 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
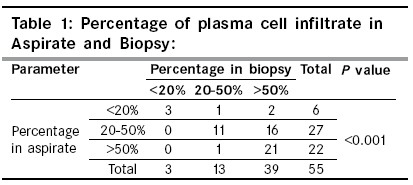
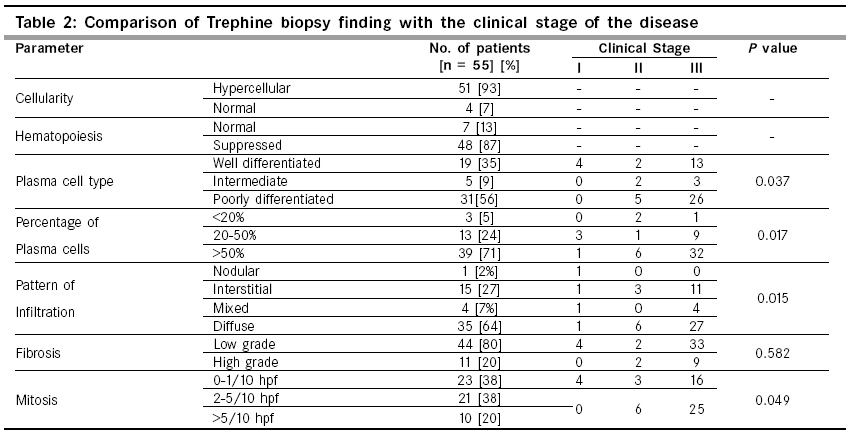
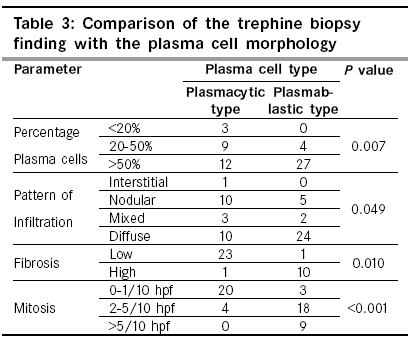
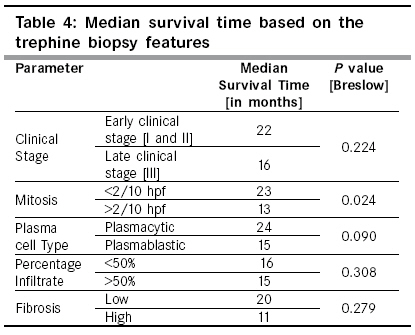
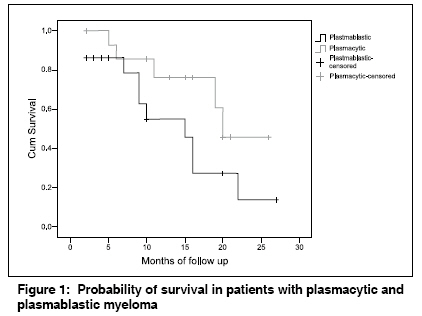
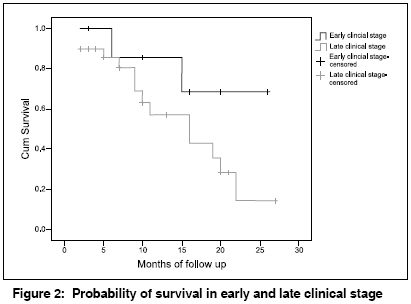
Indian Journal of Cancer, Vol. 46, No. 1, January-March, 2009, pp. 40-45 Original Article Prognostic significance of bone marrow histology in multiple myeloma Subramanian R, Basu D, Dutta TK Department of Pathology, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry Code Number: cn09007 Abstract Background: Bone marrow examination continues to be the cornerstone for establishing the diagnosis of multiple myeloma in association with other clinical and laboratory parameters. Plasma cell morphology has significant correlation with clinical stage and survival.Aims: To note the bone marrow histology in detail in multiple myeloma and to correlate it with clinical stage and survival. Methods and Material: Fifty-five cases of multiple myeloma diagnosed between January 2001 and December 2006, who had a bone marrow aspiration and biopsy done at the time of diagnosis were included in the present study. Statistical Analysis: SPSS software version 13.0 was used. Clinical stage and plasma cell morphology were correlated using chi square test and Spearman's correlation coefficient. Survival analysis was done using the Kaplan-Meier method. Results: Seventy-six percent patients were in clinical stage III, 17% and 7% were in stage II and I respectively. The clinical stage correlated significantly with plasma cell morphology, percentage of plasma cell infiltration and pattern of infiltration. Plasma cell morphology correlated significantly with bone marrow parameters like percentage infiltrate, pattern of infiltration, degree of fibrosis and mitotic activity. Patients in advanced clinical stage, >50% plasma cells in the marrow, diffuse pattern of infiltration, high mitosis and increased fibrosis had a shorter median survival than patients with favorable features. Conclusions: It is recommended that the bone marrow histology be studied in detail in multiple myeloma at diagnosis since it correlates well with the clinical stage and offers useful prognostic information. Keywords: Bone marrow, multiple myeloma, prognosis, survival, trephine biopsy. Introduction Multiple myeloma is a well established clinical and immunological entity with considerable variability in biological behavior and survival. [1] Bone marrow examination continues to be the cornerstone for establishing a diagnosis in association with other clinical and laboratory parameters. [2] Several clinical, laboratory and histological/cytological variables help us in determining the prognosis of the disease. [1],[3],[4],[5],[6],[7] The first histological classification and staging of multiple myeloma, based on the bone marrow trephine biopsy, was put forward by Bartl et al. in 1987. [3] The Durie and Salmon clinical staging system, proposed in 1977, [8] is still being used today, though it has been replaced by the ISS staging at many places. [9] Prognostic markers like beta 2 microglobulin and Interleukin-6 (IL-6) are not available in most centers in developing countries like India. Histological parameters that have a definitive prognostic significance in multiple myeloma are the percentage of myeloma cells in the marrow, pattern of infiltration, degree of plasma cell atypia, marrow fibrosis and mitotic index. [5],[6],[7] There have been very few studies from India evaluating bone marrow histology of plasma cells in myeloma. [10],[11] The current study presents an approach to evaluate the histological features in the bone marrow trephine biopsy in multiple myeloma which could be of use in prognostication.Materials and Methods Fifty-five patients with multiple myeloma diagnosed between January 2001 and December 2006 who had an adequate bone marrow aspirate smears and trephine biopsies were included in the current study. All patients had undergone a bone marrow aspiration and biopsy at the time of diagnosis. Clinical details and biochemical parameters were noted and all patients were clinically staged as per the Durie and Salmon staging system. [8] All the aspirates and biopsies were reported by the same author (DB) as per departmental protocol. Percentage of plasma cells in the aspirate was estimated by a 500-cell count. Trephine biopsy was decalcified in 1% acetic acid. Trephine biopsy was referred to as adequate if the trephine had at least 3 marrow spaces below the sub-cortical space and the aspirate had a good number of particles with cellular trails. In addition to the routine parameters, the biopsies were studied in detail for percentage of plasma cell infiltrate (< 20%, 20-50%,> 50%), pattern of infiltration (nodular, interstitial, mixed and diffuse), mitotic activity (0-1, 2-5,> 5/10 high power field) and plasma cell morphology. The criteria put forward by the German myeloma task force was used by us to type the plasma cell morphology into well differentiated, intermediately differentiated or poorly differentiated plasma cells. [7] Mitosis was counted in 20 high power fields showing plasma cell infiltration in the biopsy and was categorized as 0-1/ 10 hpf, 2-5/10 hpf and> 5/10 hpf. Fibrosis was graded between grade 0 and 3 as per the European Consensus method. [12] Following a diagnosis of multiple myeloma, all patients were put on a treatment regimen comprising Thalidomide and Dexamethasone. For statistical analysis, SPSS software version 13.0 was used. The clinical stage and plasma cell morphology were correlated with other bone marrow parameters using chi square test and Spearman′s correlation coefficient. Survival analysis was done using the Kaplan-Meier method. For the purpose of analysis, well differentiated and intermediate type of myeloma cells were grouped together as the plasmacytic type, and the poorly differentiated type of myeloma cells were called the plasmablastic myeloma cells. Similarly, a mitotic activity of < 2/10 hpf was taken as low mitotic activity and> 2/ 10 hpf was considered as high mitotic activity. Results The age of the patients ranged from 35 to 74 years with a median age of 55 years. There was a male preponderance with a male to female ratio of 1.9:1. Bone pain and easy fatigability were the most common symptoms seen in 82 and 73% respectively, followed by renal failure in 36% cases. Five patients presented with plasmacytomas in whom further investigations lead to a diagnosis of multiple myeloma. Seventy-one percent patients had a Hb value < 8.5g/dl. Nine patients had platelet count < 100 x 10 9 /l. Five patients had pancytopenia. Peripheral smear examination showed rouleaux formation in 91% cases and erythrocyte sedimentation rate (ESR) was raised in all cases. Forty-two cases (76%) were clinically in Stage III. Only 17% were in stage II and 7% in stage I disease. Bone marrow aspirate smears showed a hypercellular marrow in 89% cases with suppressed normal hematopoiesis in 70% cases. Twenty-one cases (40%), showed a plasma cell percentage of> 50% in the bone marrow aspirate. Bone marrow biopsy showed a hypercellular marrow with suppressed hematopoiesis in nearly 90% of the cases. In striking contrast to the aspirate, the biopsy showed> 50% plasma cells in 71% cases. This difference was very significant ( P < 0.001) and is represented in [Table - 1]. Fifty-six percent of the cases had poorly differentiated plasma cell morphology and nearly two-thirds of the cases had a diffuse pattern of infiltration. The findings on trephine biopsy are tabulated in detail in [Table - 2]. On comparing the clinical stage of the disease with the bone marrow histological features, it was found that the morphological subtype of plasma cells ( P = 0.037), the percentage of plasma cells in the marrow ( P = 0.017), the pattern of infiltration ( P = 0.015) and the mitotic activity of the plasma cells ( P = 0.049) correlated significantly. This data is represented in [Table - 2]. Correlating the plasma cell morphology, which is a well established prognostic marker, with the other bone marrow histological features, it was seen that patients with a poorly differentiated plasma cell morphology, had more often> 50% plasma cell burden in the marrow, a diffuse pattern of infiltration with increased mitosis and a higher degree of fibrosis. The data was significant for plasma cell percentage ( P = 0.007), the pattern of infiltration ( P = 0.049), marrow fibrosis ( P = 0.010) and mitotic activity of plasma cells ( P = < 0.001). This is represented in [Table - 3]. Follow up data were available for 37 cases. Median survival time, while shorter in each of the unfavorable histological categories, was statistically significant only for increased mitosis [Table - 4]. Patients with plasmacytic (i.e. well differentiated and intermediately differentiated combined) morphology had a median survival time of 24 months compared with 15 months for patients with a poorly differentiated morphology. Overall, there were seven patients with all histological unfavorable features, i.e. plasmablastic myeloma,> 50% marrow infiltrate, mitotic activity of> 2/10 hpf showing a diffuse pattern of infiltration. The median survival time of these patients was just nine months. The data however were not significant, as the number of patients in each group was very small. The probability of survival at the end of two years for a patient with plasmacytic morphology was found to be around 50%, whereas for a patient with plasmablastic morphology it was only 15% as shown in [Figure - 1]. Similarly, for patients in early clinical stages the probability of survival at the end of 2 years is 70%, whereas for patients in late clinical stage it is 10% as shown in [Figure - 2]. Discussion Multiple myeloma is the most common primary malignancy of the bone and has an incidence of 4.5 per 100,000 population per year in the United States. [13] Most staging systems are based on clinical and/or laboratory findings that reflect the tumor cell mass or the secondary effects of the malignancy, and not on the nature of the plasma cells in the marrow. [2] Bartl et al . had proposed a staging system based on the histological features of the bone marrow trephine biopsy and had shown a high prognostic relevance of the morphological features. [1],[6] However, to date no standard criteria based on the bone marrow biopsy have been devised to reliably predict prognosis. The most common clinical features seen were bone pain and fatigue, which is much higher than that reported by Bartl et al. , which reflects that the majority of our patients present late. [6] We had 76% in stage III, Bartl et al . had only 57% in clinical stage III, [7] Pich et al . had 58%, [14] whereas Sukpanichnant et al. had nearly 65% in stage III. [5] Anemia in myeloma is directly related to the percentage of plasma cell infiltrate in the marrow. [1],[4] In fact, absence of anemia was considered to be a favorable prognostic factor in the long-term survival of myeloma patients by Tsuchiya et al . [15] One particular problem we faced was regarding the quality of the biopsy. Since most of our patients had presented in clinical stage III with multiple ostelytic lesions, the bone was fragile and hence the marrow specimens were generally friable. We had to exclude ten patients from our analysis due to inadequate number of marrow spaces. In some of the patients we required multiple attempts to get a trephine biopsy of an adequate length. In the present study, we observed that 71% of the patients had> 50% plasma cell infiltrate in the biopsy, compared to only 40% in the aspirate, which was very significant ( P < 0.001), i.e. the aspirate had underestimated the plasma cell burden. Pich et al . had found that the mean percentage of plasma cell infiltrate was higher in the biopsy (50.3%) than in the aspirate (32.89%). [14] Terpstra et al . in 1992 had also stated that in 40% of the cases the biopsy tends to show a higher percentage of infiltrate than the aspirate. [16] A similar observation was also made by Singhal et al . from India. [11] Although Romanowsky stained aspirate smear examination is the traditional and rapid method for plasma cell quantification, it is subject to various pre analytical and analytical variables. [17] These include poorly representative bone marrow aspirate specimen affected by technical problems like blood dilution or sample clotting. Sampling variability is also encountered due to focal disease distribution. [17] Thus the exact extent of marrow involvement is better appreciated on a biopsy. There were seven cases that showed a diffuse plasma cell infiltrate, with the surrounding marrow spaces showing an interstitial infiltrate in the same biopsy. In all of them, the percentage of plasma cell infiltrate was 10-30% less in the aspirate compared to the biopsy. Fibrosis in myeloma at the time of diagnosis has not been studied in detail by many authors. Subramanian et al . had observed that increased fibrosis correlated significantly with the plasma cell morphology and mitotic activity of plasma cells and these patients had a median survival time of just 11 months. [18] The criterion for the plasma cell differentiation we used was the same as that proposed by Sailer et al . [7] Poorly differentiated myeloma [plasmablastic myeloma] is known to have poor prognosis. [1],[5],[7] When the morphology of the plasma cells was compared with the clinical stage of the disease it was seen to be statistically significant ( P = 0.037). Nearly 62% (26/42 cases) of patients in stage III had poorly differentiated plasma cells and 84% (26/31 cases) of the patients with poorly differentiated plasma cells were in stage III. Sukpanichnant et al. [5] had also reported that 66% of the patients with a plasmablastic myeloma were in stage III disease. When the plasma cell morphology was compared with other bone marrow parameters, it was observed that there was good correlation between percentage infiltration of the marrow, pattern of infiltrate, degree of fibrosis and the proliferative activity (as calculated by mitosis). However, when a multivariate analysis was done, none of the parameters were found to be statistically significant. Sailer et al. , by a multivariate analysis had reported that patients with poorly differentiated plasma cells tend to have> 50% plasma cell infiltrate and pattern of infiltration was either diffuse or mixed (nodular plus interstitial). [7] On reviewing the large series reports dealing with bone marrow biopsies and myeloma, it was found that a detailed analysis of the bone marrow parameters and their comparison with the clinical stage of the disease has not been done by any of the authors. [5],[6],[7],[14] This is the first study giving such a detailed analysis. We observed that the percentage infiltrate in the marrow and the pattern of infiltration was statistically significant when correlated with the clinical stage of the disease. Seventy-six percent of the patients in stage III had> 50% plasma cell infiltration and 64% of the patients in stage III had a diffuse pattern of infiltration. Fibrosis and mitosis were not found to correlate with the clinical stage of the disease, though they were significant when compared with the plasma cell morphology. Bartl et al. too had reported that a great proportion of patients in an advanced clinical stage of the disease had coarse fibrosis of the marrow. [6] For thirty-seven patients for whom follow up details were available, survival data was analyzed using the Kaplan-Meier analysis. Median time of survival for patients in an early clinical stage with well differentiated type of plasma cells, lower mitotic activity with an interstitial infiltrate of the marrow was shorter in our study compared to that reported in the western literature. This probably reflects a more aggressive course of the disease in the Indian population, or that the patients are diagnosed in an advanced stage of the disease (as reflected by the fact that the proportion of the cases in the advanced clinical stage in our study is much higher than that reported in the western literature). Median survival time of the patients in comparison to that reported by the other authors is shown in [Table - 4]. There were seven patients with all histologically unfavorable features, i.e. with plasmablastic morphology, having a diffuse pattern of infiltration with> 50% plasma cell infiltrate, along with a mitosis of> 2/10 hpf. The median survival time of these patients was just nine months. Sailer et al . had observed that patients with these poor prognostic histological features had a median survival time of 18 months. [7] Conclusion The present study emphasizes the role of a bone marrow biopsy not only in establishing a diagnosis of multiple myeloma, but also in providing prognostic information. It helps in assessing the plasma cell burden in the marrow. Parameters like morphology of the plasma cells, percentage of infiltrate in the marrow and pattern of infiltration correlate significantly with the clinical stage of the disease. Further, bone marrow parameters like the pattern of infiltrate, percentage of infiltrate and the degree of fibrosis and mitotic activity of the plasma cells correlate well with the plasma cell morphology. A larger study is advocated to devise a bone marrow based scoring system to prognosticate myeloma at the time of diagnosis. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09007t2.jpg] [cn09007t1.jpg] [cn09007f1.jpg] [cn09007f2.jpg] [cn09007t4.jpg] [cn09007t3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}