 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
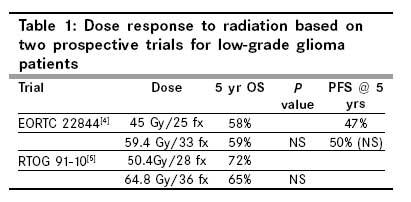
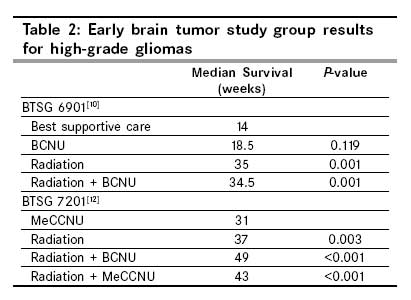
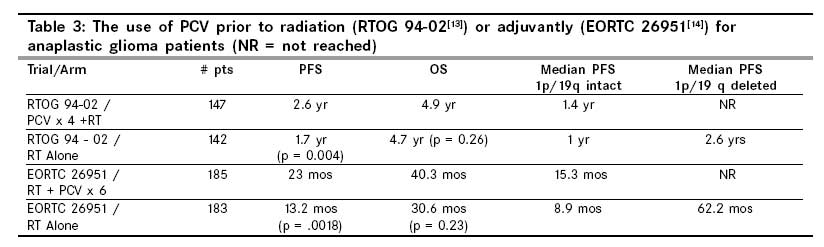
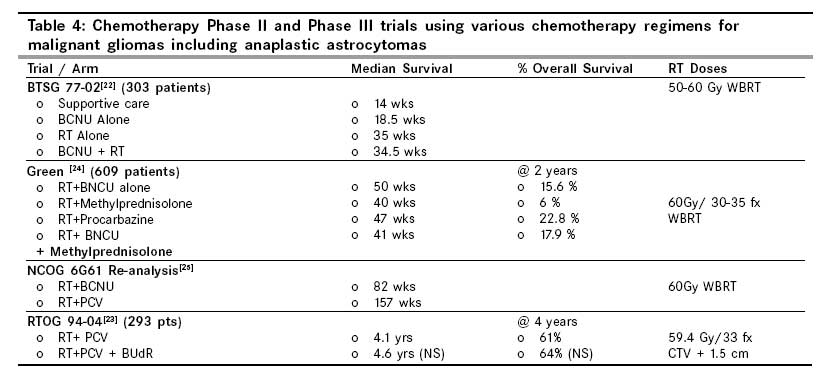
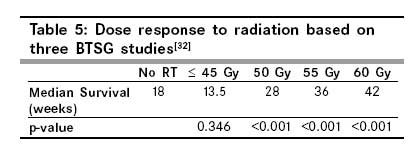
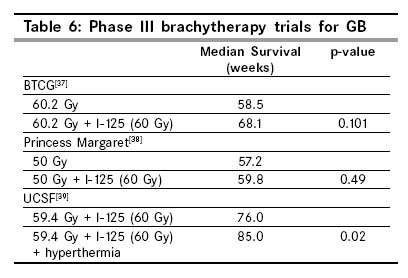
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 96-107 Symposium Evidence-based adjuvant therapy for gliomas: Current concepts and newer developments Khan MK, Hunter GK, Vogelbaum M, Suh JH, Chao ST Department of Radiation Oncology, Brain Tumor and Neuro-Oncology Center, Taussig Cancer Institute, Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, Ohio 44195 Code Number: cn09022 Abstract The incidence of gliomas is increasing worldwide, including India. Of the 18,820 new cases of primary central nervous system (CNS) tumors diagnosed annually in the United States, gliomas account for over 60% with 30-40% of them being glioblastoma multiforme (GBM), 10% being anaplastic astrocytoma (AA), and 10% being low grade gliomas (LGGs). This is in contrast to one study from West Bengal, India, in which only 7.9% of the brain tumors were GBMs, while 46.8% were astrocytomas. Of all adult primary CNS tumors, GBM is the most common and the most malignant with about 7,000 to 8,000 new cases annually in the United States. Given poor outcomes, a number of treatment approaches have been investigated. Common to these approaches is the use of adjuvant radiation therapy, even as surgery alone, with or without chemotherapy, may be the mainstay for some lower grade and low-risk gliomas. Today, treatment typically involves external beam radiation, with concurrent and adjuvant chemotherapy for more aggressive histologies. Although gliomas are relatively uncommon, active research is ongoing. Results of landmark trials along with some of the recently published trials are presented. These trials and management strategies as well as evolving concepts are found by reviewing over 200 articles in the National Library Medical (NLM) database, PubMed, more than 60 of which are refrenced. Specifically, the database is searched using the following keywords, with various combinations: glioma, low-grade, anaplastic, astrocytoma, oligodendroglioma, oligoastrocytoma, glioblastoma multiforme, chemotherapy, radiation, new concepts, phase III, MGMT, CDX-110 (Celldex), temozolomide, 1p/19q deletion, and bevacizumab.Keywords: Adjuvant therapy, anaplastic astrocytoma, anaplastic oligoastrocytoma, anaplastic oligodendroglioma, bevacizumab, CDX-110, glioblastoma multiforme, glioma, low-grade glioma, O 6 -methylguanine-DNA methyltransferase status, radiation, temozolomide, 1p/19q deletion Introduction This incidence of gliomas is in contrast to one study from West Bengal, India, in which only 7.9% of brain tumors were GBMs, while 46.8% were astrocytomas. [1] In order to review the pertinent clinical trials, the electronic database of the US National Library of Medicine and the National Institute of Health (PubMed) was reviewed, looking for literature pertaining to the adjuvant management of gliomas. Over 200 articles were reviewed, 64 of which are referenced. The focus was on evidence-based adjuvant management strategies based on historic phase III trials, as well as, describing trends based on recently reported trials and those trials that are currently underway. Furthermore, emerging concepts pertaining to the use of temozolomide - an alkylating chemotherapeutic agent, as well as, the importance of 1p/19q molecular cytogenetics, and an understanding of the O 6 -methylguanine-DNA methyltransferase (MGMT) methyl status are also highlighted in this study. While reviewing and highlighting some of the pertinent clinical trials it is important to realize that the histological classification scheme, namely the World Health Organization (WHO) classification system, used to classify gliomas, has repeatedly and substantially changed over the pertinent time period. In recognition of the emerging role of molecular diagnostic approaches to tumor classification, recent WHO updates have emphasized with greater detail, various pertinent genetic profiles. The first edition of the classification of nervous system tumors was published in 1979, and took almost a decade to complete. The second edition followed in 1993, and was a step forward, as it incorporated the advances in classification resulting from the introduction of immunohistochemistry. The third edition was published in 2000, and the most recent edition was published in 2007, with each edition based on increasingly more specific immunohistochemical and genetic markers. In light of these changes in the classification criteria, it is important to realize that the results of clinical trials cannot be fully appreciated without considering the classification system that is pertinent at that particular time. It is beyond the scope of this review to correlate previous clinical trials to the current WHO classification scheme, however, this does not detract from the applicable information gained from prior trials. Low Grade Gliomas Low grade gliomas (LGGs) typically occur in younger adults, normally before age 40, and encompass a spectrum of histological subtypes that resemble differentiated macroglial cells, without evidence of anaplasia. Diffuse astrocytomas represent 60 - 70% of the LGGs and are the most common of LGGs. The subtypes of low-grade astrocytomas include fibrillary, protoplasmic, pilocytic, and gemistocytic astrocytoma. The fibrillary subtype is the most common in adults while the gemistocytic subtype is less common, but has a higher potential for anaplastic transformation. Other histological subtypes of the LGGs include the juvenile pilocytic astrocytoma (JPA), which usually occurs before age 25, oligodendroglioma/oligoastrocytoma (LGO/LGOA), ganglioglioma, pleomorphic xanthoastrocytoma (PXA), subependymal giant cell astrocytoma (SEGA), subependymomas, and desmoplastic gangliomas. Different gliomas occur in different age groups and some entities such are PXA are more common in adolescents, while others are more common in the elderly, such as GBM. For a majority of the favorable histological LGG subtypes such as JPA, low-grade PXA, gangliogliomas, SEGA, and subependymomas, gross total resection (GTR) alone is sufficient for the asymptomatic patient. Often, adjuvant treatment is delayed until there is evidence of symptomatic or radiographic progression. For gemistocytic astrocytomas and for patients with high-risk features predictive of poor outcome, active research is underway to determine the benefits of adjuvant radiation delivered immediately versus delayed, with or without chemotherapy. Of the LGGs, the gemistocytic subtype has over a 70-80% likelihood of anaplastic transformation and is therefore generally treated aggressively, and often treated as anaplastic astrocytoma with immediate adjuvant high-dose radiation. Several retrospective reviews have questioned the role of observation and high-dose radiation for oligoastrocytoma and ordinary astrocytoma. A 1989 retrospective review of 167 patients with grade 1 - 2 supratentorial pilocytic astrocytoma, ordinary astrocytoma, or mixed oligoastrocytoma, diagnosed from 1960 - 1982, found that high-dose radiation (>53 Gy) after resection was associated with better survival compared to low-dose radiation or surgery in patients with nonpilocytic LGGs. [2] The Radiation Therapy Oncology Group (RTOG) phase II portion of the 98-02 trial published in 2005, prospectively evaluated the role of observation after GTR in 111 low risk patients younger than age of 40. This trial 98 concluded that observation is a reasonable strategy for some subsets of patients and that postoperative adjuvant treatment should be considered for higher risk patients. [3] The European Organization for Research and Treatment of Cancer (EORTC) conducted two large phase III trials, EORTC 22844 and 22845, which were published in 1996 and 2006 respectively. The EORTC 22844 trial evaluated 379 patients randomized to either 45 Gy in 25 fractions versus 59.4 Gy in 30 fractions, and concluded that there was no difference between the 59.4 Gy arm and the 45 Gy arm in terms of overall survival (OS) (59 vs. 58%) or progression free survival (PFS) (50 vs. 47%) at five years, respectively. [4] Similarly, the RTOG 91-10 trial which was published in 2002, six years later than the EORTC 22844, randomized 203 patients to 50.4 Gy in 28 fractions (101 patients) versus 64.8 Gy in 36 fractions (102 patients) and found no difference in OS or time to progression between the two arms. [5] The incidence of Grade 3 to 5 neurotoxicity, however, was 5% for the 64.8 Gy arm versus 2.5% for the 50.4 Gy arm. Results from these two trials are summarized in [Table - 1]. Thus, the benefit of higher dose for low grade gliomas is not justified, unlike that for the higher grade gliomas, such as, anaplastic astrocytomas and glioblastomas. The EORTC 22845 study included 311 patients randomized to either observation with delayed radiation only at time of progression or upfront radiation using 54 Gy to localized treatment fields. [4],[5],[6],[7] The five-year PFS rates were 55% for immediate adjuvant radiation versus 35% for delayed adjuvant radiation, for all LGG histologies. Pilocytic astrocytoma patients were not included in the study. Although the PFS was improved with immediate adjuvant radiation, the median OS times of 7.4 years for upfront radiation versus 7.2 years for delayed radiation were not statistically significant. Additionally, there were no statistical differences in the two arms with respect to headaches, cognitive deficits, and performance status at two years. However, seizures at one year were significantly more in the observation group (41%) compared to the irradiated group (25%). Furthermore, the time to progression was also reduced in the immediate radiation arm versus delayed radiation (5.3 vs. 3.4 years). These findings suggest that observation is a reasonable strategy in low-risk adults with asymptomatic supratentorial low-grade gliomas. Adults with high-risk features as described in the EORTC trials or those with symptomatic LGGs, should be managed on a case by case basis and appropriate treatment and timing of radiation should be individualized. The EORTC from the randomized studies mentioned earlier identified poor prognostic factors: age 40 years or more, astrocytoma histology subtype, tumor diameter of 6 cm or more, tumor crossing midline, and presence of neurological deficits, before surgery. [4],[5],[6],[7] The presence of fewer than three of these factors was identified as low-risk group with a median OS of 7.7 years, whereas, three or more risks were identified as a high-risk group with a median OS of 3.2 years. The use of PCV (procarbazine, Lomustine [CCNU], and vincristine) and CCNU chemotherapy is investigational for LGGs. A small Southwest Oncology Group (SWOG) study published in 1993 consisting of 60 adult patients who underwent subtotal resection were randomized to radiation alone (55 Gy in 32 fractions) or radiation with concurrent CCNU chemotherapy (100 mg/m 2 ). The radiographic response rate was 79% for radiation alone versus 54% for radiation plus CCNU. This raised questions about the merits of concurrent chemotherapy for LGGs. The median OS was 4.45 years for all patients and no significant statistical difference was noted between the two arms, at the expense of hematological toxicity with the CCNU group. [8] However, another phase II trial published in 2003, examined the use of PCV chemotherapy delivered for six cycles, eight weeks apart, followed by radiation of 50.4 Gy with a boost of either 3.6 Gy or 9 Gy, in patients with low-grade oligodendroglioma or oligoastrocytoma, showed evidence of tumor regression following PCV chemotherapy in 52% of the enrolled patients (13 of 25) at the expense of myelosupression. [9] The recently closed phase II part of the RTOG 98-02 trial was designed to evaluate the role of postoperative observation alone in favorable LGGs, and the phase III portion of this study randomized unfavorable LGG patients into the radiation alone (54 Gy in 30 fractions) arm with that of radiation followed by six cycles of PCV. Those considered unfavorable were patients of age ≥ 40 or those undergoing subtotal resection or only biopsy. Results from this trial published in 2008, showed that PFS improved for patients with LGGs, with the addition of PCV to radiation. [10],[11] This trial also suggested an OS benefit with the addition of PCV, but this was seen only in survivors beyond two years. The role of temozolomide chemotherapy is also under investigation in several phase II and phase III trials. The National Cancer Institute and EORTC are conducting a phase III trial (EORTC 22033) and the RTOG is conducting a phase II trial (RTOG 0424), both of which will help elucidate the emerging role of temozolomide in LGGs. The National Cancer Institute (NCI)/EORTC trial (EORTC 22033) is evaluating radiation alone versus temozolomide alone in a phase III trial, while the phase II RTOG trial (0424) used concurrent radiation with temozolomide, followed by adjuvant temozolomide for 12 cycles, for patients with three or more high-risk features. The high-risk features per the RTOG 0424 study include astrocytoma dominant histology, age ≥ 40, tumor that crosses midline, size ≥ 6 cm, and neurological function greater than 1. Results of these ongoing trials are awaited and will help determine the role of temozolomide with or without radiation in LGGs. Additional trials comparing PCV to temozolomide will be needed in future for LGGs. High-Grade Gliomas Anaplastic astrocytomas (AA) and glioblastoma multiforme (GBM) behave much more aggressively with poor outcome and are regarded as high-grade gliomas. Anaplastic oligodendrogliomas (AO) and anaplastic oligoastrocytomas (AOA) were thought to behave aggressively and are classified as WHO Grade 3 tumors. Recent studies have shown that depending on molecular analysis, patients with AO and AOA may have a better outcome, as described a little later in this article. The management of malignant gliomas involves maximum safe resection followed by adjuvant radiation and chemotherapy. At least three prospective randomized trials have assessed the role of adjuvant radiation with or without adjuvant chemotherapy. The Brain Tumor Study Group (BTSG) performed three protocols from 1966 to 1975. The BTSG 6901 evaluated the role of radiation with or without carmustine (BCNU) chemotherapy over best supportive care. This showed that the median OS improved from 14 weeks to approximately 35 weeks with the addition of radiation (1978). [10] Chemotherapy alone showed a slight improvement over best supportive care with a median OS of 18.5 months, but was inferior to the radiation arms. The addition of BCNU to radiation did not improve the outcome. Another study published in 1980, BTSG 7201, randomized patients to receive one of the four regimens: semustine (MeCCNU), radiation alone, BCNU plus radiation, or MeCCNU plus radiation. [12] Again, this study showed that radiation, either alone or in combination with chemotherapy, improved the chances of survival over chemotherapy alone. Based on these studies, which are summarized in [Table - 2], radiation plays an essential role in the management of high-grade gliomas.Anaplastic Oligodendroglioma/Anaplastic Oligoastrocytoma The use of adjuvant chemotherapy with PCV either before or after radiation has been evaluated in two prospective randomized control trials. The RTOG 94-02 was a prospective randomized control trial that was published in 2006, of 289 patients, which compared the role of adjuvant PCV (lomustine 130 mg/m 2 d1, procarbazine 75 mg/m 2 d8-21, and vincristine 1.4 mg/m 2 d 8-29) for four cycles followed by radiation of 59.4 Gy in 33 fx. [13] Radiation was started within six weeks of completion of chemotherapy. This trial demonstrated that PCV given prior to radiation prolonged PFS (2.6 years vs. 1.7 years), over radiation alone. The OS was not statistically significant at 4.9 years for the PCV arm versus 4.7 years for the radiation alone arm. The most notable difference in survival was for the patients with 1p/19q loss where the median OS was not reached, compared to 2.8 years for those with 1p/19q intact. [13] This was regardless of the treatment arm. The role of PCV chemotherapy after radiation was also evaluated in EORTC 26951 (2006). This prospective phase III trial of 368 patients evaluated the role of adjuvant radiation of 59.4 Gy in 33 fractions to six cycles of PCV (lomustine 110 mg/m 2 d1, procarbazine 60 mg/m 2 d8-21, and vincristine 1.4 mg/m 2 d8 - 29). Patients began radiation within six weeks of surgery, and chemotherapy was started within one month after completion of radiation. Similar findings were found within this trial as those for RTOG 94-02. Radiation followed by PCV prolonged PFS at 32 months versus 13.2 months for the radiation alone arm. However, the five-year OS was no different at 41.9% for the combined arm versus 35% for radiotherapy (RT) alone arm, but the grade III-IV toxicities were 65% in the PCV arm. Similarly, the median OS of 40.3 months for the combined arm versus 30.6 months for the radiation alone arm was not statistically significant. Patients with 1p/19q loss did significantly better than those without 1p/19q loss. The five-year overall survival for the 1p/19q loss patients was 74.7% versus 27.5% for those without 1p/19q loss. [14] The 1p/19q status is strongly prognostic and is now required in many of the newer trials. Results from these two prospective randomized control trials are summarized in [Table - 3]. Use of temozolomide has been recently studied in a phase II trial, RTOG 0131. [15] This trial evaluated the efficacy of pre-RT TMZ and the toxicity of concurrent RT and (temozolomide) TMZ in patients with newly diagnosed AO/AOA. It was noted that 6.3% of the patients had a complete response, 28.1% experienced a partial response, 50% of the patients were stable, while only 28.1% had progression. [15] Anaplastic Astrocytoma Anaplastic Astrocytomas (AA) are pathologically classified as WHO grade III tumors as they tend to behave more aggressively compared to some of the lower grade gliomas. Patients with AA have a median OS in the order of 11 months to 59 months, depending on certain prognostic factors such as age> 50, histology, mental status, Karnofsky performance status, length of symptoms prior to surgery, extent of resection, neurological functional status, and the RT dose used. Unfavorable prognostic factors predict shorter survival times based on nonparametric recursive analysis. [16] Given the aggressive and infiltrative nature of this tumor, immediate adjuvant radiation is the standard within the United States. The role of concurrent or adjuvant chemotherapy and the selection of appropriate chemotherapy are under active investigation. To date, adjuvant chemotherapy has not been validated in a prospective randomized trial for WHO III gliomas. Additional clinical trials are needed. The management of AA begins with maximal surgical resection as shown in several retrospective reviews. Adequate randomized control trials are lacking. [17] One 1989 study showed that a radical surgical resection resulting in less than 5% of tumor impacts favorably on prognosis and confers both a survival advantage and palliation of symptoms. [18] Another retrospective review published in 1992 showed that patients undergoing partial or total resection had a median survival time of 49 months versus 18 months for those undergoing biopsy only. [19] Thus, maximal surgical resection, if feasible, without major additive neurological deficit, continues to be the standard. This is then followed immediately by radiation at a minimum. Radiation has been shown to be the single most effective adjuvant treatment in two prospective randomized clinical trials conducted by the BTSG in 1978 and 1980. [20],[21] Both these trials showed improvements in median OS from four to eight months and increased the number of patients alive at 18 months from 10% to 15-20%. [20],[21] Furthermore, the role of 60.2 Gy to the whole brain as used in the earlier trials was challenged in a randomized trial published in 1989 and compared with 43 Gy to the whole brain followed by a cone-down of 17.2 Gy to the tumor volume, and it showed no difference between the two radiation techniques. [22] The standard within the United States is the use of immediate adjuvant radiation therapy after maximal safe surgical debulking. The role of chemotherapy for AA is controversial, and appropriate chemotherapy is the basis of the ongoing phase II and phase III trials within the United States. The first prospective trial to suggest the benefit of chemotherapy was reported by the BTCG in 1978. [23] This trial evaluated the role of radiation with or without BCNU in 222 patients, in a four-arm randomized control trial, with radiation doses ranging from 50 Gy to 60 Gy. The arms consisted of the best supportive group, the BCNU alone group, the radiation alone group, and the combined BCNU and radiation group. The combined group was shown to have a median OS of 34.5 weeks versus 35 weeks for the radiation alone group, at the expense of increased toxicity. [24] Thus, the use of chemotherapy has been and continues to be questioned for the management of AA. Since BCNU combined with radiation did not show efficacy, the role of other chemotherapy regimens have been tried. One 1983 phase III trial evaluated the role of procarbazine and high-dose prednisolone combined with radiation, and compared with BCNU + RT, it showed no significant difference between them and the radiation alone arm. [24] Additional trials evaluated PCV compared to BCNU. One phase III clinical trial in 1989 evaluated BCNU to PCV followed by standard radiation and showed PCV to be superior to BCNU. [25],[26] This trial showed that the median survival was 157 weeks for the PCV group versus 82.1 weeks for the BCNU group, and thus became the standard for additional trials. [25],[26] However, upon retrospective analysis of several RTOG trials including RTOG 70-18, 83-02, 90-06, and 94-04 showed that there was no statistical difference in the overall survival between PCV or BCNU. [25],[26] The benefit of adjuvant PCV against radiation alone was questioned in a Phase III randomized clinical trial done in the United Kingdom and showed no benefit in OS. [26],[27] Others have investigated the use of concurrent radiation sensitizers followed by adjuvant PCV to improve the outcome. RTOG 94-04 was a phase III randomized trial, published in 1999, comparing the adjuvant PCV with or without bromodeoxyuridine (BUdR), an analog of thymidine and a radiation sensitizer, with radiation therapy. This trial showed that there was no added OS benefit to the addition of a BUdR given concurrently with radiation. [28] Results from these phase III trials are summarized in [Table - 4]. Temozolomide has recently been shown to have some efficacy in preclinical phase I and Phase II clinical trials and serves as the basis for the RTOG 98-13 clinical trial. [26] This trial which did not meet accrual goals and closed early, randomized patients to radiation therapy (59.4 Gy in 33 fx) concurrently with BCNU or CCNU versus temozolomide. The benefits of adjuvant chemotherapy for AA were based on meta-analysis. One meta-analysis retrospectively reviewed 432 patients treated on four RTOG protocols comparing BCNU versus PCV as adjuvant chemotherapy in AA. It revealed that there was no added benefit on overall survival to PCV chemotherapy compared to BCNU, thus questioning the results of an earlier phase III clinical trial. [22],[27] A 1993 meta-analysis of 16 randomized controlled trials showed an estimated OS increase of 10% at one year and 9% at two years for patients treated with chemoradiation with the chemotherapy being BNCU in most patients. [29] Use of adjuvant chemotherapy and the selection of appropriate chemotherapy remains controversial. Additional trials with larger number of patients are needed. In light of the fact that chemotherapy has shown benefit in high-risk LGGs as well as in AOA, AO, and GBM patients, the authors feel that it is reasonable to consider the use of concurrent chemoradiation and adjuvant chemotherapy in the management of AA. The current standard of practice within the Cleveland Clinic Foundation is the use of concurrent temozolomide with radiation, followed by adjuvant temozolomide. A total dose of 5040 cGy in 28 fx is delivered to the T2 weighted post-op MRI + 2 cm margin followed by an additional 900 cGy in 5 fx delivered to the T1 weighted post-op MRI + 1 cm margin for a total dose of 5940 cGy in 33 fx. Glioblastoma Multiforme Radiation has been the mainstay of treatment for the management of malignant gliomas based on several phase III randomized control trials. Glioblastoma Multiformes (GBMs) tend to diffusely infiltrate the normal brain beyond the gross tumor and recur locally. Given its focal nature and typical failure pattern, radiation is the main modality to focus treatment on the areas of highest risk. The role of concurrent and adjuvant chemotherapy with temozolomide has been shown to improve OS. [30] An EORTC study (EORTC 22981/26981), published in 2005, concluded that the use of 75 mg/m 2 /day of temozolomide given daily, concurrently with 60 Gy/30 fx radiotherapy followed by adjuvant temozolomide 150-200 mg/m 2 /day, to glioblastoma patients improved median OS from 12.1 months to 14.6 months, with a 7% increase in grade III and IV toxicities. The two-year OS rate was 26.5% for the temozolomide group compared to 10.4% for the radiation alone group. [30] The use of temozolomide chemotherapy remains the standard within the United States, for the management of glioblastoma patients. The RTOG 0525 trial, which has recently been completed, randomized patients into an adjuvant dose-dense temozolomide group (100 mg/m 2 /day days 1-21), which was compared against the standard group (150-200 mg/m 2 /day days 1-5). Both received temozolomide for up to 12 cycles following the administration of concurrent chemoradiation as per the Stupp EORTC 22981/26981 trial. This trial is designed to evaluate the role of dose escalation with temozolomide as well as to determine if any benefits can be realized by giving temozolomide for a longer duration of 12 cycles as opposed to six cycles used in the Stupp trial. In addition to the use of novel alkylating agents such as temozolomide, an understanding of radiation and temozolomide at the biomolecular and genetic levels allows for selection of patients that are most likely to benefit with such therapy. One 2005 trial demonstrated that knowledge of the O 6 -methylguanine-DNA methyltransferase (MGMT) methyl status impacted the overall survival and progression-free survival in patients receiving concurrent temozolomide and radiation as well as in patients receiving radiation alone. [31] This trial showed that patients with methylated (silenced) MGMT promoter sequences had a median survival of 21.7 months versus 15.3 months for those who were not MGMT silenced, in the radiotherapy alone group. [31] Newer trials such as RTOG 0525, recently closed into the accrual mandate knowledge of MGMT status, as part of their eligibility criteria. Radiation Dose for Glioblastoma Multiformes The dose was retrospectively reviewed in 1979 by Walker et al . [32] This study reviewed 621 patients enrolled into three BTSG studies from 1966 to 1975, and assessed median survival stratified by dose. Patients who did not receive radiation had a median OS of 18 weeks, whereas, patients receiving 60 Gy of radiation survived a median of 42 weeks (p < 0.001). [Table - 5] shows the effect of dose on survival. Based on [Table - 5], 60 Gy is considered the current standard radiation dose used in the management of most GBM patients. Doses beyond 60 Gy have been studied as well. Dose escalation can be achieved using different modalities: fractionated radiation boost, brachytherapy, or stereotactic radiosurgery (SRS). Early studies did suggest an increase in OS with the addition of a boost of 15 to 20 Gy in addition to the standard 50 to 60 Gy, but with increased risk for radiation necrosis. [33] The RTOG and Eastern Cooperative Oncology Group (ECOG) performed a study published in 1988, which randomized 626 patients into four arms: (1) 60 Gy whole-brain radiation therapy (WBRT), (2) 60 Gy WBRT + 10 Gy partial brain boost, (3) 60 Gy WBRT + BCNU, (4) 60 Gy + lomustine (CCNU) + dacarbazine (DTIC). [34] In this study, survival among the various groups, including those that received a 10 Gy boost, were equivalent. Since then, 60 Gy has remained the standard radiation dose for RTOG studies. Boost using intensity-modulated radiation therapy (IMRT) has been studied at the University of Michigan, and reported in 2002. [35] Patients were treated with a 2.5 cm margin around the gross tumor volume (GTV) to 44 Gy, then to 60 Gy with a margin of 1.5 cm around the GTV. A 30 Gy boost was delivered to the GTV plus a 0.5 cm margin, for a total tumor dose of 90 Gy. The goal was improvement in local control. In 78% of the patients, 95% of the recurrence volume was in the 90 Gy region, demonstrating that failures continue to occur locally despite higher doses. Median OS did not change compared to other studies at 11.7 months. There was no benefit from the 30 Gy IMRT boost. Another means to increase the dose of radiation locally, but sparing the normal brain tissue, involves the use of brachytherapy. Retrospective data published in 1999, showed this technique to be promising. [36] The addition of I - 125, improved median survival from 17.9 months in RTOG Class III patients to 28 months. OS in Class IV and V patients improved as well. Unfortunately, prospective studies failed to support these encouraging results. The Brain Tumor Cooperative Group (BTCG), reported in 2002, randomized patients to 60.2 Gy in 35 fractions with BCNU or 60.2 Gy in 35 fractions with BCNU and temporary I - 125 brachytherapy for an additional 60 Gy. [37] Median OS was 68.1 weeks in the I - 125 group versus 58.5 weeks in the group without brachytherapy (p = 0.101). Princess Margaret Hospital performed a similar study, published in 1998, which randomized patients to 50 Gy in 25 fractions versus 50 Gy in 25 fractions with I - 125 seeds for an additional 60 Gy. [38] Again, no benefit was seen. Patients receiving brachytherapy survived a median of 13.8 months versus 13.2 months for those not receiving brachytherapy (p = 0.49). No benefits from brachytherapy were seen in these randomized studies. [Table - 6] summarizes these results. The University of California San Francisco was able to show a benefit from brachytherapy with the addition of hyperthermia, as reported in 1998. [39] Hyperthermia achieves additional cell kill by targeting cells in the S-phase, which are resistant to radiation, but sensitive to heat. Also, it inhibits sublethal repair and improves reoxygenation, thus improving the efficacy of radiation. In this study, hyperthermia was applied 30 minutes before and after implant. Patients receiving hyperthermia had a median OS of 85 weeks versus 76 weeks for brachytherapy alone (p = 0.02). Further studies have not been performed, and given the results from the other prospective brachytherapy studies, upfront brachytherapy has been abandoned for the most part. Another method to achieve additional dose is through the use of SRS. A number of retrospective studies reported in 1999 and 2002, showed benefit with the addition of the SRS boost. [40],[41] The RTOG performed a study randomizing 203 patients to 60 Gy of fractionated radiation with BCNU versus 60 Gy with BCNU and upfront SRS (RTOG 93-05-reported in 2003). [42] Dosing for SRS was determined in part by the results of an earlier RTOG study (reported in 2000), which showed that 24 Gy can be given safely to tumors 2 cm or less. [43] For those greater than 2 cm up to 3 cm, 18 Gy was the recommended dose. For tumors greater than 3 cm up to 4 cm, the recommended dose was 15 Gy. Similar to the results seen in brachytherapy, the results from RTOG 93-05 were disappointing. The median OS was 13.5 months in the SRS arm versus 13.6 in the standard treatment group (p = 0.57). There was no difference in the two- or three-year survival rates. Based largely on this study, the American Society for Therapeutic Radiology and Oncology (ASTRO) issued a consensus statement in 2005 that there was no benefit from the SRS boost for malignant gliomas. [44] Alternative dose-fractionation regimens have also been investigated, with the hope that by hyperfractionating radiation through twice-a-day treatments, higher doses of radiation may be achieved, which may have an advantage in suppressing the growth of the rapidly dividing cells and preventing repopulation. RTOG 83-02 investigated various hyperfractionated dose regimens for all malignant gliomas and found that 72 Gy given in 1.2 Gy per fraction and delivered twice a day resulted in the best median OS with reasonable toxicity. [45] This led to a Phase III study randomizing patients to 72 Gy given in fractions of 1.2 Gy twice daily versus 60 Gy over 30 fractions given daily. [46] BCNU was given in both arms. This study failed to show a benefit from altered fractionation. In fact in patients who were < 50 years old, those receiving the standard fractionation had a median survival of 15.7 months versus 12.2 months for those who were in the hyperfractionation arm (p = 0.02). An additional dose beyond 60 Gy, irrespective of the delivery method, has failed to show any benefit and 60 Gy has remained the standard in the treatment of GBMs. Radiation Volume for Glioblastoma Multiformes Partial brain radiation is standard as there is no benefit to whole-brain radiation in terms of survival or local control. [47] In addition, 90% of the recurrences occur within 2 cm of the known primary tumor. The current RTOG guidelines, as per RTOG 0525, uses a 2.0 to 2.5 cm margin for the initial planning tumor volume (PTV1) depending on the presence of edema and is treated to 46 Gy. The cone-down volume includes a 2.5 cm margin, which is boosted to 60 Gy. In addition, other institutions are using more modern imaging techniques to better define these volumes. At the University of California, San Francisco, magnetic resonance spectroscopy (MRS) is being used to help define their volume. [48] Using edema to delineate microscopic disease is imperfect since surgical changes or mass effect can also cause edema. Imaging that is more specific to tumor may better limit the volume and identify areas of the disease that is not seen by using traditional imaging. Further investigation with MRS is underway. Similarly, the University of Michigan is investigating the use of 11C-methionine positron emission tomography (PET) to define their volume. [49] Certainly, improved imaging techniques, which may incorporate molecular imaging, can change how we define these volumes in the future.Glioblastoma Multiformes in Elderly/Poor Performance Patients The management of GBM in patients above age 70 is controversial, as limited randomized control data is available for this population. Radiation has been shown to be beneficial in elderly patients above the age of 70. In a randomized study published in 2007, the best supportive care was compared to radiation and it was found that radiation improved OS. [50] This study randomized 81 patients, age 70 or older, to 50 Gy of radiation or no radiation. Those receiving radiation had a median survival of 29.1 weeks versus 16.9 weeks for those receiving only supportive care (p = 0.002). No chemotherapy was given. The dose scheme used, however, may not have an impact on the outcome. In a 2004 prospective study of 100 patients, age 60 years or over, the patients were randomized to 60 Gy in 30 fractions versus 40 Gy in 15 fractions. [51] The median OS was 5.1 months for standard radiation compared to 5.6 months for the shorter course (p = 0.57); there was no difference in median overall survival. Again, no chemotherapy was given in this study. As such, the RTOG 0525 study does allow elderly patients to enroll into the study with the presumption that the elderly may benefit from aggressive treatment incorporating chemotherapy. Similarly, other studies are underway to determine if chemotherapy can benefit this subset. Temozolomide alone, without radiation, is being investigated for the elderly. [52] In poor performance status patients, typically those with a KPS < 60, a hypofractionated course of radiation is very reasonable. [53],[54] A palliative dose regimen of 30 Gy in 10 fractions or 37.5 Gy in 15 fractions to the whole brain, or a hypofractionated course of focal radiation to 40-45 Gy in 15 fractions is given to expedite the completion of treatment. Unfortunately, these patients often do poorly with a median survival of approximately seven months. Radiation Sensitizers Motexafin gadolinium (Xcytrin, Pharmacyclics Inc., Sunnyvale, CA), previously known as gadolinium texaphyrin or Gd-Tex, is a redox mediator that selectively targets tumor cells. [54],[55] It catalyzes the oxidation of reducing metabolites, thus allowing for the generation of the reactive oxygen species and fixation of damage by radiation. Animal studies have demonstrated a selective uptake in tumor cells and enhancement of radiation responsiveness. [55],[56],[57] A Phase I study of this drug in GBM found that the maximum tolerated dose was 5 mg/kg/day, given daily for two weeks then thrice per week until the completion of radiation. [58] Temozolomide was not given in this study. With temozolomide now being standard in the treatment of GBMs, RTOG 0613, a Phase I/II study of this drug, with concurrent temozolomide, is underway.Follow-up Typically, patients are followed up with an MRI scan four weeks after completion of their chemoradiation, and every two to three months thereafter. One area of controversy is pseudoprogression. [59] One may see worsening FLAIR (fluid attenuated inverse recovery) or T1 contrast changes soon after the completion of radiation, which may resolve if followed long enough, rather than changing the planned treatment course. Pseudoprogression has yet to be properly defined. How to image pseudoprogression and distinguish it from tumor growth is controversial. Its cause is unknown, although it is seen more frequently with the use of more aggressive upfront treatment. Presumably, there are acute treatment-related changes including blood-brain barrier disruption and edema. As such, when following GBM patients, pseudoprogression must be considered as part of the differential diagnosis. Current work on the understanding of pseudoprogression is ongoing. One recent study points out that knowledge of MGMT promoter methylation status may have a role in the understanding of patients who are more likely to have pseudoprogression compared to those that are unmethylated, and that pseudoprogression may represent the ongoing glioma killing effects. [60] This study evaluated 103 patients and it was discovered that 91% of the methylated MGMT patients had pseudoprogression compared to only 41% of the unmethylated MGMT patients.Future Directions The importance of a multidisciplinary approach involving neurosurgeons, radiation oncologists, and medical oncologists cannot be overemphasized. It has been and will continue to be an integral part of optimal management of all glioma patients. Adjuvant radiation therapy has been shown, in randomized trials, to be the standard of care for many, while the role of chemotherapy will continue to evolve. A few of the new promising chemotherapeutic agents include targeted agents, such as, integrin inhibitor (cilengitide), monoclonal antibodies (cetuximab, bevacizumab), tyrosine kinase inhibitors (vatalanib [PTK 787], vandetibin [ZD 6474]), mammalian target of rapamycin inhibitors such as temsirolimus / everolimus, and protein kinase C inhibitors. These are under investigation and have shown some potential in animals and early phase I and II trials. [61],[62] One small phase II trial with the use of irinotecan and bevacizumab in recurrent malignant gliomas has shown good radiographic response. [62],[63] Another phase II trial has also shown benefit of cilengitide (EMD 121974) on recurrent GBM. [64] Ongoing work with novel agents continues to provide some optimism for the future. For these agents to be used in routine clinical practice in the future, they remain to be tested in the phase III clinical trials. One such trial underway is the phase II/III trial with the CDX-110 (Celldex) vaccine.Conclusions The efficacy of temozolomide has been demonstrated in GBM patients and is being evaluated for LGGs in many ongoing trials. The current standard is observation for low-risk LGGs, while adjuvant focal radiation with chemotherapy is being investigated in RTOG 0424 for high-risk features in LGGs. While focal radiation and chemotherapy have shown benefits in AO and AOA, the role of chemotherapy for AA should be further addressed in additional clinical trials. The standard management for most GBM patients includes concurrent and adjuvant temozolomide with radiation similar to that in the Stupp trial. [30] Among the trials discussed, focal radiation is the mainstay of radiation treatment for the management of most high-grade gliomas as well as LGGs with high-risk features. Results from previous trials provide optimism that benefits realized in higher grade histologies such as GBM can perhaps be extrapolated to lower grade histologies. The results of RTOG 0525 should provide answers to the use of appropriate doses and duration of adjuvant temozolomide for GBMs. The results of RTOG 98-13, although it did not fully accrue, may help address the benefits of temozolomide over the existing standards, such as, PCV or BCNU. Furthermore, a better histological and biological understanding of the molecular basis of tumorgenesis will allow for the development of targeted therapies, and for the selection of patients who are most likely to benefit from adjuvant therapies. [61],[62] The use of the methylation status of MGMT and the identification of 1p and 19q translocation will allow for the selection of subsets of patients who are more likely to benefit with adjuvant treatments. An understanding of anti-angiogenic pathways are paving the way for more effective adjuvant therapies and will likely be the basis of many other trials in the future. In addition, studying DNA repair mechanisms and how to inhibit these may make temozolomide and radiation more effective in the future. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09022t6.jpg] [cn09022t3.jpg] [cn09022t5.jpg] [cn09022t4.jpg] [cn09022t2.jpg] [cn09022t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}