 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
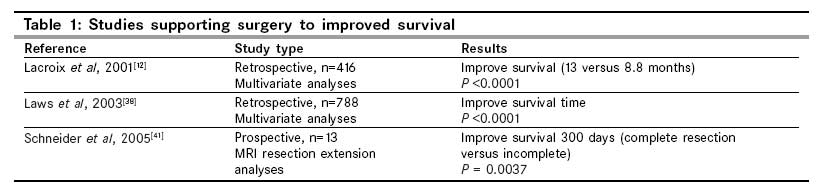
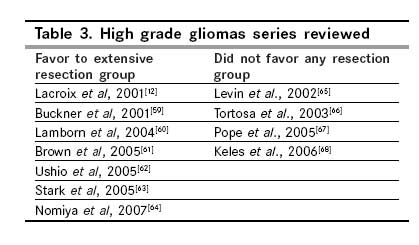
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 120-126 Symposium The role of surgery in the management of intracranial gliomas: Current concepts Nunez OM, Seol HJ, Rutka JT Arthur and Sonia Labatt Brain Tumor Research Centre, Hospital for Sick Children, Toronto, Canada Code Number: cn09024 Abstract The role of surgery in the management of human gliomas has been controversial. The results from numerous neurosurgical series are inconsistent. The current adjuvant therapies have facilitated treatment of patients, and have rendered neurosurgical removal without morbidity or mortality more commonplace than ever before. Here, we investigated the role of surgery in the management of adults with low- and high-grade gliomas. Even though there is substantial evidence which claims that surgery per se has a role to play in extending patient survival, there is a paucity of randomized clinical trials on this subject, and little in the way of Class II data to support these claims. However, this should not divert patients away from surgery, because there may be additional benefits from a concerted effort to remove a tumor completely. At the present time, it seems best that clinicians continue to individualize patient treatment based on a myriad of factors that relate to the patient, the patient's tumor, and the known biology of the disease.Keywords: Adjuvant therapies, advance in neurosurgery, extension of resection, glioma, surgery, survival Introduction Gliomas are the most common primary tumors of the central nervous system (CNS), representing approximately 50% of the newly diagnosed brain tumors. According to the 2007 World Health Organization (WHO) classification, there are many different types of gliomas: Astrocytic, oligodendroglial, mixed oligoastrocytic tumors, ependymomas, and choroid plexus tumors. [1] Of these, astrocytomas, have the highest incidence. [2],[3] The classification of human gliomas includes both histological features such as nuclear atypia, mitotic figures, microvascular proliferation and focal pseudopalisading necrosis, [4] and the separation into four grades (I-IV), with low-grade tumors being grades I and II, and high-grades tumors, grades III (anaplastic tumors) and IV (glioblastoma). This grading system has proved most accurate in predicting the clinical outcome. The goals of glioma surgery are: To obtain a tissue sample for diagnosis; to decrease tumor mass; to relieve neurological symptoms; and to provide time so that other treatments, such as, cranial irradiation and chemotherapy can be performed. The biology, clinical , and outcome are different for low- and high-grade gliomas in adults, but the treatments for these neoplasms are somewhat similar. Cranial irradiation after surgical debulking has been a mainstay of therapy in a majority of cases. Despite the advances in the care of patients with gliomas these past 15 years, surgery still plays an important and decisive role in the management of these patients. Here we discuss the current concepts on gliomas in adults, including natural history studies, surgical intervention, biopsy versus resection, impact of the extent of resection, impact of adjuvant therapies, molecular tools, and some recent advanced techniques, with which surgery has become more safe and predictable. Low Grade Gliomas Low-grade gliomas (LGGs) are typically classified as WHO grade I and II neoplasms and include pilocytic astrocytomas, diffuse astrocytomas, oligodendrogliomas, ependymomas, and mixed gliomas. However, LGGs are understandably a heterogeneous group which is clinically and molecularly diverse. Therefore, we will limit our discussion here to WHO grade II diffuse astrocytomas, oligodendrogliomas, and mixed gliomas, which share similar characteristics of clinical manifestations, with invasive and malignant potential. [5] Low-grade gliomas are generally relatively slow-growing primary brain tumors. However, they may exhibit a diverse clinical behavior. Many patients present with only seizures and are neurologically stable for a prolonged period of time. However, others may show functional deficits or signs of increased intracranial pressure. The benefits of various interventions including radiotherapy, chemotherapy, and surgical resection, have been described, but the role of the extent of surgery remains unclear. At this time, there is no consensus on the policy of surgical treatment for LGG. Either biopsy, subtotal or total excision can be undertaken, given the tumor′s location, the patient′s age, and the safety of performing surgery. High Grade Gliomas High Grade Gliomas (HGGs) are also called "malignant gliomas." These tumors represent the most common primary brain tumor in the adult population. For HGGs, the incidence is 5 to 10 per 100,000 persons, and the median survival is about two to three years for WHO grade III and ten 10 to twelve 12 months for grades IV. [6],[7] The term glioblastoma multiforme (GBM), was introduced by Mallory in 1914, and is still used at the present time to depict the most malignant of intracranial glial tumors. [8] Some controversies still exist regarding the surgical treatment of HGGs. For the last 30 years, the neurosurgery community has debated the issue of the extent of resection. In actuality, aggressive resections began when Walter Dandy performed the first hemispherectomy in 1928, in order to achieve the "total" removal of an intracranial glioma. [9] Despite this very aggressive approach, all patients succumbed from the disease retained in the hemisphere. This illustrates the highly invasive and infiltrative potential of GBMs. Total resection is impossible in most cases, especially when tumors are situated in eloquent areas. [10],[11] Today, even with a near-total resection, the survival time of most patients hovers around 12 months. In some series, gross total resection of over 98% of the tumor, followed by chemotherapy and radiotherapy, may offer some improvement in the overall survival. [12],[13],[14],[15],[16],[17],[18] Neurosurgical Adjuncts to Overcome Morbidity Historically, intraoperative electrocortical stimulation has proven to be the gold standard in glioma surgery for the avoidance of postoperative neurological deterioration. Advances in brain mapping techniques have gradually emerged and are part of the clinician′s armamentarium to supplement clinical and radiological findings for preoperative planning. Preoperative functional magnetic resonance imaging (fMRI) enables the definition of the cortical functional areas and their proximity to the tumor tissue, and can provide global preoperative information about the resectability of the tumor without causing neurological deterioration. [19] In addition, magnetic source imaging (MSI) with magnetoencephalography (MEG) provides a presurgical map, which clearly identifies the functional brain areas. As with fMRI, MSI correlates well with intraoperative cortical stimulation. [20] Diffusion tensor imaging (DTI) is a noninvasive method of studying the structure of human neuronal fibers and tracts. It captures the local water diffusion characteristics of tissues and models the 3D distribution of Brownian motion as the diffusion tensor. [21] It is beneficial to delineate margins of the glioma because DTI is sensitive to the directional diffusion of water along white matter tracks. [22] Kamada et al, [23] suggested that preoperative cortical and subcortical maps generated by a combination of functional MRI, MSI, and DTI are predictive and can be confirmed by intraoperative cortical and subcortical stimulation mapping. Intraoperatively, cortical or subcortical stimulation can be used to aggressively remove gliomas and avoid injury to long tract fiber pathways such as the corticospinal tract. Several retrospective series have shown that these techniques allow for aggressive neurosurgery for LGGs, within eloquent areas, and are associated with a decrease in the risk of neurological sequelae after surgery, and to an improvement in the extent of resection, with an impact on survival. [24],[25],[26] Currently, frameless stereotactic neuronavigation is very helpful in approaching deep seated tumors and voiding errors in trajectory during surgery. However, neuronavigation is known to be associated with intraoperative brain shifts, which render the device somewhat problematic. [27] To solve the problem of brain shifts, intraoperative MRI has been invented to allow for continuous updating of imaging data, with compensation for the brain shift. Several retrospective articles have shown an increase in the extent of resection and survival time when intraoperative MRI is used. [28],[29] As a result of advances in surgical techniques including pre- and intraoperative adjuncts and devices, more extensive surgery is now possible. In addition, greater resection of a tumor leads to less chance of sampling error, which can be problematic when biopsies are performed. Adjuvant therapies While surgery alone is often used to treat grade I gliomas, including pilocytic astrocytomas, all the other grades will require some form of combination therapy including radiotherapy (RT), chemotherapy or both. The identification of molecular markers, such as, the enzyme methylguanine methyltransferase (MGMT), epigenetically silenced in some tumors by methylation of the CpG island in the promoter region, has now been shown to be a predictive marker for treatment response to the chemotherapeutic agent, temozolomide (TMZ). Other molecular markers in clinical use today include the loss of heterozygosity on chromosomes 1p and 19q. If a patient with an anaplastic oligodendroglioma has this molecular phenotype, the overall survival is significantly better following treatment with chemotherapy. As more than 30% of GBM patients exhibit epidermal growth factor receptor (EGFR) amplification on their tumors, treatment with EGFR inhibitors, such as, gefitinib and erlotinib has been introduced. Currently, there is a phase II study which uses Cilentigide, an integrin inhibitor, for GBM. Other molecular treatments which are being examined are the use of an oral anti-vascular endothelial receptor (VEGF) tyrosine kinase inhibitor, and the use of wafers impregnated with chemotherapy, such as carmustine, to treat some patients after neurosurgical resection (GLIADEL). Is Surgical Intervention Beneficial? A ′wait-and-see′ policy has been considered for patients harboring typical LGG, especially with minimal symptoms or controllable seizures. This strategy may give some patients an overall improved quality of life (QOL) for some duration, because they are not exposed to the possible morbidity and mortality related to surgery. However, Scott et al, has shown that grading gliomas on the basis of imaging characteristics alone underestimated the degree of malignancy in one-third of the cases. [30] They advocated procuring of tissue for diagnosis whenever it was deemed safe and possible. Moreover, even though contrast enhancement on MRI has long been believed to be a sign of malignancy, recent studies have suggested that contrast enhancement may occur in up to 40-60% of LGGs. [6],[31] In the future, additional information may be gleaned through magnetic resonance spectroscopy and perfusion-weighted imaging, but at the moment, these techniques are still associated with significant error rates. [32],[33] As well as a possible error in diagnosis, the expectant management of patients with LGGs can bring on other risks, such as, malignant degeneration, subsequent tumor growth, and irreversible neurological deficit. However, despite these theoretical risks, several retrospective series revealed that the timing of surgical intervention did not affect the rates of malignant transformation, overall survival, or QOL. [34] While there is still some debate on this matter, procuring a tissue diagnosis by surgical intervention may be a reasonable first stem in the management of LGG patients, irrespective of their site of origin. Standard therapy for patients with progressive, symptomatic LGG remains fractionated radiotherapy (RT) after surgical intervention, although several clinical trials using chemotherapy, such as, TMZ before or after RT in LGG, have recently shown some effect. [35] For HGGs the policy of ′wait-and-see′ has never been considered, even for tumors located in deep or eloquent areas. For GBM patients with multifocal disease, the use of biopsy-only has been reported with poor survival time in the pre-temozolomide era, [36] with a series reporting around 30% one-year survival, with biopsy alone. [10],[37],[38],[39],[40] A small prospective series by Schneider et al , [41] [Table - 1] showed a correlation between resection and survival time. Nevertheless, physicians still considering aggressive surgical options for patients with HGGs need to take into account the importance of relief of the symptoms and the need to get patients to their adjuvant therapies to improve survival and not be hindered by neurological morbidity. We summarize only three of the series reported after 2000, showing some significant improvement in survival with aggressive resection of HGGs [Table - 1]. The Extent of Surgical Resection Historically, biopsy has been used for tumors located adjacent to or deep within eloquent cortices. While stereotactic biopsy is chosen for patients with deep-seated lesions, resection is reserved for those with superficial lesions. Sometimes, brain mapping before surgery is useful, especially in the eloquent cortex. On the other hand, craniotomy and resection have an advantage for patients with significant mass effect, which results in increased intracranial pressure or neurological deficit and for those with symptomatic refractory epilepsy. [42] However, several studies show the possibility of misdiagnosis or bias of sampling. They even suggest that stereotactic biopsy may be an additional, even unnecessary procedure in the management of glioma, because it added an additional 0.9% and 4% risk of mortality and major morbidity, in each, and led to an inaccurate diagnosis in one-third to one-half of the cases. [43],[44] Despite discrepancies between histopathology and clinical phenotype, some studies have shown that appropriate treatment was administered in more than 90% of the LGG cases. [45] From a pure risk taking vantage point, stereotactic biopsy may be more beneficial than craniotomy. In contrast to biopsy, surgical resection can minimize the likelihood of sampling error, but it exposes the patients to a higher risk. [5] Although not curative, total resection provides multiple benefits, including reduction in cell number, increased efficacy of adjuvant therapies, and symptomatic relief. Interestingly, studies have shown that a large preoperative tumor size is a poor prognosis factor. [46] Although there are many retrospective data [Table - 2] showing the benefit of extensive surgery for overall survival or QOL in LGG, [47],[48],[49],[50],[51],[52] these are limited by the retrospective nature of these studies. There have been two prospective trials [Table - 2], which showed the benefit of extensive surgery on overall survival or progression-free survival by univariate analysis. [49],[53] Despite consistent findings on univariate analysis, on multivariate analysis, the benefits of extensive surgery were minimal in these studies. To date there is no class I evidence supporting radical tumor removal in LGGs. In addition, several articles recently revealed that brain MRI has a serious limitation to delineating the true tumor extent when methionine positron emission tomography (PET) or fluorodeoxyglucose (FDG) PET were used. [54],[55] Nonetheless, many neurosurgeons opt for extensive surgery in LGGs. The definition of the extent of resection has been evaluated on the basis of the surgeon′s impressions alone (which frequently overestimate the extent of resection), while in others it has been assessed by CT or postoperative T2-weighted or fluid-attenuated inversion-recovery (FLAIR) MRI images. [5] Obviously future trials should use MRI for evaluating the extent of resection rather than relying on the neurosurgeon′s opinion. Interestingly, recent studies suggested neoadjuvant temozolomide chemotherapy before surgery could result in shrinkage of the unresectable tumor. [56],[57] Even though a couple of nonrandomized studies showed even temozolomide chemotherapy alone shrank a tumor volume enough to consider further surgery, [31],[58] the real effects, benefits, and risks are still being investigated by the European Organization for Research and Treatment of Cancer (EORTC) / National Cancer Institute of Canada (NCIC). The impact of the extension of surgical resection on HGGs had been studied extensively. In 11 series reported after 2000, seven of them showed statistics in favor of more extensive resections, whereas, in four this was not the case [Table - 3]. The key point here is related to the type of analyses used to determine the extent of resection. Six studies used nonvolumetric analyses, relying on the surgeon′s estimation of the extent of resection. In the five that used volumetric analyses, they did show survival advantages with extensive resections. However, once again, these were mostly retrospective studies, influenced by biological factors, including age and Karnofsky performance scores, among other biases that were introduced. In 2006 Stummer et al . performed a randomized controlled multicenter phase III trial with the use of 5-aminolevulinic acid (ALA) for Fluorescence-guided glioma surgery, [15] showing 65% "complete resection" compared to 36% in the control group, showing an accurate estimation of the value of the extent of resection for HGG. How this technique ultimately relates to overall patient survival remains to be determined. Conclusions Our review investigated numerous reports in the literature supporting the importance of surgery for the treatment of low- and high-grade gliomas. Many articles showed the impact of more extensive and aggressive resections. However, most of the studies are retrospective or multivariate and nonrandomized in nature. Today, the management of these patients relies on combined therapies, which have been evolving over the last two decades. Concerning the role of surgery in patients with LGGs and HGGs, it is hoped that definitive trials lie just ahead. For the moment, clinicians should continue to individualize the management of their patients, taking into account the patient′s age, tumor location, imaging studies, pathology of the tumor, and prognostic molecular markers. [68]Acknowledgments This study was partly supported by the Kangwon National University (Ho Jun Seol), the Wiley Fund, and Brainchild, at the Hospital for Sick Children.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09024t3.jpg] [cn09024t2.jpg] [cn09024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}