 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
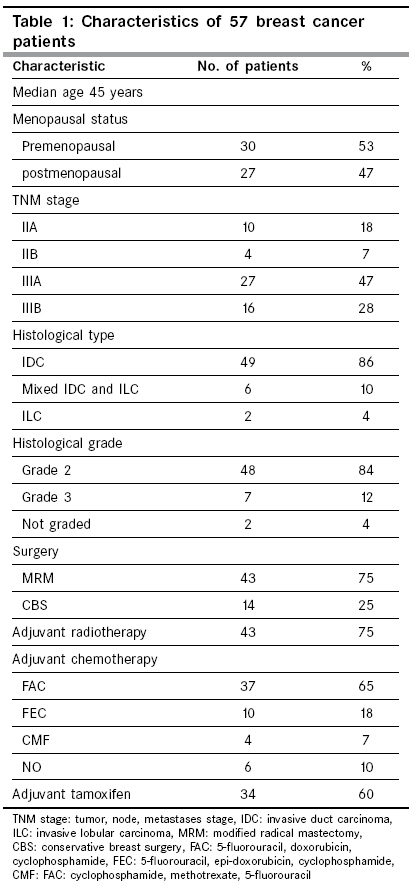
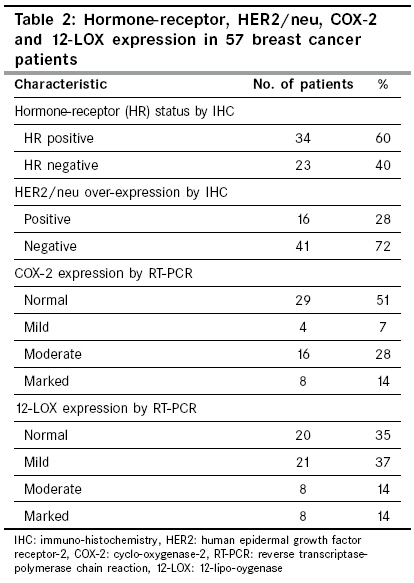
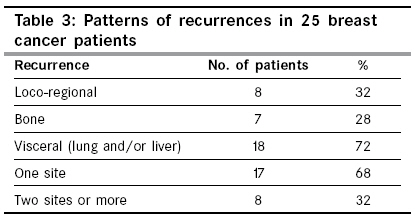
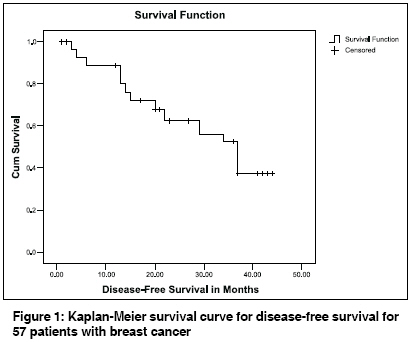
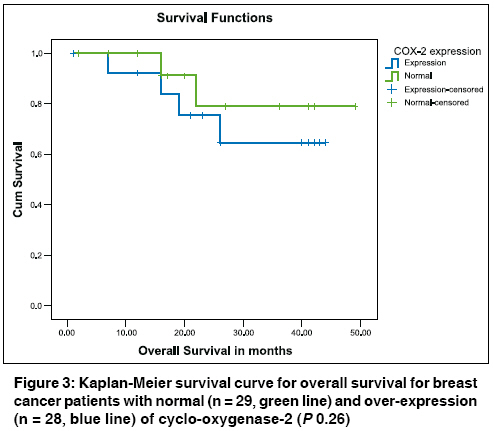
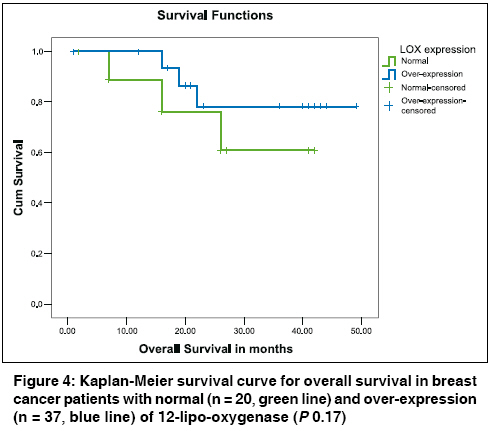
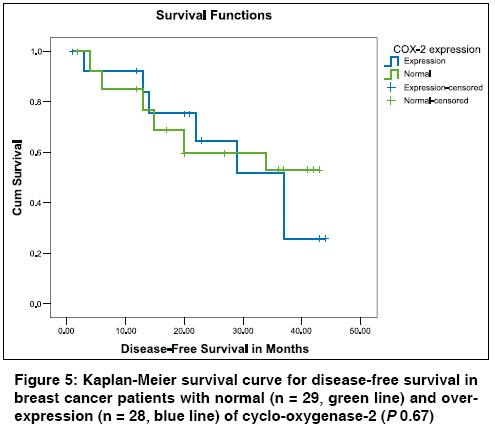
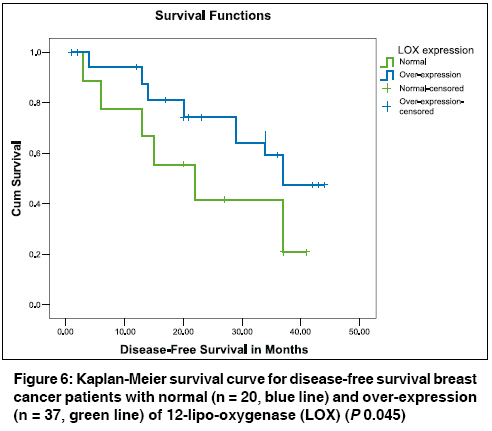
Indian Journal of Cancer, Vol. 46, No. 1, January-March, 2009, pp. 54-60 Original Article Survival effects of cyclooxygenase-2 and 12-lipooxygenase in Egyptian women with operable breast cancer Zeeneldin AA, Mohamed AM, Abdel HA, Taha FM, Goda IA, AboDeef WT Department of Medical Oncology, Faculty of Medicine, NCI, Cairo Univ Code Number: cn09010 Abstract Background: Breast cancer (BC) is the commonest among women in Egypt as well as in many other countries. Cyclo-oxygenase-2 (COX-2) and 12-lipo-oxygenase (12-LOX) are over-expressed in 30-40% of patients and carry a poor prognosis. The objectives of this study were to correlate COX-2 and 12-LOX expression with various clinico-pathologic patients' characteristics and their impact on overall survival (OS) and disease free survival (DFS) in Egyptian women with operable BC.Materials and Methods: This prospective study included 57 consecutive BC cases presenting to the Egyptian National Cancer Institute. Sections from BC and nearby normal tissues were examined for expression of COX-2 and 12-LOX using reverse transcriptase polymerase chain reaction. Results: The patients' median age was 45 years. Fifty-three percent were premenopausal. Stage II and III disease represented 25 and 75% respectively. Adjuvant chemotherapy, radiotherapy and tamoxifen were used in 90, 75 and 60% respectively. Sixty percent had hormone-receptor positive tumors and 28% over-expressed HER2/neu. Forty-nine and sixty-five percent showed over-expression of COX-2 and 12-LOX respectively. Patients with higher TNM stage or who developed visceral metastases had significantly higher COX-2 expression. For the whole group of patients, the median DFS was 37 months, while the median OS was not reached. OS or DFS did not differ significantly between patients with normal and over-expression of COX-2. DFS but not OS was significantly higher in 12-LOX over-expression compared to normal expression. Conclusion: COX-2 over-expression was associated with poor prognostic criteria in BC, but did not affect DFS or OS. 12-LOX over-expression was associated with better DFS, but not OS. Keywords: Breast cancer, cyclo-oxygenase, Egypt, lipo-oxygenase, survival Introduction Breast cancer (BC) is the most common type of cancer and the most common cause of cancer-related mortality among women worldwide. [1] In Egypt, BC is the first in females representing 37% of all female cancers presenting to National Cancer Institute, Cairo University. [2] Following surgery for operable BC, many prognostic factors help in the choice of systemic therapy including axillary lymph node status, size of the primary tumor and its grade and also the patient′s age. As predictors for response to systemic therapy, hormone receptor positivity and HER2/neu over-expression are predictors of response to hormonal manipulations and trastuzumab respectively. Efforts are continuous seeking novel prognostic and predictive factors in BC. [3] Cyclo-oxygenase-2 (COX-2) and 12-lipo-oxygenase (12-LOX) potentially serve as prognostic and predictive factors. Many investigators reported poor disease free survival (DFS) and overall survival (OS) with over-expression of COX-2. [4],[5],[6],[7],[8],[9] Significance of 12-LOX in BC is not yet well established and is less reported than COX-2. Connolly et al. reported rapid growth and high angiogenic activity in 12-LOX gene-transfected MCF-7 human breast cancer cells in athymic nude mice. [10] COX and LOX enzymes act on arachidonic acid as a substrate to form various eicosanoids. COX is a key enzyme responsible for the biosynthesis of endoperoxides that are converted into prostaglandins (PGs) and thromboxanes (TXs). LOX provides hydroperoxyeicosatetraenoic acid (HPETE) that can be converted into leukotrienes, hepoxilins, trioxilins and lipoxins. Inhibition of COX directs arachidonic acid to LOX pathway. [11] COX-2, 5-LOX and 12-LOX are expressed and up-regulated in a quite large number of cancer cells and human tumors, including lung, colon, prostate, breast, and mesothelioma. [12],[13],[14] COX exists in two isoforms commonly referred to as COX-1 and COX-2. They are the products of two distinct genes localized to chromosomes 9 and 1, respectively. [15],[16] Both enzymes carry out essentially the same catalytic reaction and have similar primary protein structures. [17] Normally, COX-1 is constitutively expressed in a broad range of cells and tissues. [18],[19] In contrast, COX-2 is an immediate early response gene and its expression is normally absent in most cells and tissues but it is highly induced in response to pro-inflammatory cytokines, hormones, and tumor promoters. [20] COX-2 expression contributes significantly to the tumorigenic potential of epithelial cells by increasing adhesion to extracellular matrix and making them resistant to apoptosis. [21] Over-expression of COX-2 in cancer cells induces the production of angiogenic factors such as vascular endothelial growth factor and basic fibroblast growth factor. [22] COX-2 derived PGE2 is a pro-inflammatory bioactive lipid and is the major prostaglandin produced in many human solid tumors, including cancer of the colon, stomach, and breast. [23],[24],[25] By binding to its cytoplasmic or nuclear receptors, PGE2 promotes angiogenesis, effects changes in cellular migration and invasive potential, alters cell cycle progression, reduces apoptosis, and inhibits immune surveillance; each of these factors contributes to the malignant phenotype. [26] PGE2 was also reported to trans-activate epidermal growth factor receptor. [27] Three forms of 12-lipoxygenase (12-LOX) have been identified, "leukocyte-type" and "platelet-type" [12(S) LOXs], and a "skin-type" [12(R) LOX]. These differ in tissue localization, substrate specificities, immunogenicities and sequence homology. The leukocyte-type 12-LOX has also been found in other tissues, including the rat pineal gland and human adrenal gland. The platelet-type 12-LOX has thus far been found only in platelets and human epidermal cells. Therapeutic agents that either activate or inhibit 12-lipo-oxygenase may be useful in treatment of atherosclerosis, hypertensive disorders, diabetes, and metastatic diseases. Both isoforms of 12-LOX have recently been cloned. [28] 12-LOX directs arachidonate metabolism towards the formation of Lipoxin A4 (LXA4). LXA4 is reported to have anti-inflammatory properties, inhibit leukocyte adhesion by affecting L-selectin and CD11/18 [29] and enhance necrosis. [30] On cancer cells, actions of 12-LOX are similar to 5-LOX and COX-2, since it stimulates proliferation and may be pro-angiogenic. [14] It enhances angiogenesis and growth of MCF-7 human breast cancer cells in athymic nude mice. [10] The aim of this study was to detect the incidence and significance of COX-2 and 12-LOX in operable BC through their effects on OS and DFS and also their correlations with various prognostic factors. To the best of our knowledge, this is the first report about the incidence and prognostic significance of COX-2 and 12-LOX in BC patients from Egypt. Materials and Methods This prospective study included a total of 57 females with operable BC consecutively presented to the National Cancer Institute, Cairo University, Egypt (NCI-Egypt). NCI-Egypt is the largest cancer hospital in the Middle East. It includes 550 beds serving all cancer-related specialties. Recruitment of cases was between December 2000 and February 2003. They were followed until May 2006. The study was approved by the local Institutional Review Board and all the patients consented to participate in the study. Inclusion criteria were histologically confirmed BC, female sex, age 18 years or more, operable BC, performance status (World Health Organization) 0-2, adequate organ functions, adequate hematologic parameters (absolute neutrophil count> 1.5 x 10 9 /l and platelets> 100 x 10 9 /l); creatinine level < 1.5 x upper limit of normal (ULN) and total rise in bilirubin level < 1.25 x ULN; aspartate and alanine aminotransferases < 3.0 x ULN; and consent to participate in the study. Exclusion criteria were male sex, pregnant females, metastatic or inoperable BC, second primary tumor and severe cardiac dysfunction. Pretreatment evaluation consisted of detailed medical history and physical examination, routine blood tests, chest X-ray and abdomino-pelvic ultrasound. CT scans of the chest/abdomen/pelvis or isotopic bone scan were done as dictated by the stage of the disease. All treatment strategies employed were according to the institutional practice guidelines. Tissues were obtained at first surgery. The major part is formalin-fixed and then paraffin-embedded and assessed according to the standard pathologic techniques. Estrogen receptor (ER) and progesterone receptor (PR) statuses were assessed by immunohistochemistry (IHC). Cases were considered positive for ER or PR when they showed a nuclear staining in more than 5% of tumor cells. Human epidermal growth factor receptor-2 (HER2/neu) status was assessed by IHC. The HercepTest ® scoring system was applied; negative = no membrane staining or < 10% of cells stained; 1+ = incomplete membrane staining in> 10% of the cells; 2+ => 10% of the cells with weak to moderate complete staining; and 3+ = strong and complete membrane staining in> 10% of the cells. Fluorescent in situ hybridization (FISH) technique was not used to verify HER2/neu with a score of 2+. Parts of the BC tissues and their corresponding matched adjacent normal tissues were frozen in liquid nitrogen at -80°C. Total RNA from tissues was extracted and stored at -70°C until assaying by reverse transcriptase-polymerase chain reaction (RT-PCR). PCR products were separated on a 2% agarose gel and the intensity of bands was measured. COX-2 or 12-LOX was defined positive when their percent of intensity was greater by 5% than the control. [31] Statistical analysis The study end points were disease free survival (DFS) and overall survival (OS). Statistical analysis was performed using statistical package for social sciences (SPSS) software for PC (version 13). Chi-square test was used to determine whether there was a statistically significant difference in the expression of COX-2 and 12-LOX between the cancer specimen and the corresponding adjacent normal specimen. Also, Chi square test was used to analyze the statistical correlation between the over-expression of COX-2 and 12-LOX with various clinico-pathological factors. P value less than 0.05 was considered statistically significant. DFS and OS were both determined by the Kaplan-Meier product-limit method, [32] and the confidence intervals (CIs) were calculated using methods for exact binomial CIs. [33] Results The median age of the 57 women with operable BC included in this study was 45 years (ranged between 27-74 years). [Table - 1] shows a summary of the patients′ characteristics. Fifty-three percent of the patients were premenopausal and 75% had stage III disease. Only 25% of patients had conservative breast surgery (CBS). The rest of the patients had modified radical mastectomy (MRM). The mean tumor size was 6 cm. The mean number of positive axillary lymph nodes was 7. Adjuvant anthracycline-based chemotherapy, hormonal therapy (tamoxifen) and radiotherapy were used in 83, 60 and 75% respectively. Using IHC technique, 60% patients had hormone receptor positive tumors defined by positivity for ER and/or PR, while only 28% over-expressed HER2/neu (3+). Using RT-PCR, 49% and 65% patients had over-expression of COX-2 and 12-LOX as compared to their corresponding normal adjacent tissues respectively [Table - 2]. By the end of the study, 25 patients (44%) had loco-regional or distant disease recurrence. Seventeen patients had only one site of recurrence [Table - 3]. Patients who developed visceral metastases (lung and/or liver) were more likely to have COX-2 over-expression at the time of initial diagnosis compared to the rest of the patients ( P 0.028). Patients who developed visceral metastases did not have 12-LOX over-expression at the time of initial diagnosis compared to the rest of the patients ( P 0.07). COX-2 and 12-LOX expression did not vary in relation to the number of metastatic sites. COX-2 and 12-LOX expressions were correlated with age (up to 35 years or more), menopausal status, hormone receptor (HR) status, tumor grade, tumor stage, lymph node stage and TNM stage. COX-2 over-expression was more likely with higher tumor stage ( P 0.041), nodal stage ( P 0.005) and TNM stage (p 0.003). While insignificant, COX-2 over-expression was more likely with HR-negative ( P 0.15) and in HER2/neu over-expressing tumors ( P 0.2). Over-expression of 12-LOX was not significantly correlated with any item. Expressions of COX-2 and 12-LOX were not correlated with each other. After a median follow-up period of 36 months [95% confidence interval (CI): 22-50 months], 12 patients died of disease recurrence and an additional 13 patients were alive with evidence of disease recurrence. The median disease-free survival (DFS) was 37 months (95% CI: 30-44 months) [Figure - 1]. The median overall survival (OS) was not reached and the mean OS was 40 months (95% CI: 36-45 months) [Figure - 2]. Although OS did not differ significantly between patients with normal and over-expression of COX-2, OS was better in patients with tumors normally expressing COX-2 ( P 0.26). The median OS was not reached in both groups. The mean OS was 43 and 35 months in normal and over-expressors of COX-2 respectively (CI: 37-48 and 29-40 months respectively) [Figure - 3]. Similarly, OS did not differ significantly between patients with normal and over-expression of 12-LOX ( P 0.17). In contrast to COX-2, OS was better in patients with tumors over-expressing 12-LOX. The median OS was not reached in both groups. The mean OS was 32 and 42 months in normal and over-expressors of 12-LOX respectively (CI: 26-39 and 38-47 months respectively) [Figure - 4]. DFS did not differ significantly between patients with normal and over-expression of COX-2 ( P 0.67). The median DFS was not reached in patients with normal COX-2 expression and it was 37 months in patients with COX-2 over-expression (CI: 29-45 months) [Figure - 5]. DFS was significantly higher in patients with over-expression of 12-LOX compared to those with normal 12-LOX expression (P 0.045). The median DFS was 37 months in 12-LOX over-expressors (CI could not be calculated), while it was 22 months in 12-LOX normal-expressors (CI: 10-34 months) [Figure - 6]. Discussion COX-2 is an immediate early response gene and its expression is normally absent in most cells and tissues but it is highly induced in response to pro-inflammatory cytokines, hormones, and tumor promoters. [20] It is expressed in many tumors including colon, stomach, breast. [23],[24],[25] There is a growing body of evidence that COX-2 expression is a fundamental step in breast cancer pathogenesis acting through prostaglandin-dependent and independent mechanisms. [34] Several studies have suggested that COX-2 expression is associated with parameters of aggressive breast cancer, including large tumor size, positive axillary lymph node metastases, ER negative and HER2-positive tumor status. [35] Similar to other studies, [4],[5],[6],[7],[36],[37],[38] we reported that 49% of the 57 patients with operable BC over-expressed COX-2. However, other authors reported very high COX-2 expression up to 80% or more. [39],[40],[41],[42],[43] The reason for this variation is unknown and may be related to racial variation or different methodologies (IHC, RT-PCR or Microarray). Similar to our study, other investigators have found a significant correlation between COX-2 over-expression and larger tumor size, higher nodal stage and higher TNM stage. [6],[7],[38] However, these significant correlations were not shown in the studies reporting very high rate of COX-2 over-expression exceeding 80%, [40],[42],[43] so that almost all the patients, whether of low or high stage, had COX-2 over-expression. Similar to other investigators, [7],[8],[36],[37],[42] we failed to show significant correlations between COX-2 over-expression and ER negativity, Her2/neu over-expression, higher tumor grade or patients′ age. Contrary to our study, Wulfing et al. and Ristimaki et al. reported a significant correlation between COX-2 over-expression and ER negativity, Her2/neu over-expression and higher tumor grade. [6],[7] Smaller patients′ number, absence of grade 1 and few grade 3 tumors in addition to lack of FISH confirmation of immuno-histochemnistry Hercep Test (R) score of 2+, in our study, may explain the controversy. Similar to our study, other investigators [6],[39],[44] have found that DFS and OS did not differ significantly between patients with low and those with high COX-2 expression. On the contrary, poor DFS and OS in patients with COX-2 over-expression were reported by other authors. [4],[5],[9] The relatively smaller number of patients in our study might be a reason for the difference not reaching a statistical significance. Over-expression of 12-LOX was not significantly correlated with age, menopausal status, HR status, tumor size, tumor grade, lymph node stage and TNM stage. OS tended to be higher in patients with over-expression of 12-LOX compared to those with normal expression (p 0.17). DFS was significantly better in patients with over-expression of 12-LOX compared to those with normal 12-LOX expression ( P 0.045). Our results contradict Connolly et al . whose work was on nude mice. [10] 12-LOX directs arachidonate metabolism towards the formation of Lipoxin A4 that have anti-inflammatory properties, inhibits leukocyte adhesion and enhances necrosis. [29],[30] All these actions might confer good prognosis in BC. In conclusion, in our study, COX-2 over-expression was associated with poor prognostic features in operable BC namely, larger tumor size, higher nodal stage and higher TNM stage. OS and DFS appear to be worse with COX-2 over-expression. 12-LOX over-expression was not associated with any prognostic feature in operable BC. It was associated with higher DFS and OS. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09010f2.jpg] [cn09010t3.jpg] [cn09010f5.jpg] [cn09010f6.jpg] [cn09010f4.jpg] [cn09010t1.jpg] [cn09010f3.jpg] [cn09010f1.jpg] [cn09010t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}