 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
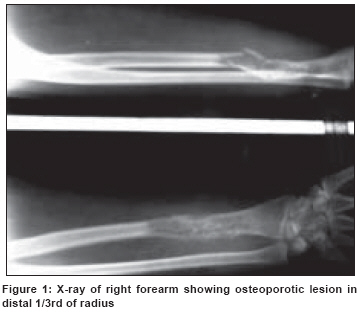
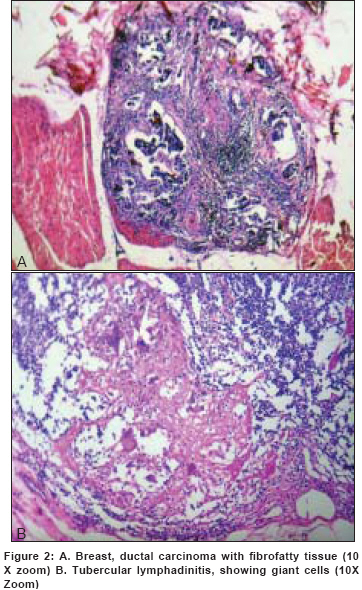
Indian Journal of Cancer, Vol. 45, No. 4, October-December, 2008, pp. 182-184 Letter To Editor Ipsilateral axillary tubercular lymphadenopathy, contralateral osseous tuberculosis in a case of ductal carcinoma of breast Wani BN, Jajoo SN Department of Surgery, Jawaharlal Nehru Medical College, Sawangi (Meghe), Wardha-442 004, Maharashtra Code Number: cn08053 Dear Sir, The coexistence of breast cancer and tuberculosis has been described in over 100 cases [1],[2],[3],[4],[5],[6] however its coexistence in the axillary node is rare. [1],[4],[5],[6] We present a case of, 43-year-old housewife presented with complaint of diffuse swelling over right distal forearm associated with dull pain of 4 months duration, for which she received conservative management but without relief. Around a month later she developed pathological fracture in the forearm after following trivial trauma. [Figure - 1] Following FNAC report that suggested the lesion to be of chronic granulomatous lesion she was started on antibiotic therapy and at the same time underwent fixation of the fracture by interlocking nail. Her all hematological and biochemical tests were normal. To rule out tuberculosis versus malignancy, the bone scan with 20 ml of tracer was performed and it showed hot spots involving right radius, the findings consistent with post-operative status and rest all bones showed physiological distribution of tracer. Serum IgG, IgM, IgA levels for Mycobacterium Tuberculosis were found to be within normal limits. For HIV, IgM antigen was reactive and IgG non-reactive but status confirmed negative by Western Blot technique, but window period could not be but ruled out. Mammography, X-ray chest, USG abdomen were found to be normal. After consultation with second orthopedic surgeon, she underwent removal of right radial nail with excision of growth with fibular graft. Grossly cut section of specimen showing hemorrhagic cavity with friable bone. Histopathological examination of the excised tissue showed numerous granulomas, epitheloid cells, Langhan′s giant cells at places and caseation necrosis, the findings consistent with tuberculosis. However she further noticed solitary, non-tender, firm lump situated in the lower medial quadrant of the left breast, which measured 2 x1.5 cm, having restricted mobility adherent to skin and also 5 th costal cartilage. Right axilla revealed enlarged lymph nodes in the anterior, central and apical groups, four in number, largest measuring 1x1.5cm. They were firm, non-tender, discrete and mobile. The right breast, right axilla and supraclavicular fossa were normal. Other systems revealed no abnormalities. A clinical diagnosis of carcinoma of left breast with TNM (tumor, node and metastasis) stage T1N1M0 was made. FNAC from lump in left breast suggestive of Ductal carcinoma, so underwent for left modified radical mastectomy with axillary dissection of 18 nodes. Histopathology of breast lump [Figure 2A] showed grossly scirrhous irregular lump, fibrofatty mass, gritty grey white tumor mass; microscopically invasive duct cell carcinoma with diffuse infiltration of tumor in fibromuscular and fatty tissue. Modified Richardson bloom score 5; suggestive of Invasive ductal carcinoma with well differentiated grade I, with clear margins. There was no evidence of tubercular foci in the breast specimen. Borders of lump, skin, apical tissue free from malignancy and all 18 axillary lymph nodes dissected out of which all negative for metastasis; but 6 positive for tuberculosis [Figure 2B]. In the postoperative period, the patient was started on chemotherapy with CMF (Cyclophosphamide, Methotrexate, 5-Fluorouracil) regimen while awaiting the status of estrogen/progesterone receptors that turned out to be negative. Following this the Methotrexate was changed to Adriamycin for a total of 6 cycles along with anti tubercular chemotherapy (Rifampicin-450mg, Isoniazide 300 mg, Pyrazinamide 1000 mg, Ethambutol-800 mg and Pyridoxine 40 mg for initial three months to followed by Rifampicin and Isoniazide for nine months). Follow-up is going on. In our case the involvement of the contra lateral lymph nodes can be explained by the facts that hematogenous spread from an obvious [5],[6] or sub clinical focus can lead to the systemic spread and involvement of the other organs. [4] A possibility of tuberculosis should always be borne in mind especially in patients from endemic areas. [2] The simultaneous occurrence of carcinoma and tuberculosis can lead to many problems regarding diagnosis and treatment. [3] References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08053f1.jpg] [cn08053f2.jpg] |
| |||||||||

{kind=link}
{kind=link}