 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
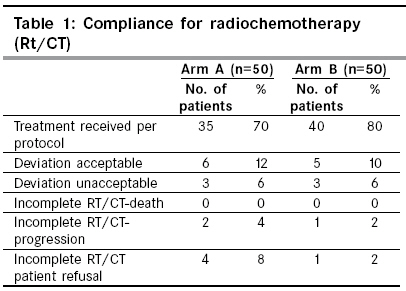
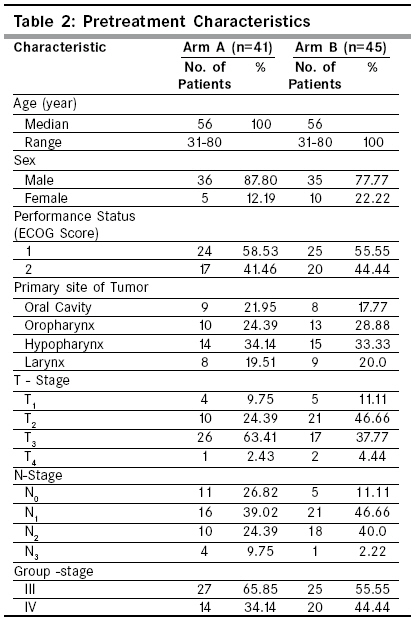
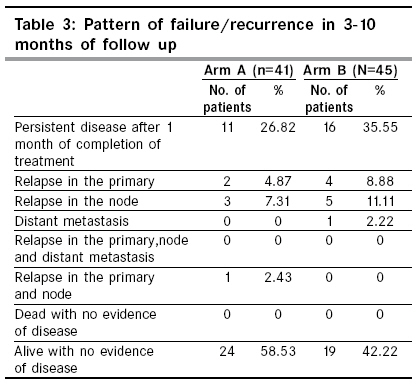
Indian Journal of Cancer, Vol. 46, No. 1, January-March, 2009, pp. 50-53 Original Article A comparative study of low dose weekly paclitaxel versus cisplatin with concurrent radiation in the treatment of locally advanced head and neck cancers Jain RK, Kirar P, Gupta G, Dubey S, Gupta SK, Goyal J Department of Radiotherapy, Jadao Ba Cancer Hospital, N.S.C.B. Medical College, Jabalpur - 482 003, Madhya Pradesh Code Number: cn09009 Abstract Purpose: The purpose of this study was to compare low dose weekly paclitaxel versus cisplatin with concurrent radiation in locally advanced head and neck cancers.Materials and Methods: From August 2005 to July 2006, a total of 100 biopsy proven, locally advanced head and neck cancers were enrolled for the study. All the patients were stratified in two groups, study group A and control group B. Study group patients received injection Paclitaxel 20 mg/m 2 , I/V 1 hr infusion weekly for 6 weeks and control group patients received injection Cisplatin 30 mg/m 2 , I/V 2 hrs infusion weekly for 6 weeks. All patients received 66-70 Gy concurrent radiation at the rate of 2 Gy/day, 5 #/week, in 6-7 weeks by cobalt theratron phoenix - 80 teletherapy units. Result: Complete response achieved in 73% of patients in study group and 64% of patients in control group. There was no statistically significant difference observed between the study group and the control group (χ2 = 1.167, df = 1, level of significance 0.05). On 3-10 months of follow-up 59% of patients in the study group and 42% of patients in the control group are alive and disease free. Local toxicities including mucositis, dysphasia and skin reactions were more in the study group but tolerable. Conclusion: Efficacy of paclitaxel in low dose weekly schedule is comparable to cisplatin in locally advanced head and neck squamous cell carcinoma. Further analysis and follow-up are needed to evaluate if this benefit will translate into prolonged survival. Keywords: Concurrent radiation, locally advanced head and neck cancer, paclitaxel Introduction The incidence of malignancy of head and neck is exceptionally high in India as compared to western and other developed countries. This is attributed to certain habits and risk factors like oral intake of tobacco, betel nut chewing, pan masala and poor oral hygiene. The lack of awareness and education among the population results in presentation in advanced stages. In the past, treatment for patients with advanced disease has involved surgery plus radiation therapy for resectable tumors or radiation therapy alone for inoperable lesions. Because of both the poor overall survival and functional outcome associated with these therapies, trials using chemotherapy in conjunction with definitive local treatment to try to improve outcome have been conducted. [1] Unavailability of surgical facilities and high expense of surgery are other factors. Also, because the critical location of most neoplasms of the head and neck interferes with breathing, eating and speaking in the last stage of illness, the cosmetic and functional implications of therapy often weigh heavily in treatment decisions. It has become increasingly clear that the use of chemotherapy concurrent with radiation contributes to improved loco regional control and prolongs survival. [2],[3],[4] We used Cisplatin arm as a control arm because cisplatin is one of the most extensively used agents effective in the management of squamous cell carcinoma of head and neck which can be used either as a single agent or combined with a variety of other drugs and has shown improved overall response rate ranging from 23 to 71%. [5] Paclitaxel, a newer active single agent in head and neck cancer was used in the trial arm, in low dose weekly schedule. [6] Observation suggests that paclitaxel induces a cell cycle blockade at the G2 phase to mitosis (G2/M) transition, the most radiosensitive portion of the cell cycle, leading to studies demonstrating a radiation sensitizing effect of paclitaxel in head and neck squamous cell carcinoma (HNSCC). [7],[8],[9] An additional mechanism seems to involve enhanced tissue oxygenation induced by paclitaxel. [10] Keeping this in mind in our setting we planned to compare the role of concomitant chemoradiation using paclitaxel versus cisplatin in locally advanced head and neck cancers. Materials and Methods Patients with biopsy proven HNSCC stages III and IV tumors for all sites were eligible. Patients must have been either ineligible for curative resection or have refused surgery and must have had no prior radiotherapy to the head and neck region or chemotherapy. Patients with obvious metastatic disease on diagnostic imaging were excluded from the study. Additional eligibility criteria included the following: eastern co-operative oncology group (ECOG) performance status < 2, age greater than 18 years, absolute granulocyte count greater than 2000/mm 3 , platelet count greater than 100,000/mm 3 , serum bilirubin, SGOT, SGPT, serum creatinine within normal limit, no other history of active malignancy and no other serious medical disease. Pretreatment evaluation included medical history, physical examination and complete blood work. Additional tests and studies required included chest X-ray, X-ray mandible, USG neck/abdomen, electrocardiogram and a dental evaluation. Patients who fulfilled the above eligibility criteria were made aware of the purpose and the design of the study and required to sign the informed consent. All patients were treated on a cobalt theratron phoenix-80 teletherapy unit. Patients of both arms received a total dose of 66-70 Gy radiation, 200 cGy/day, 5#/Week in 6-7 weeks. Arm A patients received concurrent dose of paclitaxel 20 mg/m 2 I/V 1 hour infusion with codon drip set 4 - 6 hours before radiation, repeated weekly for 6 cycles. Arm B patients received concurrent dose of cisplatin 30 mg/m 2 I/V 1 hour infusion with full hydration 4-6 hours before radiation, repeated weekly for 6 cycles. During the study, patients were hospitalized and given symptomatic treatment as needed. Patients were reviewed every week and assessed with complete clinical examination including indirect laryngoscopy and in addition, were evaluated for toxicities according to RTOG acute radiation morbidity scoring criteria. Systemic toxicities were graded according to the common toxicity criteria, version 2. Laboratory and clinical toxicities were considered acute if discovered during the first 12 weeks after the initiation of therapy. Results Between August 2005 and July 2006, 100 patients were entered into the study. Of these 41 patients in arm A and 45 patients in arm B received complete treatment as defined per protocol or with an acceptable variation with respect to overall days of therapy and total dose [Table - 1]. A total of 86 patients in both arms remained for analysis. Pretreatment characteristics of patients and tumors are shown in [Table - 2]. Response assessment was done after 1 month of completion of treatment. Complete response rates were 73 and 64% respectively for arm A and arm B. There was no statistically significant difference observed in the groups (χ2=1.167, df = 1, level of significance 0.05 ). On follow-up of 3-10 months 59 and 42% of cases are alive and disease free in arm A and B respectively [Table - 3]. Acute grade III, IV toxicity were reported more in arm A in comparison to arm B [Table - 4]. Discussion This study was intended to compare concomitant chemoradiation using newer active agent paclitaxel in low dose weekly schedule versus most extensively used agent cisplatin with conventional radiation in locally advanced head and neck cancers. In this study, we have shown that a low dose weekly infusion of paclitaxel as an outpatient during standard radiation therapy is a promising and well-tolerated regimen. A 73% complete response was achieved with paclitaxel versus 64% with cisplatin in patients with highly advanced HNSCC. Although some patients in our study in the paclitaxel arm sustained high local toxicity mucositis with dysphagia, this was acceptable and comparable to the use of concurrent cisplatin. No dose limiting systemic toxicity was encountered in our study. The 73% of complete response achieved in our study in the paclitaxel arm is comparable to those achieved with the regimens employed by Hoffmann et al . and by Steinbesy et al . [11],[12] The rationale for using low dose weekly paclitaxel is based on preclinical and clinical data that suggest the direct antitumor activity and radiosensitisation effect are more dependent on the duration of paclitaxel exposure than on the peak serum concentration. [13],[14],[15] A study has proved that the radiation potentiating activities of taxenes on normal tissue are less pronounced than those on tumors. [16] A study by John et al . found local toxicities to be greater with the higher paclitaxel dose and no significant improvement in local control with high doses. [17] Hoffman et al. studied the combination of conventional radiotherapy with weekly 1 hour infusion of paclitaxel in 18 patients with unresectable HNSCC. [11] Paclitaxel was given at a starting dose of 20 mg/m 2 , and subsequent dose escalations of 10 mg/m 2 were applied. Radiation therapy was administered over 6 to 7 weeks with 200 cGy daily, up to total doses of 60-70 Gy. The maximum tolerated dose of paclitaxel in this setting was 30 mg/m 2 /week, with mucositis being dose limiting. [11] Lovey et al . examined the use of low-dose paclitaxel concurrently with radiation for patients with locally advanced head and neck cancers. [18] Twenty-six patients were treated with external beam radiotherapy and received concomitantly 2 mg/m 2 paclitaxel three times a week. Beside an acceptable efficacy (RR: 65%, 2-year overall survival 46%) the treatment was well tolerated and resulted in a favorable toxicity profile. This regimen is resource effective and allows successive therapy if necessary, and therefore may serve as an alternative for patients in poor condition with locally advanced head and neck cancers. [18] Serious toxicity was observed in a small study of 14 head and neck cancer patients who were treated with paclitaxel every three weeks in a dose of 100 mg/m 2 concurrently with external beam radiation. [19] Most patients needed a percutaneous gastrostomy. Twelve of 13 evaluable patients achieved a complete response at the primary site with this approach. Another phase I trial studied the simultaneous treatment of continuous 24 hr paclitaxel (75 mg/m 2 /d) concomitant with radiotherapy in 24 patients with advanced head and neck cancer. [12] The dose-limiting toxicities in this study were febrile neutropenia and stomatitis. All patients had major response. [12] Because of the shorter duration of follow-up, we cannot draw any inferences about disease free survival and overall survival. In addition, this study had a small sample size and was not randomized. Therefore, further studies are needed with large sample sizes and long duration of follow-up. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09009t4.jpg] [cn09009t3.jpg] [cn09009t1.jpg] [cn09009t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}