
|
Indian Journal of Cancer
Medknow Publications on behalf of Indian Cancer Society
ISSN: 0019-509X EISSN: 1998-4774
Vol. 46, Num. 2, 2009, pp. 108-119
|
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 108-119
Symposium
Current concepts in the pathology and genetics of gliomas
Sarkar C, Jain A, Suri V
Department of Pathology, All India Institute of Medical Sciences, New Delhi
Correspondence Address:Department of Pathology, All India Institute of Medical Sciences, New Delhi, sarkar.chitra@gmail.com
Code Number: cn09023
Abstract In recent years, there has been a marked improvement in our understanding of molecular genetics of gliomas. These advancements offer hope for development of tailored therapies targeting a tumor's unique molecular profile, and may also translate into improved classification and identification of newer prognostic markers. This review focuses on the neuropathological features of different types of glial neoplasms according to the World Health Organization classification, and the recent advances in their molecular biology with emphasis on the genetic mechanisms underlying tumor progression, diagnostic and prognostic markers and potential therapeutic targets.
Keywords: Glioma, oligodendroglioma, astrocytoma, glioblastoma, 1p/19q deletion
Introduction
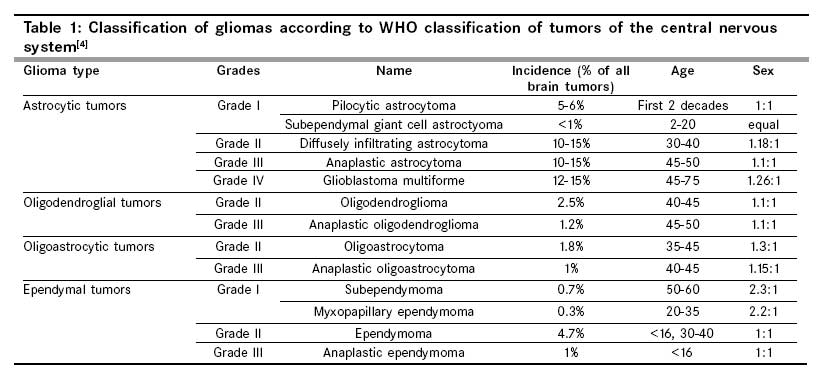
Gliomas are the most common primary brain tumors of adults. Gliomas are classified by the World Health Organization (WHO), according to their morphological characteristics, into astrocytic, oligodendroglial, and mixed tumors. The first WHO classification of tumors of the nervous system was published in 1979, [1] followed by revisions in 1993, [2] 2000, [3] and 2007. [4] The present WHO classification is considered the gold standard for prognostication. [Table - 1] gives the classification of glial tumors with their incidence, age, and sex distribution.
It is unclear whether these tumors result from the transformation of an immature precursor or from the dedifferentiation of a mature glial cell. [5] A number of prognostic and predictive factors are proposed for estimating the behavior of gliomas, including, clinical parameters, histological grading, proliferation indices, and molecular markers. Over the past 20 years, a number of chromosomal, genetic, and epigenetic alterations have been found to be associated with different histological types and malignancy grades of gliomas.
Genotype/phenotype correlation studies have identified early and late genetic alterations related either to astrocytic or oligodendroglial phenotype. They complement the existing WHO morphological classification and provide additional prognostic markers such as 1p/19q deletion in oligodendrogliomas.
Neuropathology of astrocytic tumors
Pilocytic astrocytoma (WHO grade I)
Pilocytic astrocytomas are relatively circumscribed, slow growing, often cystic neoplasms, occurring in children and young adults, most commonly affecting the cerebellum followed by optic nerve and optic chiasma, hypothalamus, thalamus, basal ganglia, and brainstem. [4],[6] Histologically they are characterized by a biphasic pattern consisting of piloid areas with bipolar cells associated with Rosenthal fibers, and protoplasmic areas comprising of loosely textured multipolar cells with microcysts and eosinophilic granular bodies. Sometimes glomeruloid vascular proliferation may be observed, but it is not a sign of malignancy. These cells are strongly glial fibrillary acidic protein (GFAP) immunopositive. Proliferation indices are low with the MIB-1 labeling index (MIB-1 LI) ranging from 0-3.9% (mean 1.1%), [7] however, due to overlap of this range with diffuse astrocytomas grade II (mean 2.3%), it is of little use in diagnosis.
Genetics : Relatively little is known about chromosomal and genetic aberrations in pilocytic astrocytomas. On comparative genomic hybridization of 48 pilocytic astrocytomas, chromosomal imbalances were observed only in seven tumors, most commonly a gain of 9q34.1-qter (three cases). [8] The majority of pilocytic astrocytomas from patients with neurofibromatosis (NF) type 1 carry allelic losses at the NF-1 tumor suppressor gene locus 17q11.2.87. In contrast, sporadic cases rarely demonstrate this allelic loss and neither NF-1 mutations nor loss of NF1 mRNA expression have been demonstrated. [9],[10] This finding argues against an important role of NF1 in the tumorigenesis of sporadic pilocytic astrocytomas. In contrast to diffuse astrocytomas, allelic losses on 17p and mutations in the TP53 tumor suppressor genes are rare in pilocytic astrocytomas. [9],[11],[12] However, one study employing the denaturing gradient gel assay detected TP53 mutation in seven out of 20 such tumors, suggesting that aberrations in p53-dependent growth control also contributes to the pathogenesis of pilocytic astrocytomas. [13]
Diffuse astrocytomas (WHO grade II)
Diffusely infiltrating astrocytomas typically affect young adults and present as cerebral hemispheric masses, with the epicenter lying predominantly in the white matter, although cortical involvement is also common and may account for the seizures experienced by some of these patients. [14] These tumors are characterized by a high degree of differentiation and slow growth, but have an intrinsic tendency for malignant progression to anaplastic astrocytomas and ultimately glioblastoma. Factors accounting for the variable time to progression have not been entirely worked out, although patient age remains a powerful prognostic parameter, inversely associated with survival time. [15] Histological examination reveals a moderately increased cellularity than in a normal brain, well-differentiated fibrillary or gemistocytic or rarely protoplasmic neoplastic astrocytes, with occasional nuclear atypia in a loosely structured, often microcystic tumor matrix. Grade II astrocytomas lack mitotic activity, endothelial proliferation, and necrosis. MIB-1 LI (usually < 4%) may provide useful information beyond that of simple mitosis counting, although there are no defined cut-off values, and there are significant methodological and interpretive differences among different laboratories. [7] However, an MIB-LI > 5% has been said to constitute a threshold value for predicting shorter survival. [16] GFAP immunoreactivity is strong in the gemistocytic and fibrillar variants, whereas, protoplasmic astrocytomas are only weakly positive. [6] Vimentin and S-100 are also usually positive, but have relatively little diagnostic relevance.
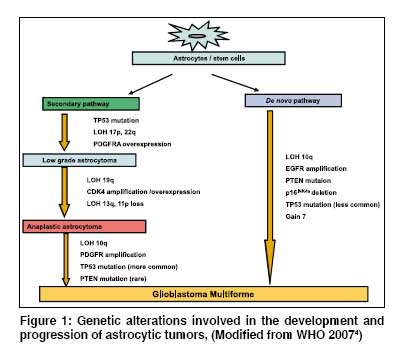
Genetics [Figure - 1]: About 60% of the diffuse astrocytomas carry mutations in the TP53 tumor suppressor gene at 17p13.1. [17],[18] Gemistocytic astrocytomas carry TP53 mutation in up to 80% of the cases. [19] In most cases TP53 mutation is accompanied by loss of heterozygosity (LOH) on 17p resulting in a complete absence of the wild-type TP53 gene. [6] Diffuse astrocytomas also frequently show elevated expression of platelet-derived growth factor receptor A (PDGFRA) and the corresponding ligand PDGFA. [20],[21] Overexpression of PDGFRA in diffuse astrocytic gliomas has been found preferentially in tumors showing LOH on 17p. [22] The prognostic significance of TP53 overexpression in diffuse astrocytomas is controversial. In a large retrospective study on diffuse astrocytomas, TP53 mutations were not associated with an overall change in the prognostic outcome. [23]
Anaplastic astrocytoma (WHO grade III)
Similar to diffuse astrocytomas, anaplastic astrocytomas are preferentially located in the cerebral hemispheres, but occur in a slightly older age group. They are histologically characterized by nuclear atypia, increased cellularity and significant proliferative activity. Additional signs of anaplasia include multinucleated tumor cells and abnormal mitosis. Initially, the St. Anne-Mayo astrocytoma grading scheme, essentially adopted in the 1993 version of the WHO system, stated that even a single mitotic figure is sufficient to warrant an anaplastic or grade III designation. [24] However, the "one mitosis" rule is questionable for large resection specimens, where it does not have the same dire implications as in a small biopsy. Survival times for anaplastic astrocytoma patients with solitary mitosis have been found to be similar to those of grade II astrocytoma patients, [7],[25] and later WHO classifications take the sample size into consideration, for defining the anaplastic features. The typical histological hallmarks of glioblastoma (microvascular proliferation and necrosis) are not yet present, but anaplastic astrocytomas tend to progress to secondary glioblastomas. [6] MIB-1 LI is usually 5-10%, but may overlap with low grade diffuse astrocytoma as well as glioblastoma, and show considerable variation even within a given tumor. [16],[26],[27]
Genetics [Figure - 1]: Gains of chromosome 7 and TP53 mutations are similarly frequent in anaplastic astrocytomas as also in diffuse astrocytomas. In addition, these tumors may carry deletions on chromosomes 6, 9p, 11p, 19q, and 22q. The target genes on 9p are the CDKN2A, p14 ARF , and CDKN2B tumor suppressor genes. [28],[29] A small fraction demonstrates amplification and overexpression of the CDK4 gene at 12q13-q1 [30] , and this alteration occurs preferentially in tumors without CDKN2A deletion or mutation. [31] In addition, a subset carries mutations in the retinoblastoma (RB1) gene. [18],[31] In contrast to glioblastomas (discussed a little later in the article), mutations of the PTEN gene on 10q23 are restricted to < 10% anaplastic astrocytomas and when present indicate a poor prognosis. [32] Although detected with much less frequency than in grade IV tumors, epidermal growth factor receptor (EGFR) overexpression and / or gains of chromosome 7 in low grade (WHO II) and grade III astrocytomas are linked with shortened survival. [33],[34],[35]
Glioblastoma Multiforme (WHO grade IV)
Glioblastoma multiformes (GBMs) are the most frequent and the most malignant primary brain tumors and occur typically in older adults, preferentially in the cerebral hemispheres. The clinical history is usually short (mostly < three months). Microscopically, glioblastomas are cellular, highly anaplastic tumors, which may be composed of cells of various morphologies including fibrillar and gemistocytic astrocyte-like cells, fusiform cells, small anaplastic cells, and pleomorphic multinuclear giant cells. Nuclear atypia is usually marked, and high mitotic activity, including atypical forms, is a prominent feature. The presence of pathological microvascular proliferation and / or necrosis is essential for the diagnosis. Microvascular proliferation often results in the formation of glomeruloid garland-like capillary structures. Vascular thromboses are also common. With respect to necroses, two types may be distinguished: (a) large confluent ischemic necrosis and (b) small, often multiple, irregularly shaped, band-like or serpiginous foci of necrosis, typically surrounded by glioma cells in a pseudopallisading pattern. [6]
The WHO classification lists two glioblastoma variants, namely, the giant cell glioblastoma and the gliosarcoma. Giant cell glioblastomas are relatively well-circumscribed (which may account for somewhat better prognosis) and histologically comprise of bizarre highly pleomorphic multinucleated giant cells. Gliosarcomas are a rare variant of GBM, characterized by a biphasic tissue pattern with areas displaying phenotypic features of gliomas and sarcomas. [6],[36] In addition, the term "glioblastoma with oligodendroglial component" is suggested for those glioblastomas that contain areas with features generally associated with oligodendroglial differentiation; however, the histological criteria for the classification of these tumors are poorly defined, making their differential diagnosis towards anaplastic oligoastrocytoma and ordinary glioblastoma a difficult and subjective issue. Nevertheless, it appears that glioblastoma with the oligodendroglial component may be associated with a better prognosis and a higher likelihood of a favorable response to adjuvant treatment than ordinary glioblastomas. [36],[37],[38],[39] The term ′small cell glioblastoma′ refers to a subset of GBMs that show a highly monomorphic cell population, characterized by small, densely packed cells with mild hyperchromasia and modest atypia, long thin GFAP positive cytoplasmic processes, and markedly elevated MIB-1 LI. [40]
Glioblastoma multiforme can either develop by progression from less malignant gliomas (secondary glioblastomas) or, more frequently, develop rapidly in a de novo manner with no evidence of a previous lesion of lower grade malignancy (primary glioblastomas). [41] Morphologically, primary and secondary glioblastomas cannot be distinguished. Clinically, secondary glioblastomas tend to occur in younger patients, below the age of 45 years, while primary glioblastomas account for the vast majority of glioblastomas in older patients. The prognosis of primary and secondary glioblastomas seems to be equally poor when adjusted for patient age. [42]
In glioblastomas GFAP immunoreactivity is heterogeneous, with poorly differentiated and small anaplastic glioma cells being frequently negative. MIB-1 LI shows great regional variation with mean values ranging from 15-20%. [23],[33],[43] Despite the wide range of proliferation indices observed, no association with the clinical outcome of GBM patients has been established. [43]
Genetics [Figure - 1]: In adults, at least two distinct molecular pathways leading to the development of GBM have been identified. Primary ( de novo ) GBM`s frequently harbor amplification of the epidermal growth factor receptor (EGFR, 7p12), are associated with an older age of onset, and an aggressive clinical course. The majority of these tumors will express wild-type EGFR and / or variant mutant forms of the EGFR. The most common mutant form is designated EGFRvIII (also called de2-7EGFR or delta EGFR), which results from an in-frame deletion of exons 2 to 7, resulting in the loss of a portion of the extracellular domain of the receptor. In contrast, the evolution of secondary glioblastoma from the lower-grade precursor lesions is characterized by alterations of the p53 gene (17p13.1) and a more protracted clinical course. [44],[45],[46] Although p53 mutation and EGFR amplification are generally mutually exclusive, occasional glioblastomas harbor both alterations. [46]
Primary glioblastomas also more frequently demonstrate the homozygous deletion of CDKN2A and p14 ARF , CDK4 amplification, MDM2 or MDM4 amplification, RB1 mutation/homozygous deletion, monosomy 10, and PTEN mutation. TP53 mutation is found in approximately 30% of primary GBMs [36],[47],[48],[49],[50] Secondary GBMs carry TP53 mutation in more than 60% of the cases, while amplification of EGFR, MDM2 or MDM4, and PTEN are rare. [51] Allelic losses on 19q and 13q, promoter hypermethylation of the RB1 gene, and overexpression of the PDGFRA are more common in secondary GBMs. [36],[47],[52]
These data indicate that primary and secondary GBMs carry different genetic alterations. However, the functional consequences of the different alterations are similar, since they result in alteration of the same pathways, namely the p53, pRB1, PTEN/PI 3-kinase/Akt, and mitogen-activated protein kinase pathways.
In the GBM group also, as in diffuse astrocytomas, there is conflicting evidence as to whether or not p53 alterations independently correlate with patient survival, although they may indirectly impact prognosis in certain patient subgroups, [23],[53],[54],[55],[56],[57],[58] such as, being a marker of age (more common in younger patients) and tumor biology. [59] Therefore, knowledge of the presence of TP53 mutation appears to be of little clinical value. The predictive value of EGFR amplification in grade IV tumors is also unclear with different studies showing conflicting results. [60],[61],[62],[63],[64],[65] Mutations in EGFR and EGFRvIII variants are particularly common in malignant astrocytomas exhibiting a small cell phenotype, which behave as aggressively as primary glioblastomas, and EGFRvIII overexpression has been associated with poorer survival. [14],[66],[67],[68]
Second only to gains on chromosome 7, losses involving chromosome 10 are quite frequent in astrocytomas, limited mainly to high grade tumors. [69],[70] LOH 10q is the most frequent genetic alteration in glioblastomas and occurs in 60-80% of the cases. [71],[72],[73] To date, most studies have identified 10q loss / monosomy 10 as an independent predictor of shorter patient survival. [69],[70],[74],[75],[76],[77],[78] Several candidate tumor suppressor genes have been mapped to 10q, including PTEN (10q23), DMBT1 (10q25.5-26.1), and recently annexinVII (ANX7;10q21). [69],[72],[73],[79] The available data on PTEN alteration and survival of glioblastomas patients are heterogeneous. In several studies, PTEN mutations are not associated with prognosis of glioblastomas patients. [32],[54],[77],[80] Terada et al . identified LOH around PTEN as a predictor of less favorable prognosis in a set of 40 astrocytomas (grades II-IV). [81] Sano et al. reported that the PTEN mRNA level is an independent prognostic factor for glioblastomas patients with low PTEN transcript levels, having significantly shorter survival times. [82]
The MGMT (O6-methylguanine-DNA methyltransferase) gene is located on chromosome 10q26 and encodes a DNA-repair protein that removes alkyl groups from the O6 position of guanine, protecting the cells against alkylating agents. Methylation of promoter CpG islands results in loss of MGMT expression and is frequently seen in glioblastomas (45-75%) and has been shown to be associated with longer overall survival in patients with glioblastoma who have received alkylating chemotherapy with temozolomide. [83],[84],[85],[86] Also, irrespective of treatment, MGMT promoter methylation is considered an independent favorable prognostic factor for GBMs. [84] Secondary GBM shows a higher frequency of MGMT promoter methylation than the primary GBM. [83],[84]
Several studies have been carried out in India on the biology, initiation, and progression of these tumors. Pathways for GBM have been worked out and correlation with outcome defined. The roles of c-myc, EGFR, and the Rb gene have also been studied in gliomas. A new genetic marker for astrocytic tumors located in the 17p13.3 region harboring several putative tumor suppressor genes. including HIC-1. has been shown for the first time. The correlation of these markers with tumor grade, proliferation, and apoptosis has been extensively evaluated. [87],[88],[89],[90],[91],[92],[93],[94],[95],[96],[97],[98]
Neuropathology of Oligodendroglial Tumors
Oligodendroglioma (WHO grade II)
These are diffusely infiltrating gliomas of adults, which can occur at any age or location, but are distinctly uncommon in children and are almost never encountered in the brainstem, cerebellum or spinal cord. The majority present as hemispheric masses in young to middle-aged adults, with the frontal lobe representing a favored location. [14] Progression to anaplastic oligodendrogliomas does occur, but less frequently than in astrocytomas. [99] Several studies have confirmed the WHO grading of oligodendroglial tumors as a significant predictor of survival. [100],[101],[102],[103] On histological examination, grade II oligodendrogliomas are diffusely infiltrating tumors of moderate cellularity, composed of monomorphic cells, with uniform round nuclei bland chromatin, clear perinuclear haloes on paraffin sections imparting a "fried egg" appearance, and a rich, branching capillary network reminiscent of "chicken wire". It is important to recognize that the "fried egg" appearance represents a formalin fixation artifact that is neither absolutely necessary for diagnosis nor is it encountered in frozen sections or rapidly fixed specimens. Other common, though slightly less specific findings include extensive cortical involvement, microcalcifications, mucin-rich microcystic spaces, and perineuronal satellitosis. [14] There is no immunohistochemical marker available that allows the specific and sensitive recognition of oligodendroglial tumor cells. GFAP may be present in intermingled reactive astrocytes as well as in neoplastic oligodendroglial cells such as minigemistocytes and gliofibrillary oligodendrocytes. Other markers expressed are vimentin, S-100, and MAP-2, along with oligodendrocyte lineage specific transcription factors OLIG-1 and OLIG-2, but these are expressed in a vast majority of other gliomas. However, oligodendroglial tumors usually lack nuclear TP53 staining. The proliferation indices are low in grade II oligodendrogliomas (usually < 5%). [99]
Anaplastic oligodendrogliomas (WHO grade III)
Oligodendrogliomas with focal or diffuse features of malignancy and less favorable prognosis fall in this group, and occur approximately seven to eight years later, on an average, than grade II oligodendrogliomas. [100],[104] They share, with WHO grade II oligodendrogliomas, a preference for the frontal lobe, followed by the temporal lobe. They may develop either de novo or by progression from pre-existing grade II oligodendrogliomas. The majority of tumor cells demonstrate features reminiscent of oligodendroglial cells, that is, rounded hyperchromatic nuclei, perinuclear haloes, focal microcalcification, and branching vascular pattern. Anaplastic features linked to malignancy in oligodendrogliomas are similar to those in astrocytic gliomas, that is, high cellularity, marked cytological atypia, high mitotic activity, microvascular proliferation and necrosis with or without pseudopalisading. Usually several of these features are present, but the diagnosis of grade III anaplastic oligodendroglioma requires the presence of either conspicuous microvascular proliferation and / or high mitotic activity. In doubtful cases, MIB-1 LI and clinicoradiological correlation may be helpful in assessing the prognosis. [104] Gliofibrillary oligodendrocytes and minigemistocytes are frequent in anaplastic oligodendrogliomas, but are not of prognostic significance. [105]
Genetics of Oligodendroglial Tumors [Figure - 2]
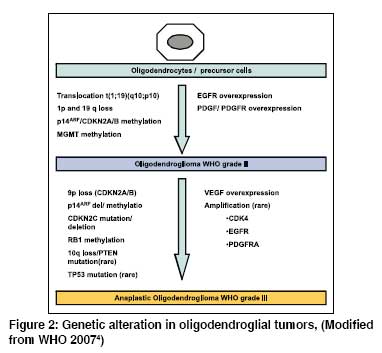
The molecular abnormalities frequently associated with grade II oligodendrogliomas include (i) LOH for chromosomes 1p, 19q, and 4q, and (ii) overexpression of EGFR, PDGFR, and PDGF. Anaplastic oligodendrogliomas grade III more frequently have (i) mutations / deletions of CDKN2A and CDKN2C, (ii) amplification of CDK4, EGFR, MYC, (iii) LOH for 1p, 19q, 9p, and 10 q, and (iv) overexpression of vascular endothelial growth factor receptor (VEGFR). [106],[107],[108],[109]
LOH of 1p/19q: In 1994, Reifenberger et al . reported that allelic loss of chromosome 19q was detectable in 81% oligodendroglial tumors, of which approximately 75% also exhibited LOH at 1p locus. [108] Subsequently several studies have confirmed that a combined loss of large chromosomal regions at these loci is the hallmark of oligodendroglial tumors. These structural lesions have been detected in up to 90% of the oligodendrogliomas. [110],[111],[112],[113],[114],[115],[116] In adults, combined 1p and 19q LOH has been observed in up to 83% of pure oligodendrogliomas, 63% of anaplastic oligodendroglioma, 56% of mixed low-grade oligoastrocytoma, and 52% of anaplastic mixed oligoastrocytoma. [117],[118],[119] The frequency of LOH 1p/19q is lower in anaplastic oligodendrogliomas, indicating a wider spectrum of genetic alterations leading to these tumors. [120] Fuller and Perry found 1p/19q co-deletion to be highly associated with morphology: 84% in oligodendrogliomas, 15% in mixed oligoastrocytomas (MOAs) and 1% in astrocytomas (P < 0.001). [121] Loss of 19q alone has been described in a smaller subset and is particularly common in MOAs.
To explain the mechanism of dual 1p/19q co-deletion, recently Griffin et al . [122] and Jenkins et al . [123] hypothesized that there occurs a balanced whole-arm translocation t(1;19)(q10:p10) between chromosomes 1 and 19 forming two derivative chromosomes, one composed of 1q and 19p, the other of 1p and 19q. Subsequent loss of der(1;19)(p10;q10) then results in the simultaneous 1p and 19q loss observed in the oligodendroglioma, with retention of der(1;19)(q10;p10) seen in these cases. All informative markers on 1p/19q demonstrate that LOH makies the localization of relevant tumor suppressor genes difficult. Although the precise mechanism(s) relating to the whole chromosome arm loss of 1p and 19q to tumorigenesis remains a mystery, it is possible that: (1) haploinsufficiency of multiple genes is somehow sufficient without the need for a "second hit", (2) epigenetic events such as hypermethylation of CpG islands are inactivating genes on the remaining copies of 1p and 19q, or (3) this cytogenetic signature is simply a marker of a specific glioma type, mechanistically unrelated to other, yet-to-be identified tumorigenic events. [121]
Whatever the mechanism of tumorigenesis, oligodendrogliomas are the first CNS neoplasms in which a genetic signature, namely, 1p and 19q deletion, has been associated, with outcome and response to chemotherapy. [121],[124],[125],[126],[127] LOH for 1p and 19q has correlated with the response to chemotherapy and increase in overall survival. [101],[119],[128],[129] A five-year survival rate of 95% has been observed for those with deletions versus 65% for those without deletions. Those with deletions also have a longer overall survival of 172 months vs. 105 months without deletions. [101],[130] In a series of 39 patients with anaplastic oligodendroglioma, nearly all of the 70% cases with positive response to procarbazine, lomustine, and vincristine (PCV) chemotherapy exhibited LOH 1p/19q. Another study confirmed the association of LOH 1p/19q and prolonged overall survival in oligodendrogliomas WHO grade II, while no survival advantage was observed in patients with oligoastrocytomas or glioblastomas with LOH 1p/19q. [119] Studies indicate a similar outcome in patients with LOH 1p/19q treated at the time of diagnosis with both PCV chemotherapy and radiotherapy or only with chemotherapy. [131] Other recently published studies support this positive correlation between LOH 1p/19q and survival. [132],[133],[134],[135],[136] Two recent phase III prospective trials, namely, RTOG 9402 (Radiation therapy oncology group) and EORTC 26951 (European organization for research and treatment of cancer) have included correlative analyses of 1p and 19q deletions in tumor specimens of anaplastic oligodendrogliomas and anaplastic oligoastrocytomas. Both involved radiation therapy along with PCV chemotherapy in the treatment protocol. The RTOG 9402 study showed that LOH for either 1p or 19q was a significant independent prognostic variable correlating with the outcome (p = 0.01). In EORTC 26951, a significant difference in survival was also observed for patient with 1p/19q loss as compared to those without deletions (p = 0.003). [137],[138],[139],[140] The findings from these two phase III studies, the largest to date on newly diagnosed oligodendrogliomas, suggest that there is no improvement in survival with the addition of PCV to RT, and the timing of the PCV with respect to RT is also irrelevant. It was also interesting to note in these prospective studies that 1p and 19q deletions are associated with improved outcome, regardless of treatment. Thus, combined loss of 1p and 19q identified a favorable prognostic group in both studies, which appeared independent of the treatment arms. Irrespective of whether a patient was treated with RT alone or with PCV and RT, the survival was better if the patient had 1p/19q deletions. Giannini et al . [141] in their recent study on refining the correlation among histopathology, 1p 19q deletion, and clinical outcome in intergroup RTOG trial 9402 found that (i) overall survival (OS) of patients with classical features of oligodendrogliomas was significantly longer than for patients without these features ( P < 0.0001) and they were not affected by necrosis, (ii) Classic oligodendroglial morphology was highly associated with 1p 19q deletion, present in 80% of classic for oligodendroglioma (CFO) and in only 13% lacking classic features of oligodendroglioma (NCFO), (iii) On multivariate analysis, both classic oligodendroglial morphology and 1p 19q deletion remained significantly associated with progression free survival (PFS) and OS, (iv) Patients with CFO, treated with PCV-plus-RT, showed a trend toward increased survival compared with CFO treated with RT ( P = 0.08).
Given the significance of these findings, it is not surprising that many institutions have initiated testing for 1p/19q deletions, for prognostic information that this testing provides, and some clinicians are basing treatment decision on these markers. It is also unclear if the more favorable clinical outcome associated with these molecular changes is simply due to a better response to treatment or other inherent molecular characteristics yet to be elucidated. [127] In a recent review on the clinicopathological aspects of 1p / 19q status, Aldape et al . [142] concluded that it is an important marker in oligodendrogliomas and its loss is associated with classic oligodendroglioma histology as well as improved prognosis. Thus, the combined 1p / 19q marker will continue to be a clinically useful marker of prognosis and could potentially be incorporated into the diagnostic criteria in the future.
Other genetic alterations and prognosis [Figure - 2]:
The incidence of TP53 mutation in oligodendroglial tumors is not as frequent as in astrocytomas, remaining within the range of 10-20%. [98],[119] It has been noted that TP53 mutations were almost exclusively found in oligodendrogliomas without 1p loss. LOH 10q, frequently seen in glioblastomas has been observed in up to 58% of anaplastic oligodendrogliomas, and associated with a poorer outcome in some studies, but not in others. [143],[144],[145] An inverse association between LOH 10q and LOH 1p/19q has frequently been noted. [131],[135],[146],[147] PTEN on 10q23.31 is frequently mutated in glioblastomas and altered in 3-10% of grade III oligodendrogliomas. [143],[147],[148],[149] In an analysis of 72 oligodendrogliomas, 10 q was identified in 14 of 67 (21%), including the PTEN and DMBT1 regions. PTEN gene alterations have been associated with poorer survival in oligodendrogliomas, even in patients with chemotherapy sensitive tumors. [150]
Alterations of chromosome 9p have been encountered in oligodendrogliomas, albeit at a lower frequency than is typical for high-grade astrocytic lesions. [108],[135],[146],[148],[151],[152] Likewise, deletions of p16 have been associated with anaplasia and worsened survival. [132],[153],[154],[155] Another negative molecular indicator for overall survival and anaplastic oligodendrogliomas has been found to be CDKN2A/p16 deletion. [156] However, only small groups of patients have as yet been analyzed regarding these genetic alterations.
Promoter hypermethylation of MGMT (O6-methylaguanine-DNA methyltransferase) on 10q26.3 has been observed in 60-80% of oligodendroglial tumors, and an association with 1p / 19q status and tumor grade is reported. [157],[158]
Neuropathology of Oligoastrocytic tumors
Mixed Oligoastrocytoma (WHO grade II)
Mixed Oligoastrocytoma (MOA) are diffusely infiltrating gliomas composed of a mixture of two distinct neoplastic cell types, morphologically resembling the tumor cells in oligodendrogliomas and diffuse astrocytomas of WHO grade II. [159] They usually develop in middle-aged individuals (35-45 years), preferentially in cerebral hemispheres. [100],[160],[161] Of all the gliomas, MOAs remain the most difficult to define, are least reproducible, and most likely to receive discordant diagnoses from expert neuropathologists around the country. [14] Nevertheless, the WHO recognizes two basic patterns, (1) a biphasic ("compact") variant, where the two elements are spatially distinct, and (2) an intermingled ("diffuse") variant, where the cell types are interspersed. The former, though more often illustrated, is far less common than the latter. A diffuse admixture of GFAP positive minigemistocytes and gliofibrillary oligodendrocytes with an oligodendroglial component should not be confused as oligoastrocytoma instead of oligodendroglioma. Only tumors in which fibrillary, protoplasmic or classic gemistocytic astrocytic cells are present, in addition to the oligodendroglial tumor, qualify as oligoastrocytoma. [159] Both the components show the same immunoreactivity patterns as ′pure′ oligodendrogliomas and astrocytomas, respectively. GFAP and vimentin expression are more consistently found in the astroglial component, while they are variably expressed in oligodendroglial tumor cells. About one-third demonstrate nuclear p53 overexpression. [162] MIB-1 LI is usually low (< 6%). [163]
Anaplastic Oligoastrocytoma (AOA) (WHO grade III)
As with other high grade gliomas, AOA occur at a higher age (mean age 44 years). [164] They are predominantly hemispheric. AOA are oligoastrocytomas with histological features of anaplasia, including nuclear atypia, cellular pleomorphism, high cellularity, and high mitotic activity. In addition, microvascular proliferation may be present. [159] MIB-1 LI correlates with the presence of anaplastic features. The presence of necrosis in AOA, in contrast to AO, has been seen to be associated with a significantly worse prognosis. Even though prognosis of patients with AOA is better than classical glioblastomas, AOA with necrosis according to some authors should be classified as ′glioblastoma with oligodendroglial component". [37],[164],[165]
Genetics of oligoastrocytic tumors [Figure - 3]
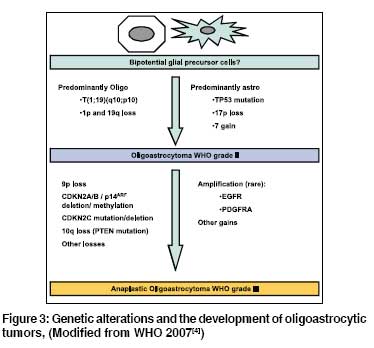
The molecular genetic alterations underlying oligoastrocytomas resemble those of oligodendrogliomas and astrocytomas. About 30-50% of oligoastrocytomas (predominantly nontemporal) are characterized by combined loss of 1p and 19q, while 30% (predominantly temporal) carry the TP53 mutations, with both these alterations being mutually exclusive. [108],[109],[112],[116] As for oligodendrogliomas, a combined 1p / 10q loss is associated with favorable prognosis. [166],[167] In AOA, 1p loss alone has been seen to be an independent marker of improved progression and free and overall survival. [166]
References
| 1. | Zulch KJ. Histological typing of tumors of the central nervous system. Internatinal histological classification of tumors, no.21. Geneva: World Health Organization; 1979. Back to cited text no. 1 |
| 2. | Kleihues P, Burger PC, Scheithauer BW. Histological typing of tumors of the central nervous system. 2nd ed. International histological classification of tumors. Berlin, Heidelberg, New York: Springer; 1993. Back to cited text no. 2 |
| 3. | Kleihues P, Cavenee WK. Pathology and genetics of tumors of the nervous system. World Health Organization classification of tumors. Lyon: IARC; 2000. Back to cited text no. 3 |
| 4. | Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, editors. World Health Organization classification of tumors of the central nervous system. Lyon: IARC; 2007. Back to cited text no. 4 |
| 5. | Sanson M, Thillet J, Hoang-Xuan K. Molecular changes in gliomas. Curr Opin Oncol 2004;16:607-13. Back to cited text no. 5 |
| 6. | Reifenberger G, Collins VP. Pathology and molecular genetics of astrocytic gliomas. J Mol Med 2004;82:656-70. Back to cited text no. 6 |
| 7. | Giannini C, Scheithauer BW, Burger PC, Christensen MR, Wollan PC, Sebo TJ, et al . Cellular proliferation in pilocytic and diffuse astrocytomas. J Neuropathol Exp Neurol 1999;58:46-53. Back to cited text no. 7 |
| 8. | Sanoudou D, Tingby O, Ferguson-Smith MA, Collins VP, Coleman N. Analysis of pilocytic astrocytoma by comparative genomic hybridization. Br J Cancer 2000;82:1218-22. Back to cited text no. 8 |
| 9. | Kluwe L, Hagel C, Tatagiba M, Thomas S, Stavrou D, Ostertag H, et al . Loss of NF1 alleles distinguish sporadic from NF1 associated pilocytic astrocytomas. J Neuropathol Exp Neurol 2001;60:917-20. Back to cited text no. 9 |
| 10. | Wimmer K, Eckart M, Meyer-Puttlitz B, Fonatsch C, Pietsch T. Muatational and expression analysis of the NF1 gene argues against a role as tumor suppressor in sporadic pilocytic astrocytomas. J Neuropathol Exp Neurol 2002;61:1896-902. Back to cited text no. 10 |
| 11. | Ohgaki H, Eibl RH, Schwab M, Reichel MB, Mariani L, Gehring M, et al . Mutations of the p53 tumor suppressor gene in neoplasms of the human nervous system. Mol Carcinog 1993;8:74-80. Back to cited text no. 11 |
| 12. | Lang FF, Miller DC, Pisharody S, Koslow M, Newcom EW. High frequency of p53 protein accumulation without p53 gene mutation in human juvenile pilocytic, low grade and anaplastic astrocytomas. Oncogene 1994;9:949-54. Back to cited text no. 12 |
| 13. | Hayes VM, Dirven CM, Dam A, Verlind E, Molenaar WM, Mooij JJ, et al . High frequency of TP53 mutations in juvenile pilocytic astrocytomas indicates role of TP53 in the development of these tumors. Brain Pathol 1999;9:463-7. Back to cited text no. 13 |
| 14. | Perry A. Pathology of low grade gliomas: An update of emerging concepts. Neuro Oncol 2003;5:168-78. Back to cited text no. 14 |
| 15. | Shafqat S, Hedley-Whyte ET, Henson JW. Age-dependent rate of anaplastic transformation in low-grade astrocytoma. Neurology 1999;52:867-9. Back to cited text no. 15 |
| 16. | Jaros E, Perry RH, Adam L, Kelly PJ, Crawford PJ, Kalbag RM, et al . Prognsotic implications of P53 protien, epidermal growth factor receptor, and Ki-67 labelling in brain tumors. Br J Cancer 1992;66:373-85. Back to cited text no. 16 |
| 17. | Kleihues P, Davis RL, Ohgaki H, Burger PC, Westphal M, Cavenee WK. Diffuse astrocytoma. In: Kleihues P, Cavenee WK, editors. Pathology and genetics of tumors of the nervous system. World Health Organization classification of tumors. Lyon: IARC; 2000.p. 22-6. Back to cited text no. 17 |
| 18. | Ichimura K, Bolin MB, Goike HM, Schmidt EE, Moshref A, Collins VP. Deregulation of the p14ARF/Mdm2/p53 pathway is a prerequisite for human astrocytic gliomas with G1-S transition control gene abnormalities. Cancer Res 2000;60:417-24. Back to cited text no. 18 |
| 19. | Watanabe K, Peraud A, Gratas C, Wakai S, Kleihues P, Ohgaki H. p53 and PTEN gene mutations in gemistocytic astrocytomas. Acta Neuropathol (Berl) 1998;95:559-64. Back to cited text no. 19 |
| 20. | Hermanson M, Funa K, Hartman M, Claesson-Welsh L, Heldin CH, Westermark B, et al . Platelet-derived growth factor and its receptors in human glioma tissue: Expression of messenger RNA and protein suggests the presence of autocrine and paracrine loops. Cancer Res 1992;52:3213-9. Back to cited text no. 20 |
| 21. | Guha A, Dashner K, Black PM, Wagner JA, Stiles CD. Expression of PDGF and PDGF receptors in human astrocytomas operation specimens supports the existence of an autocrine loop. Int J Cancer 1995;60:168-73. Back to cited text no. 21 |
| 22. | Hermanson M, Funa K, Koopmann J, Maintz D, Waha A, Westermark B, et al . Association of loss of heterozygosity on chromosome 17p with high platelet-derived growth factor alpha receptor expression in human malignant gliomas. Cancer Res 1996;56:164-71. Back to cited text no. 22 |
| 23. | Peraud A, Kreth FW, Wiestler OD, Kleihues P, Reulen HJ. Prognostic impact of TP53 mutations and p53 protein overexpression in supratentorial WHO grade II astrocytomas and oligoastrocytomas. Clin Cancer Res 2002;8:1117-24. Back to cited text no. 23 |
| 24. | Daumas-Duport C, Scheithauer BW, O'Fallon J, Kelly P. Grading of astrocytomas. A simple and reproducible method. Cancer 1988;62:2152-65. Back to cited text no. 24 |
| 25. | Perry A, Jenkins RB, O'Fallon JR, Schaefer PL, Kimmel DW, Mahoney MR, et al . Clinicopathologic study of 85 similarly treated patients with anaplastic astrocytic tumors: An analysis of DNA content (ploidy), cellular proliferation, and p53 expression. Cancer 1999;86:672-83. Back to cited text no. 25 |
| 26. | Coons SW, Johnson PC. Regional heterogeneity in the proliferative activity of human gliomas as measured by the Ki-67 labeling index. J Neuropathol Exp Neurol 1993;52:609-18. Back to cited text no. 26 |
| 27. | Karamitopoulou E, Perentes E, Diamantis I, Maraziotis T. Ki-67 immunoreactivity in human central nervous system tumors: A study with MIB-1 monoclonal antibody on archival material. Acta Neuropathol 1994;87:47-54. Back to cited text no. 27 |
| 28. | Ruas M, Peters G. The p16INK4a/CDKN2A tumor suppressor and its relatives. Biochim Biophys Acta 1998;1378:F115-77. Back to cited text no. 28 |
| 29. | Roussel MF. The Ink4 family of cell cycle inhibitors in cancer. Oncogene 1999;18:5311-7. Back to cited text no. 29 |
| 30. | Reifenberger G, Reifenberger J, Ichimura K, Meltzer PS, Collins VP. Amplification of multiple genes from chromosomal region 12q13-14 in human malignant gliomas: Preliminary mapping of the amplicons shows preferential involvement of CDK4, SAS, and MDM 2. Cancer Res 1994;54:4299- 303. Back to cited text no. 30 |
| 31. | Ichimura K, Schmidt EE, Goike HM, Collins VP. Human glioblastomas with no alterations of the CDKN2A (p16INK4A, MTS1) and CDK4 genes have frequent mutations of the retinoblastoma gene. Oncogene 1996;13:1065-72. Back to cited text no. 31 |
| 32. | Smith JS, Tachibana I, Passe SM, Huntley BK, Borell TJ, Iturria N, et al . PTEN mutation, EGFR amplification, and outcome in patients with anaplastic astrocytomas and glioblastoma multiforme. J Natl Cancer Inst 2001;93:1246-56. Back to cited text no. 32 |
| 33. | Wessels PH, Twijnstra A, Kessels AG, Krijne-Kubat B, Theunissen PH, Ummelen MI, et al . Gain of chromosome 7, as detected by in situ hybridization, strongly correlates with shorter survival in astrocytomas grade 2. Genes Chromosomes Cancer 2002;33:279-84. Back to cited text no. 33 |
| 34. | Kunwar S, Mohapatra G, Bollen A, Lamborn KR, Prados M, Feuerstein BG. Genetic subgroups of anaplastic astrocytomas correlate with patient age and survival. Cancer Res 2001;61:7683-8. Back to cited text no. 34 |
| 35. | Varela M, Ranuncolo SM, Morandi A, Lastiri J, De Kier Joffι EB, Puricelli LI, et al . EGFR and PDGFR, but not bcl-2 overexpression predict overall survival in patients with low grade astrocytomas. J Surg Oncol 2004;86:34-40. Back to cited text no. 35 |
| 36. | Kleihues P, Burger PC, Aldape KD, Brat DJ, Biernat W, Bigner DD, et al . Glioblastoma. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, editors. World Health Organization classification of tumors of the central nervous system. Lyon: IARC; 2007. p. 33-49. Back to cited text no. 36 |
| 37. | Kraus JA, Lamszus K, Glesmann N, Beck M, Wolter M, Sabel M, et al . Molecular genetic alterations in glioblastomas with oligodendroglial component. Acta Neuropathol 2001;101:311-20. Back to cited text no. 37 |
| 38. | He J, Mokhtari K, Sanson M, Marie Y, Kujas M, Huguet S, et al . Glioblastomas with an oligodendroglial component: A pathological and molecular study. J Neuropathol Exp Neurol 2001;60:863-71. Back to cited text no. 38 |
| 39. | Homma T, Fukushima T, Vaccarella S, Yonekawa Y, Di Patre PL, Franceschi S, et al . Correlation among pathology, genotype, and patient outcomes in glioblastomas. J Neuropathol Exp Neurol 2006;65:846-54. Back to cited text no. 39 |
| 40. | Perry A, Aldape KD, George DH, Burger PC. Small cell astroctyoma: An aggressive variant that is clinicopathologically and genetically distinct from anaplastic oligodendrogliomas. Cancer 2004;101:2318-26. Back to cited text no. 40 |
| 41. | Kleihues P, Ohgaki H. Primary and secondary glioblastomas: From concept to clinical diagnosis. Neuro Oncol 1999;1:44-51. Back to cited text no. 41 |
| 42. | Dropcho EJ, Soong SJ. The prognostic impact of prior low grade histology in patients with anaplastic gliomas: A case-control study. Neurology 1996;47:684-90. Back to cited text no. 42 |
| 43. | Moskowitz SI, Jin T, Prayson RA. Role of MIB1 in predicting survival in patients with glioblastomas. J Neurooncol 2006;76:193-200. Back to cited text no. 43 |
| 44. | Lang FF, Miller DC, Kislow M, Newcomb EW. Pathways leading to glioblastomas multiforme: A molecular analysis of genetic alteration in 65 astroctyic tumors. J Neurosurg 1994;81:427-36. Back to cited text no. 44 |
| 45. | von Deimling A, Louis DN, Wiestler OD. Molecular pathways in the formation of gliomas. Glia 1995;15:328-38. Back to cited text no. 45 |
| 46. | Watanabe K, Tachibana O, Sata K, Yonekawa Y, Kleihues P, Ohgaki H. Overexpression of EGF receptor and p53 mutation are mutually exclusive in the evolutions of primary and secondary glioblastomas. Brain Pathol 1996;6:216-23. Back to cited text no. 46 |
| 47. | Kliehues P, Ohgaki H. Primary and secondary glioblastomas: From concept to clinical diagnosis. Neuro Oncol 1999;1:44-51. Back to cited text no. 47 |
| 48. | Riemenschneider MJ, Buschges R, Wolter M, Reifenberger J, Bostrom J, Kraus JA, et al . Amplification and overexpression of the MDM 4 (MDMX) gene from 1q32 in a subset of malignant gliomas without TP53 mutation or MDM 2 amplification. Cancer Res 1999;59:6091-6. Back to cited text no. 48 |
| 49. | Nakamura M, Yonekawa Y, Kleihues P, Ohgaki H. Promoter hypermethylation of the RB1 gene in glioblastomas. Lab Invest 2001;81:77-82. Back to cited text no. 49 |
| 50. | Nakamura M, Yang F, Fujisawa H, Yonekawa Y, Kleihues P, Ohgaki H. Loss of heterozygosity on chromosome 19 in secondary glioblastomas. J Neuropathol Exp Neurol 2000;59:539-43. Back to cited text no. 50 |
| 51. | Fujisawa H, Reis RM, Nakamura M, Colella S, Yonekawa Y, Kleihues P, et al . Loss of heterozygosity on chromosome 10 is more extensive in primary (de novo) than in secondary glioblastomas. Lab Invest 2000;80:65-72. Back to cited text no. 51 |
| 52. | Watanabe K, Sato K, Biernat W, Tachibana O, von Ammon K, Ogata N, et al . Incidence and timing of p53 mutations and during astrocytomas progression in patients with multiple biopsies. Clin Cancer Res 1997;3:523-30. Back to cited text no. 52 |
| 53. | Ohgaki H, Dessen P, Jourde B, Horstmann S, Nishikawa T, Di Patre PL, et al . Genetic pathways to glioblastoma: A population-based study. Cancer Res 2004;64:6892-9. Back to cited text no. 53 |
| 54. | Schmidt MC, Antweiler S, Urban N, Mueller W, Kuklik A, Meyer-Puttlitz B, et al . Impact of genotype and morphology on the prognosis of glioblastoma. J Neuropathol Exp Neurol 2002;61:321-8. Back to cited text no. 54 |
| 55. | Newcomb EW, Cohen H, Lee SR, Bhalla SK, Bloom J, Hayes RL, et al . Survival of patients with glioblastomas multiforme is not influenced by altered expression of p16, p53, EGFR, MDM 2 or Bcl-2 genes. Brain Pathol 1998;8:655-67. Back to cited text no. 55 |
| 56. | Burton EC, Lamborn KR, Forsyth P, Scott J, O'Campo J, Uyehara-Lock J, et al . Aberracne p53, mdm2, and proliferation differ in glioblastomas from long term compared with typical survivors. Clin Cancer Res 2002;8:180-7. Back to cited text no. 56 |
| 57. | Stander M, Peraud A, Leroch B, Kreth FW. Prognostic impact of TP53 mutation status for adult patients with supratentorial World Health prganization grade II astrocytoma or oligoastrcotyoma. Cancer 2004;101:1028-35. Back to cited text no. 57 |
| 58. | Hwang SL, Hong YR, Chai CY, Lin HJ, Hwang SL. Prognostic evaluation in supratentorial astrocytic tumors using p53, epidermal growth factor receptor, c-erbB2 immunostaining. Kaohsiung J Med Sci 1998;14:607-15. Back to cited text no. 58 |
| 59. | Rasheed A, Herndon JE, Stenzel TT, Raetz JG, Kendelhardt J, Friedman HS, et al . Molecular markers of prognosis in astrocytic tumors. Cancer 2002;94:2688-97. Back to cited text no. 59 |
| 60. | Simmons ML, Lamborn KR, Takahashi M, Chen P, Israel MA, Berger MS, et al . Analysis of complex relationships between age, p53, epidermal growth factor receptor, and survival in glioblastoma patients. Cancer Res 2001;61:1122-8. Back to cited text no. 60 |
| 61. | Hurtt MR, Moossy J, Donovan-Peluso M, Locker J. Amplification of epidermal growth factor receptor gene in gliomas: Histopathology and prognosis. J Neuropathol Exp Neurol 1992;51:84-90. Back to cited text no. 61 |
| 62. | Torp SH, Helseth E, Dalen A, Unsgaard G. Relationships between Ki-67 labelling index, amplification odthe epidermal growth factor receptor gene, and prognosis in human glioblastomas. Acta Neurochir (Wein) 1992;117:182-6. Back to cited text no. 62 |
| 63. | Huncharek M, Kupelnick B. Epidermal growth factor receptor gene amplification as a prognostic marker in glioblastoma multiforme: Results of a meta-analysis. Oncol Res 2000;12:107-12. Back to cited text no. 63 |
| 64. | Shinojima N, Tada K, Shirishi S, Kamiryo T, Kochi M, Nakamura H, et al . Prognostic value of epidermal growth factor receptor in patients with glioblastoma multiforme. Cancer Res 2003;63:6962-70. Back to cited text no. 64 |
| 65. | Batchelor TT, Betensky RA, Esposito JM, Pham LD, Dorfman MV, Piscatelli N, et al . Age dependent prognostic effects of genetic alteration in glioblastoma. Clin Cancer Res 2004;10:228-33. Back to cited text no. 65 |
| 66. | Burger PC, Pearl DK, Aldape K, Yates AJ, Scheithauer BW, Passe SM, et al . Small cell architecture histological equivalent of EGFR amplification in glioblastoma multiforme? J Neuropathol Exp Neurol 2001;60:1099-104. Back to cited text no. 66 |
| 67. | Aldape KD, Ballman K, Furth A, Buckner JC, Giannini C, Burger PC, et al . Immunohistochemical detection of EGFRvIII in high malignancy grade astrocytomas and evaluation of prognostic significance. J Neuropathol Exp Neurol 2004;63:700-7. Back to cited text no. 67 |
| 68. | Feldkamp MM, Lala P, Lau N, Roncari L, Guha A. Expression of activated epidermal growth factor receptors, Ras-guanosine triphosphate, and mitogen activated protein kinase in human glioblastoma multiforme specimens. Neurosurgery 1999;45:1442-53. Back to cited text no. 68 |
| 69. | Cianciulli AM, Morace E, Coletta AM, Occhipinti E, Gandolfo GM, Leonardo G, et al . Investigation of genetic alteration associated with development and adverse outcome in patients with astrocytic tumor. J Neurooncol 2000;48:9-101. Back to cited text no. 69 |
| 70. | Perry A, Tonk V, McIntire DD, White CL 3rd. Interphase cytogenetic (in situ hybridization) analysis of astrocytomas using archival, formalin-fixed, paraffin-embedded tissue and nonfluorescent light microscopy. Am J Clin Pathol 1997;108:166-74. Back to cited text no. 70 |
| 71. | Rasheed BK, McLendon RE, Friedman HS, Friedman AH, Fuchs HE, Bigner DD, et al . Chromosome 10 deletion mapping in human gliomas: A common deletion region in 10q25. Oncogene 1995;10:2243-6. Back to cited text no. 71 |
| 72. | Karlbom AE, James CD, Boethius J, Cavenee WK, Collins VP, Nordenskjφld M, et al . Loss of heterozygosity in malignant gliomas involves at least three distinct regions on chromosome 10. Hum Genet 1993;92:169-74. Back to cited text no. 72 |
| 73. | Ichimura K, Schmidt EE, Miyakawa A, Goike HM, Collins VP. Distinct patterns of deletion on 10p and 10q suggest involvement of multiple tumor suppressor genes in the development of astrocytic gliomas of different malignancy grades. Genes Chromosomes Cancer 1998;22:9-15. Back to cited text no. 73 |
| 74. | Burton EC, Lamborn KR, Feuerstein BG, Prados M, Scott J, Forsyth P, et al . Genetic aberrations defined by comparative genomic hybridization distinguish long-term from typical survivors of glioblastoma. Cancer Res 2002;62:6205-10. Back to cited text no. 74 |
| 75. | Arslantas A, Artan S, Oner U, Müslümanoπlu H, Durmaz R, Cosan E, et al . The importance of genomic copy number changes in the prognosis of glioblastoma multiforme. Neurosurg Rev 2004;27:58-64. Back to cited text no. 75 |
| 76. | Schmidt EE, Ichimura K, Goike HM, Moshref A, Liu L, Collins VP. Mutational profile of the PTEN gene in primary human astrocytic tumors and cultivated xenografts. J Neuropathol Exp Neurol 1999;58:1170-83. Back to cited text no. 76 |
| 77. | Zhou XP, Li YJ, Hoang-Xuan K, Laurent-Puig P, Mokhtari K, Longy M, et al . Mutational analysis of the PTEN gene in gliomas: molecular and pathological correlations. Int J Cancer 1999;84:150-4. Back to cited text no. 77 |
| 78. | Balesaria S, Brock C, Bower M, Clark J, Nicholson SK, Lewis P, et al . Loss of chromosome 10 is an independent prognostic factor in high-grade gliomas. Br J Cancer 1999;81:1371-7. Back to cited text no. 78 |
| 79. | Fults D, Pedone CA, Thompson GE, Uchiyama CM, Gumpper KL, Iliev D, et al . Microsatellite deletion mapping on chromosome 10q and mutation analysis of MMAC1, FAS, and MXI1 in human glioblastoma multiforme. Int J Oncol 1998;12:905-10. Back to cited text no. 79 |
| 80. | Bδcklund LM, Nilsson BR, Goike HM, Schmidt EE, Liu L, Ichimura K, et al . Short postoperative survival for glioblastoma patients with a dysfunctional Rb1 pathway in combination with no wild-type PTEN. Clin Cancer Res 2003;9:4151-8. Back to cited text no. 80 |
| 81. | Terada K, Tamiya T, Daido S, Kambara H, Tanaka H, Ono Y, et al . Prognostic value of loss of heterozygosity around three candidate tumor suppressor genes on chromosome 10q in astrocytomas J Neurooncol 2002;58:107-14. Back to cited text no. 81 |
| 82. | Sano T, Lin H, Chen X, Langford LA, Koul D, Bondy ML, et al . Differential expression of MMAC/PTEN in glioblastoma multiforme: Relationship to localization and prognosis. Cancer Res 1999;59:1820-4. Back to cited text no. 82 |
| 83. | Bello MJ, Alonso ME, Amiρoso C, Anselmo NP, Arjona D, Gonzalez-Gomez P, et al . Hypermethylation of the DNA repair gene MGMT: Association with TP53 G:C to A:T transitions in a series of 469 nervous system tumors. Mutat Res 2004;554:23-32. Back to cited text no. 83 |
| 84. | Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, et al . MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med 2005;352:997-1003. Back to cited text no. 84 |
| 85. | Kamiryo T, Tada K, Shiraishi S, Shinojima N, Kochi M, Ushio Y. Correlation between promoter hypermethylation of the O6-methylguanine-deoxyribonucleic acid methyltransferase gene and prognosis in patients with high-grade astrocytic tumors treated with surgery, radiotherapy, and 1-(4-amino-2-methyl-5-pyrimidinyl)methyl-3-(2-chloroethyl)-3-nitrosourea-based chemotherapy. Neurosurgery 2004;54:349-57. Back to cited text no. 85 |
| 86. | Nakamura M, Watanabe T, Yonekawa Y, Kleihues P, Ohgaki H. Promoter methylation of the DNA repair gene MGMT in astrocytomas is frequently associated with G:C --> A:T mutations of the TP53 tumor suppressor gene. Carcinogenesis 2001;22:1715-9. Back to cited text no. 86 |
| 87. | Sarkar C, Karak AK, Nath N, Sharma MC, Mahapatra AK, Chattopadhyay P, et al . Apoptosis and proliferation: Correlation with p53 in astrocytic tumours. J Neurooncol 2005;73:93-100. Back to cited text no. 87 |
| 88. | Sarkar C, Sinha S, Sharma MC, Kumar R, Mehta VS. Supratentorial glioblastoma in adults: Identification of subsets and their clinical correlation. Brain Tumor Pathol 2004;21:7-12. Back to cited text no. 88 |
| 89. | Sharma MC, Ralte AM, Gaekwad S, Santosh V, Shankar SK, Sarkar C. Subependymal giant cell astrocytoma: A clinicopathological study of 23 cases with special emphasis on histogenesis. Pathol Oncol Res 2004;10:219-24. Back to cited text no. 89 |
| 90. | Sarkar C, Ralte AM, Sharma MC, Mehta VS. Recurrent astrocytic tumours: A study of p53 immunoreactivity and malignant progression. Br J Neurosurg 2002;16:335-42. Back to cited text no. 90 |
| 91. | Sarkar C, Rathore A, Chattopadhyaya P, Mahapatra AK, Sinha S. Role of 17p13.3 chromosomal region in determining p53 protein immunopositivity in human astrocytic tumors. Pathology 2000;32:84-8. Back to cited text no. 91 |
| 92. | Misra A, Chattopadhyay P, Dinda AK, Sarkar C, Mahapatra AK, Hasnain SE, et al . Extensive intra-tumor heterogeneity in primary human glial tumors as a result of locus non-specific genomic alterations. J Neurooncol 2000;48:1-12. Back to cited text no. 92 |
| 93. | Rathore A, Kamarajan P, Mathur M, Sinha S, Sarkar C. Simultaneous alterations of retinoblastoma and p53 protein expression in astrocytic tumors. Pathol Oncol Res 1999;5:21-7. Back to cited text no. 93 |
| 94. | Ghosh M, Dinda A, Chattopadhyay P, Sarkar C, Bhatia S, Sinha S. Rearranged p53 gene with loss of normal allele in a low-grade nonrecurrent glioma. Cancer Genet Cytogenet 1994;78:68-71. Back to cited text no. 94 |
| 95. | Banerjee M, Dinda AK, Sinha S, Sarkar C, Mathur M. C-MYC oncogene expression and cell proliferation in mixed oligo-astrocytoma. Int J Cancer 1996;65:730-3. Back to cited text no. 95 |
| 96. | Chattopadhyay P, Banerjee M, Sarkar C, Mathur M, Mohapatra AK, Sinha S. Infrequent alteration of the c-myc gene in human glial tumours associated with increased numbers of c-myc positive cells. Oncogene 1995;11:2711-4. Back to cited text no. 96 |
| 97. | Chattopadhyay P, Rathore A, Mathur M, Sarkar C, Mahapatra AK, Sinha S. Loss of heterozygosity of a locus on 17p13.3, independent of p53, is associated with higher grades of astrocytic tumours. Oncogene 1997;15:871-4. Back to cited text no. 97 |
| 98. | Nayak A, Ralte AM, Sharma MC, Singh VP, Mahapatra AK, Mehta VS, et al . p53 protein alterations in adult astrocytic tumors and oligodendrogliomas. Neurol India 2004;52:228-32. Back to cited text no. 98 [PUBMED]  |
| 99. | Reifenberger G, Kros JM, Louis DN, Collins VP. Oligodendroglioma. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, editors. World Health Organization classification of tumors of the central nervous system. Lyon: IARC; 2007. p. 54-9. Back to cited text no. 99 |
| 100. | Ohgaki H, Kleihues P. Population based studies on incidence, survival rates, and genetic alteration in astrocytic and oligodendroglial gliomas. J Neuropathol Exp Neurol 2005;64:479-89. Back to cited text no. 100 |
| 101. | Felsberg J, Erkwoh A, Sabel MC, Kirsch L, Fimmers R, Blaschke B, et al . Oligodendroglial tumors: refinement of candidate regions on chromosome arm 1p and correlation of 1p/19q status with survival. Brain Pathol 2004;14:121-30. Back to cited text no. 101 |
| 102. | Giannini C, Scheithauer BW, Weaver AL, Burger PC, Kros JM, Mork S, et al . Oligodendrogliomas: Reproducibility and prognostic value of histologic diagnosis and grading. J Neuropathol Exp Neurol 2001;60:248-62. Back to cited text no. 102 |
| 103. | Lebrun C, Fontaine D, Ramaioli A, Vandenbos F, Chanalet S, Lonjon M, et al . Long-term outcome of oligodendrogliomas. Neurology 2004;62:1783-7. Back to cited text no. 103 |
| 104. | Reifenberger G, Kros JM, Louis DN, Collins VP. Anaplastic Oligodendroglioma. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, editors. World Health Organization classification of tumors of the central nervous system. Lyon: IARC; 2007. p. 60-3. Back to cited text no. 104 |
| 105. | Kros JM, Van Eden CG, Stefanko SZ, Waayer-Van Batenburg M, van der Kwast TH. Prognostic implications of glial fibrillary acidic protein containing cell types in oligodendrogliomas. Cancer 1990;66:1204-12. Back to cited text no. 105 |
| 106. | Reifenberger G, Reifenberger J, Lui L, et al . Molecualr genetics of oligodendroglial tumors. In: Nagai M, editors. Brain Research and Therapy. Tokyo, Japan: Springer-Verlag; 1996. p. 187-209. Back to cited text no. 106 |
| 107. | Reifenberger J, Ring GU, Gies U, Cobbers L, Oberstrass J, An HX, et al . Analysis of p53 mutation and epidermal growth factor receptor amplification in recurrent gliomas with malignant progression. J Neuropathol Exp Neurol 1996;55:822-31. Back to cited text no. 107 |
| 108. | Reifenberger J, Reifenberger G, Liu L, James CD, Wechsler W, Collins VP. Molecular genetic analysis of oligodendroglial tumors shows preferential allelic deletions on 19q and 1p. Am J Pathol 1994;145:1175-90. Back to cited text no. 108 |
| 109. | Maintz D, Fiedler K, Koopmann J, Rollbrocker B, Nechev S, Lenartz D, et al . Molecular genetic evidence for subtypes of oligoastrocytomas. J Neuropathol Exp Neurol 1997;56:1098-104. Back to cited text no. 109 |
| 110. | Bello MJ, Vaquero J, de Campos JM, Kusak ME, Sarasa JL, Saez-Castresana J, et al . Molecular analysis of chromosome 1 abnormalities in human gliomas reveals frequent loss of 1p in oligodendroglial tumors. Int J Cancer 1994;57:172-5. Back to cited text no. 110 |
| 111. | Bello MJ, Leone PE, Vaquero J, de Campos JM, Kusak ME, Sarasa JL, et al . Allelic loss at 1p and 19q frequently occurs in association and may represent early oncogenic events in oligodendroglial tumors. Int J Cancer 1995;64:207-10. Back to cited text no. 111 |
| 112. | Kraus JA, Koopmann J, Kaskel P, Maintz D, Brandner S, Schramm J, et al . Shared allelic losses on chromosomes 1p and 19q suggest a common origin of oligodendroglioma and oligoastrocytoma. J Neuropathol Exp Neurol 1995;54:91-5. Back to cited text no. 112 |
| 113. | von Deimling A, Louis DN, von Ammon K, Petersen I, Wiestler OD, Seizinger BR. Evidence for a tumor suppressor gene on chromosome 19q associated with human astrocytomas, oligodendrogliomas, and mixed gliomas. Cancer Res 1992;52:4277-9. Back to cited text no. 113 |
| 114. | Bigner SH, Rasheed BK, Wiltshire R, McLendon RE. Morphological and molecular genetic aspects of oligodendroglial neoplasms. Neuro Oncol 1999;1:52-60. Back to cited text no. 114 |
| 115. | Jeuken JW, von Deimling A, Wesseling P. Molecular pathogenesis of oligodendroglial tumors. J Neurooncol 2004;70:161-81. Back to cited text no. 115 |
| 116. | Okamoto Y, Di Patre PL, Burkhard C, Horstmann S, Jourde B, Fahey M, et al . Population-based study on incidence, survival rates, and genetic alterations of low-grade diffuse astrocytomas and oligodendrogliomas. Acta Neuropathol 2004;108:49-56. Back to cited text no. 116 |
| 117. | van den Bent MJ, Taphoorn MJ, Brandes AA, Menten J, Stupp R, Frenay M, et al . Phase II study of first-line chemotherapy with temozolomide in recurrent oligodendroglial tumors: the European Organization for Research and Treatment of Cancer Brain Tumor Group Study 26971. J Clin Oncol 2003;21:2525-8. Back to cited text no. 117 |
| 118. | Kreiger PA, Okada Y, Simon S, Rorke LB, Louis DN, Golden JA. Losses of chromosomes 1p and 19q are rare in pediatric oligodendrogliomas. Acta Neuropathol 2005;109:387-92. Back to cited text no. 118 |
| 119. | Smith JS, Perry A, Borell TJ, Lee HK, O'Fallon J, Hosek SM, et al . Alterations of chromosome arms 1p and 19q as predictors of survival in oligodendrogliomas, astrocytomas, and mixed oligoastrocytomas. J Clin Oncol 2000;18:636-45. Back to cited text no. 119 |
| 120. | Reifenberger G, Louis DN. Oligodendroglioma: Toward molecular definitions in diagnostic neuro-oncology. J Neuropathol Exp Neurol 2003;62:111-26. Back to cited text no. 120 |
| 121. | Fuller CE, Perry A. Molecular diagnostics in central nervous system tumors. Adv Anat Pathol 2005;12:180-94. Back to cited text no. 121 |
| 122. | Griffin CA, Burger P, Morsberger L, Yonescu R, Swierczynski S, Weingart JD, et al . Identification of der(1;19)(q10;p10) in five oligodendrogliomas suggests mechanism of concurrent 1p and 19q loss. J Neuropathol Exp Neurol 2006;65:988-94. Back to cited text no. 122 |
| 123. | Jenkins RB, Blair H, Ballman KV, Giannini C, Arusell RM, Law M, et al . A t(1;19)(q10;p10) mediates the combined deletions of 1p and 19q and predicts a better prognosis of patients with oligodendroglioma. Cancer Res 2006;66:9852-61. Back to cited text no. 123 |
| 124. | Jaeckle KA, Ballman KV, Rao RD, Jenkins RB, Buckner JC. Current strategies in treatment of oligodendroglioma: Evolution of molecular signatures of response. J Clin Oncol 2006;24:1246-52. Back to cited text no. 124 |
| 125. | Ueki K. Oligodendroglioma: Impact of molecular biology on its definition, diagnosis and management. Neuropathology 2005;25:247-53. Back to cited text no. 125 |
| 126. | Hartmann C, Mueller W, von Deimling A. Pathology and molecular genetics of oligodendroglial tumors. J Mol Med 2004;82:638-55. Back to cited text no. 126 |
| 127. | Kelley TW, Tubbs RR, Prayson RA. Molecular diagnostic techniques for the clinical evaluation of gliomas. Diagn Mol Pathol 2005;14:1-8. Back to cited text no. 127 |
| 128. | Johnson MD, Vnencak-Jones CL, Toms SA, Moots PM, Weil R. Allelic losses in oligodendroglial and oligodendroglioma-like neoplasms: Analysis using microsatellite repeats and polymerase chain reaction. Arch Pathol Lab Med 2003;127:1573-9. Back to cited text no. 128 |
| 129. | Fallon KB, Palmer CA, Roth KA, Nabors LB, Wang W, Carpenter M, et al . Prognostic value of 1p, 19q, 9p, 10q, and EGFR-FISH analyses in recurrent oligodendrogliomas. J Neuropathol Exp Neurol 2004;63:314-22. Back to cited text no. 129 |
| 130. | Buckner JC, Ballman KV, Scheithauer RM. NCCTG 94-72-53: Diagnostic and prognostic significance of 1p and 19q deletions in patients with low grade oligodendroglioma and astrocytomas. J Clin Oncol 2005;23:114s. Back to cited text no. 130 |
| 131. | Ino Y, Betensky RA, Zlatescu MC, Sasaki H, Macdonald DR, Stemmer-Rachamimov AO, et al . Molecular subtypes of anaplastic oligodendroglioma: Implications for patient management at diagnosis. Clin Cancer Res 2001;7:839-45. Back to cited text no. 131 |
| 132. | Hashimoto N, Murakami M, Takahashi Y, Fujimoto M, Inazawa J, Mineura K. Correlation between genetic alteration and long-term clinical outcome of patients with oligodendroglial tumors, with identification of a consistent region of deletion on chromosome arm 1p. Cancer 2003;97:2254-61. Back to cited text no. 132 |
| 133. | Buckner JC, Gesme D Jr, O'Fallon JR, Hammack JE, Stafford S, Brown PD, et al . Phase II trial of procarbazine, lomustine, and vincristine as initial therapy for patients with low-grade oligodendroglioma or oligoastrocytoma: Efficacy and associations with chromosomal abnormalities. J Clin Oncol 2003;21:251-5. Back to cited text no. 133 |
| 134. | Chahlavi A, Kanner A, Peereboom D, Staugaitis SM, Elson P, Barnett G. Impact of chromosome 1p status in response of oligodendroglioma to temozolomide: Preliminary results. J Neurooncol 2003;61:267-73. Back to cited text no. 134 |
| 135. | Thiessen B, Maguire JA, McNeil K, Huntsman D, Martin MA, Horsman D. Loss of heterozygosity for loci on chromosome arms 1p and 10q in oligodendroglial tumors: Relationship to outcome and chemosensitivity. J Neurooncol 2003;64:271-8. Back to cited text no. 135 |
| 136. | van den Bent MJ, Looijenga LH, Langenberg K, Dinjens W, Graveland W, Uytdewilligen L, et al . Chromosomal anomalies in oligodendroglial tumors are correlated with clinical features. Cancer 2003;97:1276-84. Back to cited text no. 136 |
| 137. | Cairncross G, Seiferheld W, Shaw E. An intergroup randomized controlled clinical trial (RCT) of chemotherapy plus radiotherapy (RT) versus RT alone for pure and mixed anaplastic oligodendrolgioma: initial report of RTOG 9402. J Clin Oncol 2004;22:107s. Back to cited text no. 137 |
| 138. | Cairncross G, Seiferheld W, Shaw E. An intergroup randomized controlled clinical trial (RCT) of chemotherapy plus radiotherapy (RT) versus RT alone for pure and mixed anaplastic oligodendrolgioma: initial report of RTOG 9402. Presented at the society for Neuro-Oncology 9th Annual Scientific Meeting, Toronto, Canada, Nov 18-21, 2004. Back to cited text no. 138 |
| 139. | van den Bent MJ, Chinot O, Boogerd W, Bravo Marques J, Taphoorn MJ, Kros JM, et al . Second-line chemotherapy with temozolomide in recurrent oligodendroglioma after PCV (procarbazine, lomustine and vincristine) chemotherapy: EORTC Brain Tumor Group phase II study 26972. Ann Oncol 2003;14:599-602. Back to cited text no. 139 |
| 140. | Kros JM, Gorlia T, Kouwenhoven MC, Zheng PP, Collins VP, Figarella-Branger D, et al . Panel review of anaplastic oligodendroglioma from European Organization for Research and Treatment of Cancer Trial 26951: Assessment of consensus in diagnosis, influence of 1p/19q loss, and correlations with outcome. J Neuropathol Exp Neurol 2007;66:545-51. Back to cited text no. 140 |
| 141. | Giannini C, Burger PC, Berkey BA, Cairncross JG, Jenkins RB, Mehta M, et al . Anaplastic Oligodendroglial Tumors: Refining the Correlation among Histopathology, 1p 19q Deletion and Clinical Outcome in Intergroup Radiation Therapy Oncology Group Trial 9402. Brain Pathol 2008;18:360-9. Back to cited text no. 141 |
| 142. | Aldape K, Burger PC, Perry A. Clinicopathologic aspects of 1p/19q loss and the diagnosis of oligodendrogliomas. Arch Pathol Lab Med 2007;131:242-51. Back to cited text no. 142 |
| 143. | Sanson M, Leuraud P, Aguirre-Cruz L, He J, Marie Y, Cartalat-Carel S, et al . Analysis of loss of chromosome 10q, DMBT1 homozygous deletions, and PTEN mutations in oligodendrogliomas. J Neurosurg 2002;97:1397-401. Back to cited text no. 143 |
| 144. | Bissola L, Eoli M, Pollo B, Merciai BM, Silvani A, Salsano E, et al . Association of chromosome 10 losses and negative prognosis in oligoastrocytomas. Ann Neurol 2002;52:842-5. Back to cited text no. 144 |
| 145. | Jeuken JW, Sprenger SH, Vermeer H, Kappelle AC, Boerman RH, Wesseling P. Chromosomal imbalances in primary oligodendroglial tumors and their recurrences: Clues about malignant progression detected using comparative genomic hybridization. J Neurosurg 2002;96:559-64. Back to cited text no. 145 |
| 146. | Ueki K, Nishikawa R, Nakazato Y, Hirose T, Hirato J, Funada N, et al . Correlation of histology and molecular genetic analysis of 1p, 19q, 10q, TP53, EGFR, CDK4, and CDKN2A in 91 astrocytic and oligodendroglial tumors. Clin Cancer Res 2002;8:196-201. Back to cited text no. 146 |
| 147. | Duerr EM, Rollbrocker B, Hayashi Y, Peters N, Meyer-Puttlitz B, Louis DN, et al . PTEN mutations in gliomas and glioneuronal tumors. Oncogene 1998;16:2259-64. Back to cited text no. 147 |
| 148. | Jeuken JW, Nelen MR, Vermeer H, van Staveren WC, Kremer H, van Overbeeke JJ, et al . PTEN mutation analysis in two genetic subtypes of high-grade oligodendroglial tumors: PTEN is only occasionally mutated in one of the two genetic subtypes. Cancer Genet Cytogenet 2000;119:42-7 Back to cited text no. 148 |
| 149. | Maier D, Comparone D, Taylor E, Zhang Z, Gratzl O, Van Meir EG, et al . New deletion in low-grade oligodendroglioma at the glioblastoma suppressor locus on chromosome 10q25-26. Oncogene 1997;15:997-1000. Back to cited text no. 149 |
| 150. | Sasaki H, Zlatescu MC, Betensky RA, Ino Y, Cairncross JG, Louis DN. PTEN is a target of chromosome 10q loss in anaplastic oligodendrogliomas and PTEN alterations are associated with poor prognosis. Am J Pathol 2001;159:359-67. Back to cited text no. 150 |
| 151. | Bello MJ, de Campos JM, Vaquero J, Kusak ME, Sarasa JL, Pestaρa A, et al . Molecular and cytogenetic analysis of chromosome 9 deletions in 75 malignant gliomas. Genes Chromosomes Cancer 1994;9:33-41. Back to cited text no. 151 |
| 152. | Bigner SH, Matthews MR, Rasheed BK, Wiltshire RN, Friedman HS, Friedman AH, et al . Molecular genetics aspects of oligodendrogliomas including analysis by comparative genomic hybridization. Am J Pathol 1999;155:375-86. Back to cited text no. 152 |
| 153. | Cairncross JG, Ueki K, Zlatescu MC, Lisle DK, Finkelstein DM, Hammond RR, et al . Specific genetic predictors of chemotherapeutic response and survival in patients with anaplastic oligodendrogliomas. J Natl Cancer Inst 1998;90:1473-9. Back to cited text no. 153 |
| 154. | Law ME, Templeton KL, Kitange G, Smith J, Misra A, Feuerstein BG, et al . Molecular cytogenetic analysis of chromosomes 1 and 19 in glioma cell lines. Cancer Genet Cytogenet 2005;160:1-14. Back to cited text no. 154 |
| 155. | Bortolotto S, Chiadò-Piat L, Cavalla P, Bosone I, Chiò A, Mauro A, et al . CDKN2A/p16 inactivation in the prognosis of oligodendrogliomas. Int J Cancer 2000;88:554-7. Back to cited text no. 155 |
| 156. | Miettinen H, Kononen J, Sallinen P, Alho H, Helen P, Helin H, et al . CDKN2/p16 predicts survival in oligodendrogliomas: Comparison with astrocytomas. J Neurooncol 1999;41:205-11. Back to cited text no. 156 |
| 157. | Alonso ME, Bello MJ, Gonzalez-Gomez P, Arjona D, Lomas J, de Campos JM, et al . Aberrant promoter methylation of multiple genes in oligodendrogliomas and ependymomas. Cancer Genet Cytogenet 2003;144:134-42. Back to cited text no. 157 |
| 158. | Dong SM, Pang JC, Poon WS, Hu J, To KF, Chang AR, et al . Concurrent hypermethylation of multiple genes is associated with grade of oligodendroglial tumors. J Neuropathol Exp Neurol 2001;60:808-16. Back to cited text no. 158 |
| 159. | von Deimling A, Reifenberger G, Kros JM, Louis DN, Collins VP. Oligoastrocytoma. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, editors. World Health Organization classification of tumors of the central nervous system. Lyon: IARC; 2007. p. 63-7. Back to cited text no. 159 |
| 160. | Shaw EG, Scheithauer BW, O'Fallon JR, Davis DH. Mixed oligoastrocytomas: A survival and prognostic factor analysis. Neurosurgery 1994;34:577-82. Back to cited text no. 160 |
| 161. | Mueller W, Hartmann C, Hoffmann A, Lanksch W, Kiwit J, Tonn J, et al . Genetic signature of oligoastrocytomas correlates with tumor location and denotes distinct molecular subsets. Am J Pathol 2002;161:313-9. Back to cited text no. 161 |
| 162. | Beckmann MJ, Prayson RA. A clinicopathologic study of 30 cases of oligoastrocytoma including p53 immunohistochemistry. Pathology 1997;29:159-64. Back to cited text no. 162 |
| 163. | Shimada y, Kubo O, Tajika Y, Hiyama H, Atuji S, Takakura K. Clinicopathological study of mixed oligoastrocytoma. In: Nagai M, editor. Brain tumor research and therapy. Tokyo: Springer-Verlag; 1997. p. 51-60. Back to cited text no. 163 |
| 164. | Miller CR, Dunham CP, Scheithauer BW, Perry A. Significance of necrosis in grading of oligodendroglial neoplasms: A clinicopathologic and genetic study of newly diagnosed high-grade gliomas. J Clin Oncol 2006;24:5419-26. Back to cited text no. 164 |
| 165. | He J, Mokhtari K, Sanson M, Marie Y, Kujas M, Huguet S, et al . Glioblastomas with an oligodendroglial component: A pathological and molecular study. J Neuropathol Exp Neurol 2001;60:863-71. Back to cited text no. 165 |
| 166. | Eoli M, Bissola L, Bruzzone MG, Pollo B, Maccagnano C, De Simone T, et al . Reclassification of oligoastrocytomas by loss of heterozygosity studies. Int J Cancer 2006;119:84-90. Back to cited text no. 166 |
| 167. | Hoang-Xuan K, Capelle L, Kujas M, Taillibert S, Duffau H, Lejeune J, et al . Temozolomide as initial treatment for adults with low-grade oligodendrogliomas or oligoastrocytomas and correlation with chromosome 1p deletions. J Clin Oncol 2004;22:3133-8. Back to cited text no. 167 |
Copyright 2009 - Indian Journal of Cancer
The following images related to this document are available:
Photo images
[cn09023f2.jpg]
[cn09023f1.jpg]
[cn09023f3.jpg]
[cn09023t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}