 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
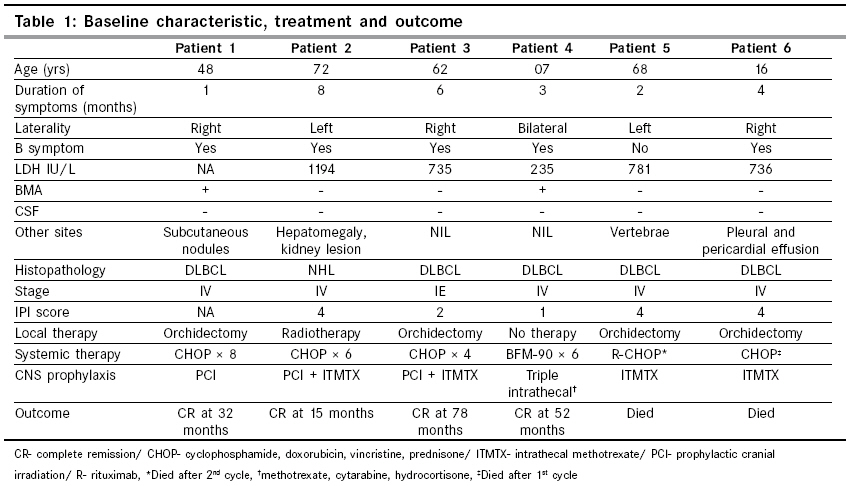
Indian Journal of Cancer, Vol. 46, No. 1, January-March, 2009, pp. 46-49 Original Article Primary testicular non-Hodgkin lymphoma: A single institution experience from India Gupta D, Sharma A, Raina V, Bakhshi S, Mohanti BK Department of Medical Oncology, BRA Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi Code Number: cn09008 Abstract Background: Primary testicular non-Hodgkin lymphoma (NHL) is an uncommon extra nodal presentation, constituting 1% of all NHL. Median age at time of presentation is 60 years. Anthracycline based chemotherapies are most frequently used. There is not enough data on use of monoclonal antibody (Rituximab) in testicular NHL.Methods: We screened approximately eight hundred and fifty NHL cases registered from January 2002 to May 2008 and found six primary testicular NHL patients. These six cases were analyzed for baseline clinical features, investigations, staging, treatment and outcome variables. Results: Median age was 55 years (range 7-72 years) and median duration of symptoms was 3.5 months (range 1-8 months). All patients had testicular swelling and abdominal lymphadenopathy. Five patients (83%) had stage IV and one had stage IE disease. Majority had diffuse large B-cell histology (83%). All patients were treated with anthracycline based combination chemotherapy and CNS prophylaxis after local therapy except one pediatric patient who did not receive any local therapy. Four patients completed therapy and are on follow up while two patients having extensive disease with poor performance status died of neutropenic sepsis after 1-2 cycles of chemotherapy. The surviving four patients achieved complete remission and are without any recurrence with a median follow up of 26 months (1-78 months). Conclusion: Primary testicular NHL is an uncommon entity and with current combined modality treatment and CNS prophylaxis, the outcome may be as good as nodal NHL. Keywords: Extranodal, non hodgkin lymphoma, testicular Introduction Non-Hodgkin lymphoma (NHL) of the testes is an uncommon extranodal presentation with incidence rates of 0.06 to 0.09 per 100,000 persons and accounts for about 1% of all NHL. [1],[2],[3],[4] The disease typically presents in patients aged over 60 years and is the most common testicular tumor in patients older than 60 years. [4],[5] Right and left sided testicular involvement is equal in frequency and approximately 6% of testicular lymphomas will have bilateral involvement. Most patients present with limited stage; stage I (59.1%), stage II (15.3%), stage III (6.0%) and stage IV (19.6%). [3] Historically, prognosis is poor after surgery alone and addition of postoperative radiotherapy improves 5-year survival up to 50-60%. [2] Chemotherapy with anthracycline-containing regimens is the recommended therapy after orchidectomy and improves survival beyond that achieved by orchidectomy and radiotherapy combined. [2],[6],[7] Testicular NHL has shown tendencies to relapse in central nervous system (CNS), contra lateral testis and less commonly lung, skin, bone, adrenal glands, liver, gastrointestinal tract and nodal sites. [2],[6],[7] Over the years, treatment for primary testicular lymphoma has been variable and survival rates are improving, probably due to multimodality treatment strategies and incorporation of rituximab in standard therapy. [3],[4] Use of anthracycline-based chemotherapy and multimodality treatment are independent predictors of survival. [3],[6] In this retrospective study we analyzed baseline characteristics, treatment modalities and survival of six cases of primary testicular non-Hodgkin lymphoma seen at our center from January 2002 to May 2008. As this is a rare disease, there is scarcity of data from the Indian subcontinent and this is the first single institution series from our country.Materials and Methods We screened all NHL cases registered from January 2002 to May 2008. There were approximately 850 NHL registered, of which we could find six primary testicular NHL patients. The demographic details, presenting features, clinical details, investigations, treatment, response and outcome were recorded from the case records. Remission status was defined as per standard criteria. Complete remission was defined as complete absence of disease. The date of death, due to any cause, was taken into account to calculate overall survival (OS).Results Median age was 55 yrs (range 7-72 yrs) [Table - 1]. Three patients had right testis involvement; two with left side involvement and one patient (patient 4) had bilateral testicular disease. Median duration of symptoms was 3.5 months (range 1-8 months). All presented with testicular swelling and mild testicular pain. All patients had abdominal lymphadenopathy. Bone marrow involvement was seen in two patients; however, none had CNS involvement. Mean LDH value was 736 U/L (range 235-1194 U/L). Five patients had diffuse large B cell (DLBC) histology and in one patient further characterization could not be done. IPI score could be calculated in five of six patients and was 4 for three patients and ≤ 2 for two patients. The aim of the treatment was to use systemic chemotherapy together with local treatment and CNS prophylaxis. Four patients underwent high inguinal orchidectomy and one patient (patient 2) received radiotherapy as local treatment. Patient 4 received no local therapy. All six patients received anthracycline-based chemotherapy; four patients completed prescribed treatment and two patients died while on treatment. All six patients received central nervous system prophylaxis in the form of either intrathecal methotrexate (ITMTX), prophylactic cranial irradiation or both. Four patients completed chemotherapy and CNS prophylaxis and tolerated chemotherapy without any grade III/IV toxicity. All four patients achieved complete response after three to four cycles of chemotherapy. These four patients are on regular follow up and alive without any evidence of active disease. Median follow up is 26 months (range 1-78 months). Two patients died of neutropenic sepsis while on therapy. Both patients had extensive disease, ECOG performance status IV and international prognostic index (IPI) of 4. One of these patients had paraplegia and urethral rupture during catheterization before chemotherapy. Discussion Primary testicular lymphoma is predominantly a disease of the elderly. The median age in our study was 55 years compared to ≥ 70 years reported in other recent reports. [3],[8] Although multiple lymphoma classifications have been used in the description of testicular lymphoma, the predominant histology is DLBCL. [3],[5],[7],[9] In the largest series involving 3669 cases of testicular NHL registered with National Cancer Data Base (NCDB) from 1985 to 2004, DLBCL accounted for 77.8%. Other B cell types and T cell types were seen in 21.1% and 1.1% cases respectively. [3] In a recent series of 18 cases, immunohistochemical subtyping of testicular DLBC was attempted and it was found that majority (89%) had non germinal center subgroup (CD 10/Bcl-6 negative and MUM-1 positive) with high proliferative activity. [10] In our series five of six patients had DLBC histology. High inguinal orchidectomy alone was previously performed to treat stage IE primary NHL of the testis, but the 5-year survival rate was as low as 12% and most patients died within 2 years after systemic dissemination. Postoperative radiotherapy was introduced in the 1980s by Duncan et al. resulting in 5-year survival rates of 64% in stage I/II and 17% in stage III/IV patients. [11] In another study, CR rate of 100% and 5-year survival rate of 93% was reported with anthracycline-based chemotherapy and radiotherapy in stage I and II patients. [2] Touroutoglou et al . showed 5-year survival rates of 50% in stage I-IV patients using a similar strategy. [12] In a retrospective series of the Hellenic Cooperative Oncology Group involving twenty-six patients, anthracycline based protocols led to CR rates of 25-80% depending upon the stage of the disease. [13] We have used anthracycline-based chemotherapy in all patients and all four patients who completed therapy achieved CR and are surviving with a median follow up of 26 months. Overall survival of testicular NHL compared to nodal NHL is higher for the first 10 years of follow up. Median OS was 4.4 years for testicular NHL compared to 1.9 years for nodal NHL in a study which included patients treated between 1980-2004 ( P < 0.001). [4] CNS relapse is considered to be common, but whether prophylactic CNS directed therapy prevents relapse has not been consistently reported. In a retrospective analysis of 62 patients, 32% of relapses were in CNS and type of therapy or stage did not affect relapse rates. [14] Connors et al. reported that they encountered no CNS relapses following combined modality treatment and suggested that the chemotherapy, by promptly eradicating systemic micrometastasis, prevents later seeding of CNS. [2] In other studies chemotherapy was not shown to reduce the incidence of CNS relapses. [11],[12],[15] The presumed reason for this is the existence of blood brain barrier (BBB) which chemotherapy drugs fail to cross to enter CNS. To prevent CNS relapses, CNS directed therapies have been utilized and have shown promising results in preventing CNS recurrences. Niitsu et al. demonstrated a reduction in CNS relapses using intrathecal methotrexate and achieved 100% 5-year CNS relapse free survival in stage IE patients. [16] Since optimum CNS prophylaxis is still not defined, we used a combination of intrathecal therapy and PCI in two patients and only intrathecal or PCI in three and one patient respectively. None of our patients had CNS relapse, further confirming the hypothesis that CNS preventive therapies are effective and should be incorporated in the treatment of these patients. Recurrence in contra lateral testis has been reported in approximately 20% of cases. [7],[13] Zucca et al . in their retrospective analysis showed that continuous risk of recurrence in contra lateral testis (15% at 3 years and 42% at 15 years) is present in patients not receiving radiotherapy to contra lateral testis. They concluded that prophylactic radiotherapy to contra lateral testis was associated with better PFS (5-year PFS, 36 v 70%; P = 0.00001) and OS (5-year OS, 38 v 66%; P = 0.00001) rates. [7] None of our patients received radiotherapy to contra lateral scrotal sac but no patient has had recurrence up to the last follow up. As most patients are elderly, preserving function of normal testis is not so vital and irradiation can be used. The management of patients with testicular lymphoma presents several challenges. Because of the poor prognosis, an aggressive treatment approach is warranted. However, testicular lymphoma is predominantly a disease of older men who often have limited ability to tolerate aggressive treatment. There is no concrete data for use of rituximab in this subset of patients although there are occasional case reports. [9],[17] Even prior to the introduction of rituximab, survival and prognosis has improved over a period of time, perhaps due to use of multimodality therapy. Median survival has improved from 35.5 months to 49.5 months for those who were diagnosed between 1985-1989 and 1995-2000 respectively (p = 0.01). [3] High rates of central nervous system relapses in historical series have led to a recommendation for routine CNS prophylaxis with at least intrathecal methotrexate. [11] But its role in prophylaxis remain controversial as CNS relapses have been observed after intrathecal therapy and CNS relapses also occur in brain parenchyma. [7],[18] Considering the rarity of disease, it will be difficult to standardize the therapeutic and preventive strategies through randomized trials; treatment will continue to evolve with improved understanding of the molecular and genetic characteristics of testicular lymphoma, identification of patients at higher risk of relapse and with incorporation of newer drugs into current regimes of chemotherapy. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09008t1.jpg] |
| |||||||||

{kind=link}