 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
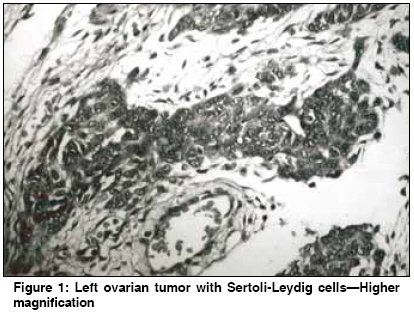
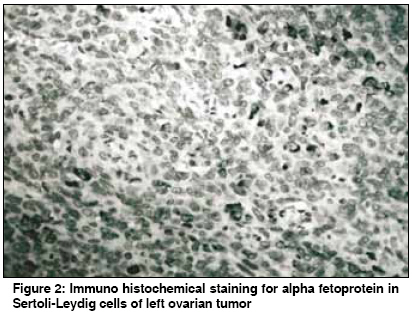
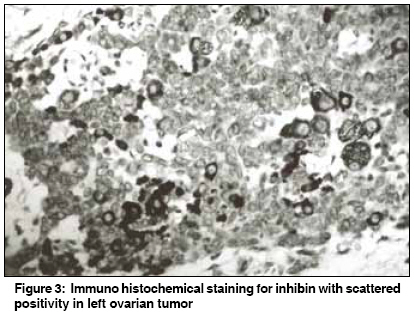
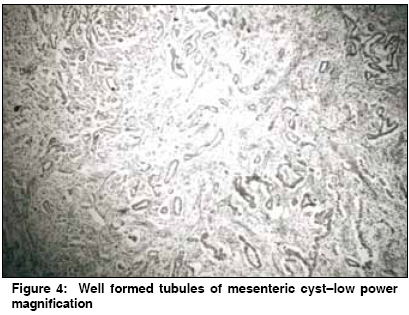
Indian Journal of Cancer, Vol. 46, No. 1, January-March, 2009, pp. 64-66 Case Report Recurrent alpha-fetoprotein secreting Sertoli-Leydig cell tumor of ovary with an unusual presentation Poli UR, Swarnalata G, Maturi R, Rao ST Department of Surgical Oncology, MNJ Institute of Oncology and Regional Cancer Centre, Hyderabad Code Number: cn09012 Abstract Alpha-fetoprotein secreting (AFP) Sertoli-Leydig cell tumors of ovary (SLCT) are now identified as a distinct entity among the uncommon group of sex cord tumors of ovary. We report an unusual case of recurrent AFP secreting ovarian tumors and as ileocecal mesenteric cyst in a 25-year-old patient resulting in difficulty in initial diagnosis of AFP producing SLCT. Although six recurrent cases were described out of the 25 reported cases of AFP secreting SLCTs, this patient with an unusual presentation of recurrence is the second case in the literature to the best of our knowledge.Keywords: Alpha-fetoprotein, ovarian tumors, Sertoli-Leydig cell tumor Introduction Sertoli-Leydig cell tumors of ovary are uncommon, accounting for 0.2% of all primary ovarian tumors. Hormone production is well described and one third of these patients have clinical and biochemical evidence of androgen excess resulting in virilization or defeminization. A small group of these SLCTs found to produce alpha-fetoprotein (AFP) were described and only 25 such cases have been reported in the literature since the early 1980s. [1] The histogenesis and clinical prognosis of these AFP producing SLCTs are not yet clearly understood. Bilateralism and recurrence in the contra lateral ovary and metastases beyond ovary or into upper abdomen is extremely rare.Case Report A 25-year-old para 1 with one living child of 7 yrs was referred with history of 4 months amenorrhea and vague abdominal pain. Hirsutism and moderate clitoromegaly were present. Abdominal examination revealed a cystic mass of 10 x 8 cm size in left fornix and normal sized uterus. Serum AFP levels were elevated (101.0U/ml) and other tumor markers were within normal range. She underwent exploratory laparotomy with total abdominal hysterectomy and left salpingo ovariotomy with infracolic omentectomy. Operative findings were a left sided ovarian cyst of 10 x 8 cm with solid and cystic areas and intact capsule, normal uterus and tubes without any intra-abdominal adhesions, deposits or free fluid. Histopathological examination of left ovarian mass showed sheets of polygonal Leydig cells with occasional glandular formations of intermediate grade [Figure - 1]. Immunohistochemical staining for alpha-fetoprotein [Figure - 2] and inhibin [Figure - 3] showed scattered cytoplasmic positivity. In the past, she was operated upon 7 yrs ago in the immediate postpartum period for an ovarian mass noticed at the time of delivery with elevated serum AFP levels (25.6U/ml). It was an uneventful pregnancy with spontaneous normal delivery. Transient mild features of hirsutism and clitoromegaly were present. She underwent right adnexectomy. The laparotomy findings at that time were a right ovarian mass of 25 x 15 cm containing solid and cystic areas with intact capsule, and there were no deposits in omentum or any intra-abdominal areas. The histopathological examination was reported as endodermal sinus tumor of right ovary. She also received 6 cycles of PEB chemotherapy regimen. Serum AFP levels returned to normal range after surgery. Two years later she was again admitted into the general surgical department on a complaint of abdominal lump and on laparotomy she was found to have a mesenteric cyst of 15 x 12 cm arising from the root of mesentery at ileocecal junction. Uterus, left ovary and other viscera were normal. There was no evidence of metastatic deposits or ascites. Tumor markers and immuno histochemistry were not done at that time. Excision of mesenteric cyst was done and histopathology was reported as adenocarcinoma of mesenteric cyst. She received 6 cycles of Cisplatin based chemotherapy and was on follow up for 3 years without any evidence of disease until the appearance of present left ovarian mass. Review of the HPE slides of mesenteric cyst revealed well-formed tubules mimicking adenocarcinoma [Figure - 4] and [Figure - 5]. HPE slides of initial right ovarian mass could not be traced for reviewing the original diagnosis. In view of the intermediate grade of the present tumor she was given combination chemotherapy with doxorubicin and Carboplatin for 4 cycles. Her serum AFP levels returned to normal and hirsutism and clitoromegaly regressed. She is disease free two years after the last treatment and 7 years after initial onset of disease. Discussion This young woman had right ovarian mass followed by mesenteric cyst in ileocecal region and left sided ovarian mass consecutively with associated features of virilization and raised serum AFP levels. This case is reported for its rarity in presentation as recurrent, AFP secreting Sertoli Leydig cell tumor of ovary with virilizing features and the histopathological misdiagnosis confusing it with endodermal sinus tumor and serous papillary adenocarcinoma. [2] Seventy-five percent of AFP producing SLCTs are usually in young patients under 30 years and only 6 cases are reported in postmenopausal women. [3] AFP is a glycoprotein, a normal product of the fetal liver, yolk sac, and fetal upper gastrointestinal tract. Elevated serum AFP is associated with hepatocellular carcinoma, germ cell tumors with endodermal sinus tumor component, carcinomas involving organs of endodermal derivations such as lung, esophagus, stomach and pancreas etc. AFP production is associated with Leydig cells, Sertoli cells and heterologous hepatocytic cells. The rise in serum AFP levels corresponds to the onset of ovarian tumor and regress to normal values immediately after surgery, as the half-life is 5 days. Immuno histochemistry studies can demonstrate AFP in tissues even in the absence of demonstrable elevation of serum AFP. [4] In our case the elevated serum AFP levels corresponded to onset of ovarian mass each time with development of virilizing signs which disappeared after surgery. Though the AFP levels were not documented with the mesenteric cyst, the histology of both the specimens is comparable suggesting recurrence of the same disease. This patient was initially misdiagnosed as endodermal sinus tumor of right ovary and later as adenocarcinoma of ileocecal mesenteric cyst. It was also emphasized by Young and Scully that presence of retiform pattern often poses difficult diagnostic problems in about 10% of SLCTs and they are confused for endodermal sinus tumor or serous cystadeno carcinomas on histological grounds. [5] The immuno histochemistry of the second recurrence with retrospective review of earlier clinicopathological correlation has led to exact diagnosis of this as AFP producing recurrent SLCT in our patient. The only earlier similar case reported was in an 11-month-old girl where metastasis occurred 4 months after primary tumor of the ovary in the mesentery, ileocecal region and iliac lymph nodes, with contra lateral normal ovary. [6] But in our patient, one ovary, ileocecal mesenteric cyst and contra lateral ovary were affected with the similar clinico pathological picture sequentially over an interval of 2 and 3 years. Most of the women who developed Sertoli Leydig cell tumors had an intermediate-differentiated tumor (58%). [7] In view of recurrence and intermediate grade of this tumor post operative chemotherapy would give a favorable outcome in our case. [8] The long-term clinical nature of the disease in this woman is difficult to predict or to prognosticate. Since the behavior and therapy of these neoplasms differs from the other epithelial and endodermal ovarian neoplasms it is important to arrive at initial correct diagnosis. The long-term prognostic factors and management protocols for these recurrent AFP producing SLCTs need to be further studied. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09012f5.jpg] [cn09012f2.jpg] [cn09012f4.jpg] [cn09012f3.jpg] [cn09012f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}