 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
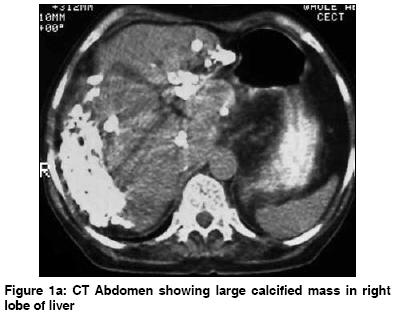
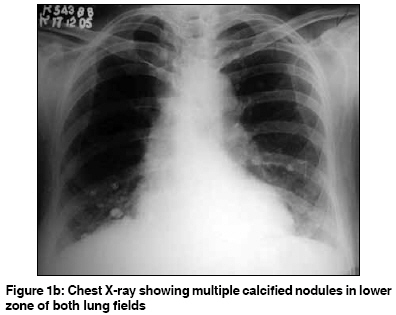
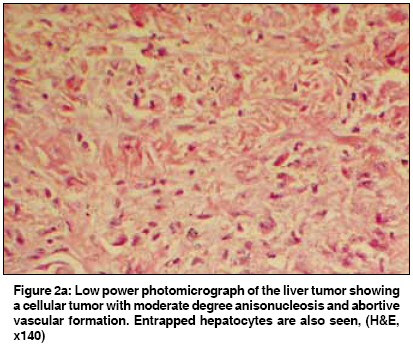
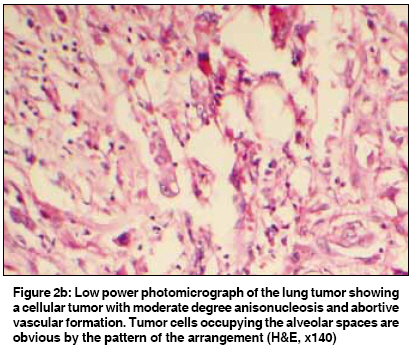
Indian Journal of Cancer, Vol. 46, No. 1, January-March, 2009, pp. 61-63 Case Report Coexistent hepatic and pulmonary epitheloid hemangioendothelioma Kalra N, Kochhar R, Vaiphei K, Virmani V, Yadav TD, Khandelwal N Department of Radiodiagnosis, PGIMER, Chandigarh Code Number: cn09011 Abstract Epitheloid hemangioendothelioma (EHE) is a rare neoplasm of vascular origin known to arise in soft tissue, liver and lung. We describe a case of coexistent hepatic and pulmonary epitheloid hemangioendothelioma, proven on autopsy, and review the histological and radiological features of epitheloid hemangioendothelioma. The coexistence of hepatic with pulmonary EHE has been reported in only a few cases. Large confluent masses, peripheral location with capsular retraction, hypertrophy of uninvolved liver, invasion of portal and hepatic veins, enhancing margins and delayed enhancement and dense calcification are the typical features which provide a clue to diagnosis of hepatic EHE. In patients with both hepatic and pulmonary EHE it is difficult to say whether the tumor arose primarily in the lung or liver, or began simultaneously in both organs.Keywords: Hemangioendothelioma, hepatic, pulmonary Introduction Epitheloid hemangioendothelioma (EHE) is a rare neoplasm of vascular origin known to arise in soft tissues, liver and lung. This term was coined in 1982 by Weiss and Enzinger who reported 41 patients with an unusual soft tissue tumor of vascular origin. [1] In 1975 a pathologically similar tumor was reported in the lung in 20 patients by Dail and Leibow who named it as intravascular bronchioloalveolar tumor. [2] The coexistence of hepatic with pulmonary EHE [3] has been reported in only a few cases. However in patients with both hepatic and pulmonary EHE it is difficult to say whether the tumor arose primarily in the lung or liver, or began simultaneously in both organs. EHE has non-specific clinical manifestations and many cases are misdiagnosed at presentation. Familiarity with imaging findings may allow detection of disease at an earlier stage. We report a case of hepatic EHE with pulmonary EHE, which was proven on autopsy.Case Report A 70-year-old female presented with a three-month history of right upper quadrant pain and one-month history of jaundice and abdominal distention with loss of appetite and loss of weight. There was no history of fever. Physical examination revealed hepatomegaly with ascites. Contrast enhanced CT of the abdomen showed hepatomegaly with an irregular contour, with a peripheral calcified mass primarily in the right lobe of the liver with non-visualized intrahepatic portal venous branches [Figure 1a]. MRI of the abdomen showed that the mass lesion was hypointense on T1WI and heterogeneously hyperintense on T2WI. Chest X-ray showed multiple 1-2.5 cm calcified lesions in both lung fields [Figure 1b]. During her stay in hospital, the patient developed hypotension with hepatic and respiratory failure and eventually had a cardiac arrest. Autopsy findings revealed 4000 ml of straw colored fluid in peritoneal cavity. The liver surface was grossly distorted with scarred depressed areas with a thick capsule. Randomly distributed calcified areas were seen in the right lobe of liver. The main portal vein was dilated. On microscopy a fibrotic tumor with variable sized vascular channels was seen. Tumor cells had a tendency to form vascular lumen. High-grade mitotic figures could be identified in the tumor cells [Figure 2a]. Tumor clusters were present within smaller branches of portal and central veins with sinusoidal extension. Tumor cells showed positivity for CD31, CD34 and vimentin. Electron microscopy showed many Weibel Palade bodies further confirming the endothelial origin of the tumor cells. The lungs showed multiple tumor emboli in the pulmonary vessels and hilar nodes with tumor cells showing high-grade mitotic figures identified in hyalinised and calcified nodular areas of the parenchyma [Figure 2b]. A final autopsy diagnosis of epitheloid hemangioendothelioma of liver and lungs was made.Discussion EHE of liver is an intermediate to low grade malignant vascular neoplasm presenting in age group 18-86 years (average age 45 years). It has a predilection for women (2:1 to 1:1 in various series). [4],[5] The clinical manifestations are variable and the presenting complaints in decreasing order of frequency are right upper quadrant pain, weight loss, easy fatigability, fever and jaundice. [4] The most common laboratory abnormality is elevated serum alkaline phosphatase levels while serum AFP is normal in all patients. [4] The prognosis is variable. It has been found to be intermediate between the benign hemangioma and the highly malignant angiosarcoma and is considered better than other hepatic malignancies. Pathologically on liver biopsy specimens, the tumor is composed of dendritic or epitheloid cells with intracytoplasmic vacuoles, occasionally containing RBCs. The stroma is fibrous with myxohyalinised areas and occasionally contains calcifications. On immunochemistry, the tumor is positive for at least one endothelial marker (Factor V111 related antigen, CD34/CD31) and negative for epithelial markers (CEA and cytokeratin). The tumor typically grows within branches of hepatic and portal veins and occludes them. This leads to portal hypertension. This tumor can be mistaken on histology for veno-occlusive disease, primary/metastatic sclerosing carcinoma or cholangiocarcinoma. There is no clear standard for treatment, because of the rarity and natural history of the tumor. Radical hepatic resection of isolated lesions is considered the treatment of choice; but the multifocal nature of the disease makes orthotopic liver transplantation the optimal treatment in most cases and it can be performed even in the presence of metastatic disease. [6] Other treatment modalities like chemotherapy with different agents like adriamycin and interferon, radiotherapy and transcatheter arterial embolisation have been tried in a few cases with varying results. The 5-year overall survival rate of patients with EHE in the literature varies from 43 to 55%. [7] Long-term survival of patients with EHE is significantly higher compared to other hepatic malignancies. [7] Partial or more complete remission after treatment has been described even in patients with coexistent pulmonary or extrahepatic involvement as part of more widespread disease. The imaging findings when typical can help in diagnosis and in assessing the spread of disease. EHE in liver or lungs is usually multifocal. In patients with both liver and lung lesions it is impossible to determine the primary site of origin of the neoplasm. In the liver, usually multifocal and bilobar involvement is seen with typical involvement of the liver periphery extending up to the capsule. Capsular retraction is seen in as many as 25% of patients. [8] In advanced cases the nodules are large in diameter. The multifocal nodular masses may coalesce and present as a diffuse heterogeneous mass lesion. [9] The involved portion of the liver may show decreased perfusion as the portal vein branches are obliterated and this leads to shunting of blood and hypertrophy of the uninvolved segments. Focal hepatic parenchymal calcification may be seen in 15-25% of cases and may also be seen on abdominal X-ray. [8] On CT, the peripheral nodular lesions, hepatic parenchymal calcification and capsular retraction are well appreciated. In widespread disease with confluent masses, the hepatic and portal veins may not be well visualized. Post contrast administration some tumor nodules show mild enhancement during arterial phase, and may become isodense in late venous phase. Splenomegaly, ascites and other features of portal hypertension may be seen. MRI shows the tumor nodules as low signal intensity lesions on T1WI. On T2WI the lesions show heterogeneously increased signal intensity. Some lesions show a target appearance on T2WI. This is due to the inner low signal intensity zone due to hemorrhage, sclerosis or calcification while the outer zone corresponds to edematous viable tumor. On I/V contrast administration tumor nodules may show peripheral enhancement with delayed central enhancement. Though distinction between normal liver and tumor may be difficult on all sequences, ferruxomide enhanced T1WI shows the extent of tumor. [10] Pulmonary EHE is diagnosed incidentally as the patients have no symptoms or only minor symptoms. Characteristically, multiple perivascular nodules with well to ill defined margins are seen in both lungs. [11] Less typical features include ground glass opacity and interlobular septal thickening. Although partial spontaneous regression has been reported, treatment options include chemotherapy and interferons. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09011f2a.jpg] [cn09011f1a.jpg] [cn09011f2b.jpg] [cn09011f1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}