 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
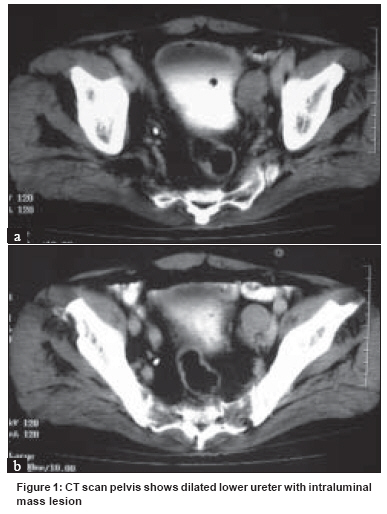
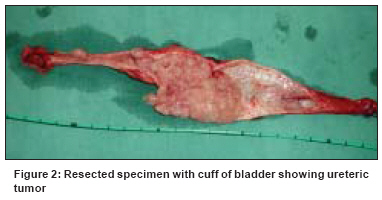
Indian Journal of Cancer, Vol. 45, No. 4, October-December, 2008, pp. 184-185 Letter To Editor Transitional cell cancer of ureter misdiagnosed as pelviureteric junction obstruction: Pitfalls of standard diagnostic tools Goel A, Singh D, Goel A Department of Urology, King George's Medical University, Lucknow - 226 003 Code Number: cn08054 Dear Sir, Upper urinary tract urothelial tumors (UUT) are uncommon, accounting for about 5-7% of all renal tumors and about 5% of all urothelial tumors. [1] Ureteral tumors are even more uncommon, occurring with one-quarter the incidence of renal pelvic tumors. [2] It is estimated that 2,290 new cases will be reported in United States of America in 2008. [3] A 70-year man presented with dull-aching flank pain of 4-months duration and a single episode of total hematuria. Evaluation revealed normal renal functions, left gross hydronephrosis on ultrasonography, and normal urine cytology. An intravenous urogram revealed normal right kidney while the left side was nonvisualized. Renal scintigraphy showed normal right kidney and nonfunctioning left kidney. Suspecting him as a case of left nonfunctioning kidney due to ueteropelvic junction obstruction (UPJO), transperitoneal laparoscopic nephrectomy was done. Six months later the patient again experienced hematuria. Repeat ultrasonography, urine cytology, and cystoscopy were normal. Suspecting benign prostatic enlargement as cause of hematuria, dutasteride and tamsulosin treatment was started. The patient experienced hematuria again after three months. Cystoscopy done at this time revealed bloody efflux from the left ureteric orifice. CT scan revealed left mid-ureteric tumor [Figure 1a] and [Figure 1b]. The patient was subjected to excision of the ureteric stump with cuff of bladder [Figure - 2]. The biopsy revealed transitional cell carcinoma grade II with invasion of muscularis mucosa (stage T1N0M0). The patient is under regular follow-up (two-year follow-up) and there is no evidence of recurrence or distant metastasis. Primary UUTs are relatively uncommon [1] and sometimes difficult to diagnose. Urine cytology is useful for the diagnosis of UUT, although not very sensitive in low and moderate grade tumors. The sensitivity of voided urine cytology is related to tumor grade and overall accuracy estimates of the sensitivity of cytology have ranged from about 20% for grade 1 tumors to 45% and 75% for grade 2 and grade 3 tumors, respectively. [4] Intravenous urography has been the traditional method for diagnosing UUTs but as the kidney was nonvisualized, no filling defect could be demonstrated. Ultrasonography is generally not considered a sensitive tool for detecting ureteral pathology. A CT scan may miss small urinary filling defects (< 5 mm) between the ′cuts′. The greatest downside of CT or MRI is in the detection of small lesions that may be lost in volume averaging. [5] We did not perform CT scan as none of the investigations initially suggested malignancy. A retrograde pyelography (RGP) could have had been diagnostic but was not performed because of its invasive nature and because there was no other cue toward a diagnosis of UUT. As the patient was subjected to laparoscopic simple nephrectomy (only 2-3 cm of ureter below the ureteropelvic junction is removed with the kidney) the diagnosis of ureteric tumor was missed on histopathology also. Hematuria, either spontaneous or associated with otherwise minor trauma, may also be an initial symptom of UPJO. We misdiagnosed this case as UPJO giving rise to nonfunctioning kidney, as this condition is more common and frequently encountered by urologists. Upper tract urothelial cancers are often associated with a poor prognosis. [6] The thin muscle layer of the renal pelvis and ureter probably allows earlier penetration of UUT through the thinned muscle layer than is seen in bladder cancers. [6] Obstruction of the urinary tract is also considered a poor prognostic sign for tumor invasion. [6] This patient had a relatively benign clinical course which is unusual. This case highlights the pitfalls of the standard investigations all of which missed the diagnosis of UUT. We now feel that diagnostic suspicion for this uncommon condition with an initial CT scan or RGP could have diagnosed this case earlier. Any patient presenting with hematuria should warrant a through evaluation to rule out cancer, especially in elderly. References
Copyright 2008 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn08054f2.jpg] [cn08054f1.jpg] |
| |||||||||

{kind=link}
{kind=link}