 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
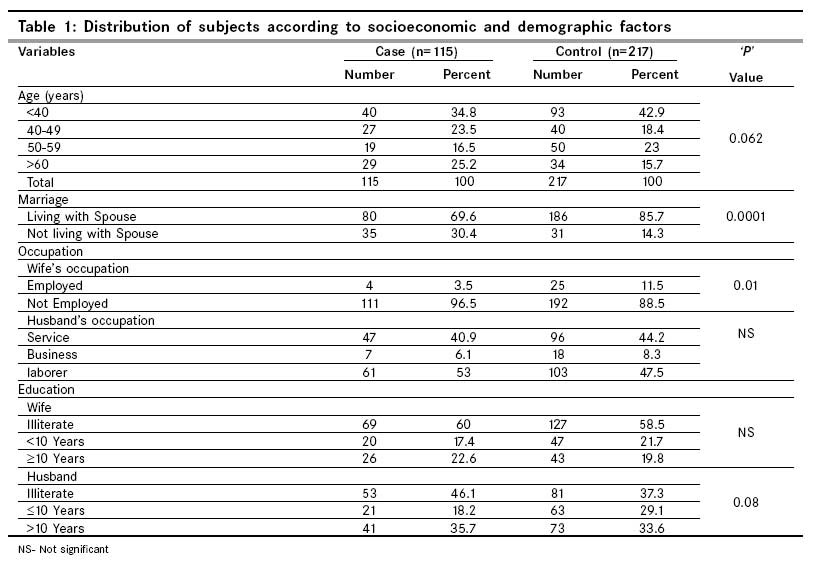
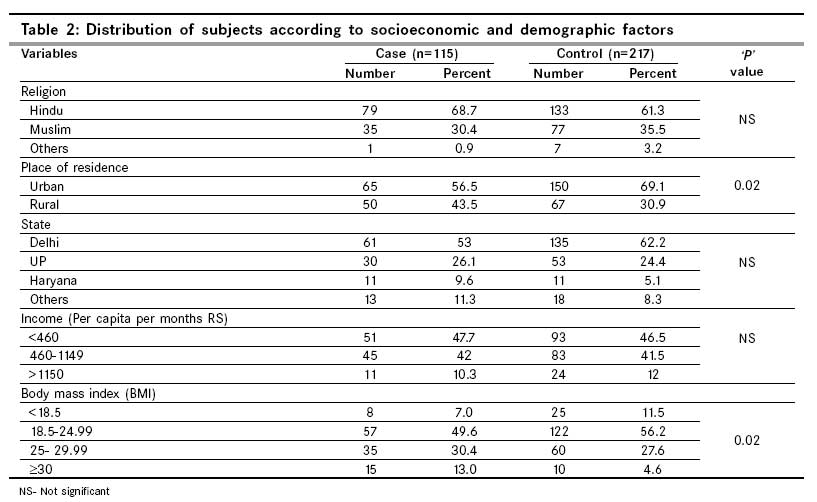
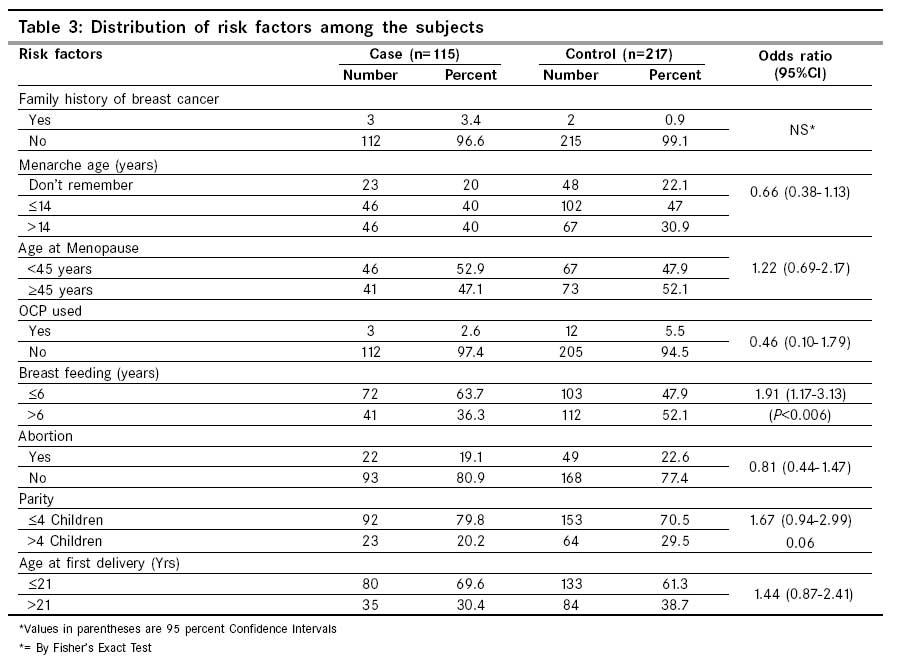
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 132-138 Original Article Risk factors with breast cancer among women in Delhi Pakseresht S, Ingle GK, Bahadur AK1, Ramteke VK2, Singh MM, Garg S, Agarwal PN2 Department of Community Medicine, 1Radiotherapy and 2 Surgery, Maulana Azad Medical College, New Delhi, India Code Number: cn09026 Abstract Background: The incidence of breast cancer is on the rise in India, breast cancer is the second most common malignancy in Indian women. In the present study 52.9% of the cases and 47.9% of controls had attained menopause before the age of 45 years, and a higher number of controls were living with spouses than cases (P < 0.0001). A larger number of controls (150, 69.1%) were living in urban areas than cases (65, 56.5%) (P<0.05). There was a significant difference between breast cancer cases and controls in relation to place of residence, occupation, marital status, body mass index and breast feeding. Keywords: Breast cancer, risk factor, women Introduction More than one million new patients suffer from breast cancer annually in the world. In developed countries, breast cancer is the most common malignancy diagnosed among women, and in developing regions, it ranks second to cervical cancer. [1],[2] Among American women, breast cancer represents 32% of all new patients of cancer and is the second leading cause of cancer deaths (15%) after lung cancer. [2],[3] It is estimated that 211,240 patients suffer from invasive breast cancer in a year in the United States. These numbers represent a sharp increase over the past 30 years. [4] Currently, in India, the incidence of breast cancer has steadily increased over the years and as many as 100,000 new patients are being detected every year. [2] The increase reported by the cancer registries is nearly 12% from 1985 to 2001, representing a 57% rise in India′s cancer burden. [3],[5] The trends for increase in breast cancer incidence over time for most of the population in India were found to be statistically significant. [6] Trends in breast and cervix cancer in six population based cancer registries (Mumbai, Bangalore, Chennai, Delhi, Bhopal, and Barshi) were evaluated over the last two decades. This approach showed a decreasing trend for cancer of the cervix and increasing trends for cancers of the breast throughout the entire period of observation in most of the registries. [7] The cancer registries also suggest that age-standardized incidence rates are rising even more rapidly in low-incidence regions such as Africa and Asia. Probably the socio-economic and lifestyle changes (e.g., late child-bearing and dietary changes) and associated changes in menstrual patterns are responsible for the rise in developing countries. At the same time, improved life expectancy will increase the burden of breast cancer in developing countries as more older women are likely to develop breast cancer than younger women. [8],[9] Geographical variation in incidence of breast cancer can be attributed to exposure to various risk factors. Among these, the high risk factors are: (1) Early menarche (2) Late menopause (3) Late first full-term pregnancy (4) Nulliparity (5) No breast feeding (6) Family history of breast cancer in two or more first-degree relatives (7) Hereditary breast cancer. The minor risk factors are: (1) Obesity in postmenopausal women (2) Hormone Replacement Therapy (3) Smoking (4) Exposure to low-dose radiation (5) Excessive alcohol intake. [7],[8],[9],[10] The present study attempts to find out some of the risk factors of breast cancer among patients attending Lok Nayak Hospital in New Delhi. Materials and Methods This is a case-control study conducted at Lok Nayak Hospital (LNJPH), New Delhi from January to December 2006. All the newly diagnosed cases of breast cancer attending surgery out patient department (OPD) and wards during this period were included as the study cases. The diagnosis was based on fine needle aspiration cytology (FNAC), incision biopsy, mammography, and clinical examination. The cases having any cancer other than breast cancer were excluded from the study. Thus a total of 115 women with breast cancer were included in this study. The controls were selected from the patients attending surgery OPD and wards during the same period by matching for age and sex. One to three controls were selected for a case of breast cancer by matching for age within ± 2 years age difference and without having any type of cancer. A total of 217 subjets acted as controls. None of the controls were missed or refused to participate. Data was collected by interviewing the subjects using a predesigned and pretested questionnaire, which included preliminary data, reproductive history, family history of breast cancer, parity, socioeconomic status, age at first full-term pregnancy, marital status, breast feeding, menarche, menopause, religion, family history of breast cancer, use of oral contraceptive pills, etc. Informed consent was taken from the study subjects before the interview. The reference date for recording information was the date of diagnosis for cases and the date of initial contact for controls. Statistical methods The data was analyzed statistically using Chi-Square test and Odds ratio with 95% confidence interval. All analyses were performed with SPSS version 11.5 software and EPI-INFO Version 3.03. Results [Table - 1] and [Table - 2] shows distribution of socio-demographic characteristics of cases and controls. Age of the cases ranged from 25 to 80 years (mean = 47.73, median = 45 years), and age of the controls ranged from 24 to 78 years (mean = 45.64, median = 45 years). 34.8% cases and 42.9% controls were in the age group < 40 years. Sixty one (53 %) cases and 135 (62.2%) controls were from Delhi [Table - 1]. Seventy nine (68.7%) cases and 133 (61.3%) controls were Hindus, while the others were nonHindus. Sixty nine (60%) cases and 127 (58.5%) controls were illiterate, and 111 (96.5%) cases and 192 (88.5%) controls were housewives. Husbands of 46.1% cases and 37.3% controls were illiterate. Sixty one (53%) husbands of cases and 103 (47.5%) husbands of controls were laborers. Fifty one (47.7%) cases and 93 (46.5%) controls were having income less than Rupees (Rs.) 460 per capita per month (the median income). In this study most of the study subjects (49.6% of cases and 56.2% in controls) had BMI in the range of 18.5 - 24.99. There was a significant difference in relation to BMI ( P =0.02) [Table - 2]. The mean age of menarche was 14.25 years among cases and 14.24 years among controls. The mean age at first delivery was 20.8 years in cases and 21.4 years among controls. We observed that, 74 (64.3%) cases and 103 (47.5%) controls had breast fed at most three children, 90 (78.3%) cases and 155 (71.4%) controls had breast fed at most four children and the mean of duration of the sum total breast feeding for all children was 6.58 years in patients and 7.4 years in controls (OR=1.91; 95% CI, 1.17 - 3.13) (P < 0.006). Only 19.1% cases and 22.6% controls had one abortion (OR = 0.81, 95% CI; 0.44 - 1.47). 92 (79.8%) cases and 153 (70.5%) controls had parity of at least four (OR = 1.67; 95% CI, 0.94 - 2.99). One hundred twelve (97.4%) cases and 205 (94.5%) controls did not use oral contraceptives. 112 (96.6%) cases and 215 (99.1%) controls did not have any history of breast cancer in the family [Table - 3]. In the present study only one person was reported to be smoking and no one reported to be drinking among the cases, whereas, no one was reported to be smoking or drinking among controls. The finding of this study did not show any significant difference in the wife′s education, religion, states of origin, income, parity, abortion, age at first delivery, oral contraceptive use, and family history with breast cancer ( P >0.05). This study revealed that the mean age at menopause was 44.92 years in cases and 44.44 years in controls. In the present study 52.9% of cases and 47.9% of controls had attained menopause before the age of 45 years. A significantly higher proportion of breast cancer cases 80 (69.6%), were living with spouses than controls 186 (85.7%), ( P = 0.0001) and others were either widows, divorcees or separated. Sixty-five (56.5%) patients and 150 (69.1%) controls lived in urban areas ( P < 0.02). Discussion Breast cancer is associated with various factors. In this study, we found a significant difference between breast cancer cases and controls in relation to marital status, place of residence, occupation, BMI, and breast-feeding. The mean age at diagnosis of cases was 47.73 years. 58.3% of cases and 61.3% of controls were < 50 years of age. Other studies reported 33% of women with breast cancer were less than age 50 years at the time of diagnosis. [11],[12] Women between the ages of 20 years and 29 years accounted only 0.3% of breast cancer patients. [1] In our study, the mean age at menarche was 14.25 years among cases, 14.24 years among controls, and no significant difference in breast cancer risk by age of menarche was found. In a study, 50% subjects had the age at menarche > 13 years. [13] A similar finding was reported in another study. [14] Early age at menarche is associated with increased risk of breast cancer and there appears to be a 20% decrease in breast cancer risk for each year if menarche is delayed. [15],[16] Studies reported that women who began menstruating at an early age (before age 12) and those who reach menopause after age 55 years had an increased risk of breast cancer .[17],[18] Buchholz et al. found that the age at menarche was negatively associated with breast cancer risk regardless of Estrogen and Progesterone Receptor (ER/PR) status. In comparison with women who had menarche before the age of 12 years, later age at menarche (at least 14 years) was associated with an approximately 40% reduced risk of breast cancer. [19] The variations observed in different studies could be due to the difference in the socio-demographic, geographical, and lifestyle factors. In the present study, religion, state of origin, parity, abortion, oral contraceptive uses, and family history of breast cancer did not show any significant association with breast cancer. Study by Gajalakshmi et al. showed that breast cancer risk factors significantly modified the effect of Hormone Replacement Therapy (HRT) on breast cancer risk, particularly first-degree family history of breast cancer, higher age, lower education, higher body mass index (BMI), and nonuse of oral contraceptives (OCP) during lifetime. [18] Many studies have not confirmed an overall excess risk associated with use of oral contraceptives, but a number of studies have suggested that long-term use of oral contraceptives is associated with a higher risk for early onset of cancers, usually those occurring before age 45 years. [20] In this study 49.6% of cases and 56.2% of controls had Body Mass Index (BMI) in the range of 18.5 - 24.99. 30.4% of cases and 27.6% of controls had BMI in the range of 25 - 29.99 and 13% of cases and 4.6% of controls have BMI =>30. BMI was significantly higher among the cases than controls ( P =0.02). A study reported that the increased BMI (OR=1.33, 95% CI: 1.05-1.69 for 25.0-29.9 kg/m(2) and OR=1.56, 95% CI: 1.03-2.35 for 30+ kg/m(2) were associated with pre-menopausal breast cancer risk. The data support the hypotheses that increased anthropometric factors (Body mass index (BMI)>25.0 kg/m(2), waist size > 85 cm and hip size > 100 cm) are risk factors of breast cancer in India. [21] Body size influences breast cancer risk differently in premenopausal and postmenopausal women; higher weight is associated with a lower risk of premenopausal breast cancer, whereas risk is reported to increase with BMI in postmenopausal white women. [22] Weight control may reduce the risk among postmenopausal women. [23] This study revealed that the mean age at menopause was 44.92 years in cases, 44.44 years in controls. In present study 52.9% of cases and 47.9% of controls had attained menopause before the age of 45 years. In similar studies Pre-menopausal women comprised 27%, [24] 44.6% [25] and 49.7%. [26] Some studies found early menarche and late menopause can be affecting in breast cancer. [27] Some studies found late menopause as risk factors for breast cancer. [10],[28],[29] A study reported that the risk of cancer did not differ with regard to menopausal status, age at menopause, and ever-use of hormone replacement therapy. [14] There was equal distribution of pre- and post-menopausal women, 49% vs. 48% respectively. It is reported that whereas 73% of white female subjects are postmenopausal at diagnosis, only 35%, 49%, and 52% of Asian, black, and mixed-race subjects, respectively, are postmenopausal. [11] A significantly lesser proportion of breast cancer patients were living with spouse (69.6%) as compared to controls (85.7%) ( P < 0.0001). Similar findings were reported in other studies. [14],[25] Sixty-five (56.5%) cases and 150 (69.1%) controls lived in urban area ( P =0.02). Dalton et al. found an urban-rural, gradient, with higher risk among rural women (OR 1.10; 95% CI, 1.02, 1.18) and lower risk among women in the capital suburbs (OR, 0.85; 95% CI: 0.78, 0.93) and capital area (OR = 0.93; 95% CI: 0.84-1.02). [12] Other studies reported (55%), [24] (60%), [30] women with breast cancer came from the rural areas. A study reported breast cancer incidence in India is approximately twice as high in urban women as in rural women. [21] Our study showed that, 112 (96.6%) cases and 215 (99.1%) controls did not have breast cancer in the family. In recent years, various authors have shown that approximately 5 to 10% of all breast cancers can be accounted for hereditary breast cancer susceptibility disorders. [31] Several major studies have conducted more detailed analyses and agreed that about 6% of breast cancer before the age of 55 years is linked to a family history of breast cancer in first-degree relatives. If a woman′s blood-related relatives on either her mother or father′s side of the family have had breast cancer, then she is at increased risk for the disease. [2],[20] Although, the majority of women in the population do not have a family history of breast cancer, family history has long been recognized as a key risk factor for the development of this disease. [2],[17] We did not find an association of breast cancer with family history. This could be due to less number of patients in our study, and maybe because of increased incidence of this disease in recent years. In this study we observed that, 74 (64.3%) cases and 103 (47.5%) controls had breast fed at most three children, 90 (78.3%) cases and 155 (71.4%) controls had breast fed at most four children and the mean duration of the sum total of breast feeding for all children was 6.58 years in patients and 7.4 years in controls (OR = 1.91; 95% CI, 1.17 - 3.13) ( P < 0.006). Gajalakshmi et al. showed duration of breast-feeding was negatively associated with breast cancer risk regardless of ER/PR status. [18] There is a decrease of 4.3% in risk for every 12 months of breast-feeding, so that the protective effect becomes clearly evident only after many years of breast-feeding. [1],[2],[29] The mean age at first delivery in cases was 20.8 years and in controls was 21.4 years. 69.6% of cases and 61.3% of controls delivered the first child at ≤21 years of age. Michael et al. showed that a slight increase in risk for ER + PR + breast cancer and a reduced risk for ER - PR - breast cancer was observed with increasing age at first full-term pregnancy. [1] Similar studies reported that the mean age at first delivery was 21 years. [24,32] Another study showed that 17% subject′s age at first birth was < 20 years. [13] Women who had their first child after age 30 years or who never had a child were at a slightly higher risk for developing breast cancer. [33] In contrast, there are consistent results that early age at first full-term pregnancy is not a strong protective factor in young women. [34] The result of this study is consistent with the results of many other studies. Conclusions The current data support that various factors like marital status, wife′s occupation, place of residence (urban/rural), BMI, and breast-feeding were significantly associated with breast cancer (p < 0.05). Income, religion, age at menarche and menopause, parity, abortion, oral contraceptive, family history of breast cancer, wife′s and husband′s education, and husband′s occupation did not show any significant association with breast cancer.Acknowledgment The authors duly acknowledge the contribution and help of Surgery Department, PSM Department and Department of Radiotherapy, Maulana Azad Medical College, Lok Nayak Hospital, New Delhi in preparation of this paper.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09026t3.jpg] [cn09026t2.jpg] [cn09026t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}