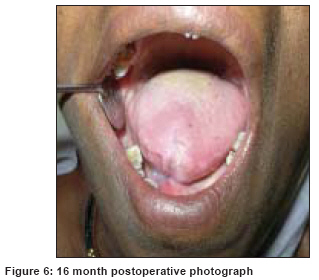
Indian Journal of Cancer, Vol. 45, No. 4, October-December, 2008, pp. 176-178 Case Report Ductal adenocarcinoma of ventral surface of the tongue: An unusual presentation Halli R, Kini R, Bither S Department of Oral and Maxillofacial Surgery, Christian Dental College, Ludhiana - 141 008, Punjab Code Number: cn08050 Abstract There are very few cases reported of adenocarcinoma of the tongue. We report an unusual case of a 60-year-old female having a large, pedunculated ductal adenocarcinoma that had arisen from ventral surface of the tongue. The lesion was managed by surgery.Keywords: Ductal adenocarcinoma, pedunculated, ventral tongue Introduction In the literature on salivary gland tumors the term ′adenocarcinoma′ is frequently used as a generic designation of a large group of neoplasms. [1] Ductal adenocarcinoma is a slow growing malignancy occurring mainly in minor intra-oral salivary glands, particularly the palate. Following the criteria set out in, for example, the WHO blue book, it is usually fairly easy to recognize them by microscopy. [2],[3] The presentation of the lesion from the ventral surface of the tongue is a rare one and to our knowledge there has not been any previous report in the literature. We present an unusual and rare presentation of ductal adenocarcinoma arising from the ventral surface of tongue. Another unusual thing is absence of palpable neck nodes. Case Report A 60-year-old female presented with a 45-day history of difficulty in swallowing and a seven-day history of difficulty in breathing and inability to speak properly. She gave a positive history of tobacco use and ′mishri′ application. Intraoral examination revealed a 6.5 X 3.5 X 4 cm pedunculated mass arising from the ventral surface of the tongue. The surface of the lesion was smooth and covered with normal mucosal texture [Figure - 1],[Figure - 3]. The lesion was firm and painless and had increased in size. It was resting over the dorsal surface of tongue, obstructing the oro-pharynx and the patient was not able to close her mouth completely. Incisional biopsy was obtained from the lesion, which revealed it to be a ductal type of adenocarcinoma [Figure - 2]. The lesion was excised from its base, under general anesthesia and primary closure achieved [Figure - 4],[Figure - 5]. At 16-month postoperatively the patient is symptom free [Figure - 6]. Histopathology The tumor cells have a deceptively uniform appearance. The cells can exhibit different growth patterns - polymorphous; includes solid nests and trabeculae, tubules, papillae, cyst, cribriform or pseudoadenoid cystic formations, strands and fascicles. Combinations and transitions among these patterns are frequently seen. Discussion Histologically, ductal adenocarcinoma of minor salivary gland is characterized by its morphological variability, cytological baldness and an infiltrative growth pattern.[4] WHO classification of head and neck tumors 2005 distinguishes it to be a separate entity. [5] Tumors with a conspicuous papillary component are associated with higher incidence of lymph node metastasis and rarely ductal adenocarcinoma may undergo transformation to a high grade tumor. [6] Differential diagnosis includes adenoid cystic carcinoma, monomorphic adenoma, pleomorphic adenoma and papillary cystadenocarcinoma. [4],[6] The ductal adenocarcinoma can metastasize to neck nodes, which require neck dissection along with surgical excision followed by radiotherapy. There has to be a long-term patient follow-ups as the mortality rate associated is high and prognosis is poor. References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08050f6.jpg] [cn08050f4.jpg] [cn08050f2.jpg] [cn08050f5.jpg] [cn08050f3.jpg] [cn08050f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}