 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 139-145 Original Article Prognostic significance of location of the primary tumor in operable breast cancers Hazrah P3 , Dhir M1, Gupta SD2 Deo V2, Parshad R3 Department of 2Pathology, 3Surgical Disciplines, All India Institute of Medical Sciences, New Delhi and
1All India Institute of Medical Sciences, New Delhi – 110 029, India Code Number: cn09027 Abstract Background: The prognostic significance of the primary tumor site in breast cancers is not established with only a few studies having evaluated the issue.Materials and Methods: The relevance of a primary tumor site with respect to systemic disease relapse was evaluated in 187 patients with breast cancer treated with primary surgery and adjuvant chemotherapy, in whom the location of primary tumor was classifiable in any one of the three sites, namely: outer, periareolar, and inner, quadrants. Data was obtained from prospectively maintained records of breast cancer patients treated at a single surgical unit in a tertiary care center. Results: The three groups were comparable with regard to demographic, pathological tumor, and treatment characteristics. In the multivariate analysis, patients with inner and periareolar quadrant tumors had a higher hazard for systemic disease relapse, (2.53, 95% CI: 1.18-5.42; P = 0.02, and 2.73, 95% CI: 1.04-7.14; P = 0.04, respectively) as compared to outer quadrant tumors. The projected five-year survival estimates in Kaplan Meier were 87%, 61%, and 69%, respectively, for outer, periareolar, and inner quadrant. On further substratification the difference was particularly noted in high risk inner quadrant tumors: age < 45, premenopausal patients, tumor size >2 cms, positive nodes and intermediate or high grade histology, as also in patients treated with breast conservation and CMF, Cyclophosphamide, Methorexate, 5 Fluorouracil chemotherapy. Conclusion: The location of the primary tumor influences survival in breast cancer with inferior outcome for tumors in inner and periareolar quadrants, especially in high risk groups and those treated with conservative approaches. The role of aggressive therapies merits investigation in these patients. Keywords: Metastasis, risk factor, survival, systemic relapse, tumor site, quadrant Introduction The site of location of a tumor in an organ has been known to affect treatment options and survival in some cancers, [1],[2],[3],[4] however, its role in breast cancer has not been defined. There is evidence to suggest that the quadrant of involvement in breast cancer can affect disease recurrence, [5] distant relapse, and survival. [6],[7],[8],[9] However the issue is as yet considered controversial and a recent study failed to find any influence of intra-mammary tumor location on the disease outcome. [10] Controversy also exists regarding tumor site classifications. Central or periareolar tumors have usually been combined with outer [8] or inner quadrants [6] or excluded from the analysis [7],[10] in most studies. This study was undertaken to compare the impact of the location of the tumor, with respect to quadrant of involvement, on systemic disease relapse in patients with breast cancer, treated with primary surgery and adjuvant systemic therapy. Materials and Methods This is a retrospective analysis of prospectively recorded data on operable breast cancer patients. Data on patients treated for breast cancer in the Department Of Surgery at our institute is prospectively maintained in clinical record files at the Breast Cancer Clinic. The study cohort included all patients treated in a single surgical unit during the period from 1994 to 2005, who fulfilled the selection criteria given below Inclusion criteria : Patients who were primarily operated (in T classes 1 - 3 and Nodal status N0 - N2) and had received postoperative adjuvant chemotherapy, with tumors located in the breast, classifiable into the following quadrants.
The classification was made on the basis of records of clinical examination and mammographic findings whenever such was available. Patients excluded : Patients with multiple primary tumors, nonpalpable or occult primary, unspecified quadrant of involvement, tumors that involved more than one quadrant, that is, overlapping tumors, and breast cancer in males, have been excluded. Evaluation and follow up : The patients were evaluated in the follow-up period with clinical examination, serum alkaline phosphatase, and chest X-ray routinely, every three months for the first three years, every six months for the next two years, and thereafter yearly. A yearly mammogram was also done for evaluation of disease relapse in residual breast, in patients treated with breast conservation. and in the opposite breast, in all cases. Furthermore, patients suspected to have disease relapse were further investigated with additional scans and treated accordingly. Analysis : Analysis was done with respect to the three groups classified, based on tumor location, that is: Outer, periareolar, and inner quadrants. A computerized grouped database of the patients was created using established risk criteria, treatment administered, and follow-up information. Statistical analysis was done using the Statistical Package for the Social Sciences (SPSS) package. Continuous normally distributed data have been analyzed using the t test and not normally distributed data were analyzed using a nonparametric test, namely, the Kruskall Wallis test. Categorical data have been evaluated using Chi Square tests. Survival has been analyzed using the Kaplan Meier curves and the difference evaluated using the log rank test for univariate analysis. Multivariate survival analysis was done using Cox′s proportional hazard model, using stepwise selection. The dependent variable and the time frame in consideration were as follows : Event: Systemic disease relapse Time Frame: Time in months calculated from date of surgery to date of first diagnosis of systemic relapse, for patients who had disease relapse, and from date of surgery to date of last follow-up, for patients alive and disease free. The independent variables considered have been listed below as also their prognostic categorization as used in the analysis:
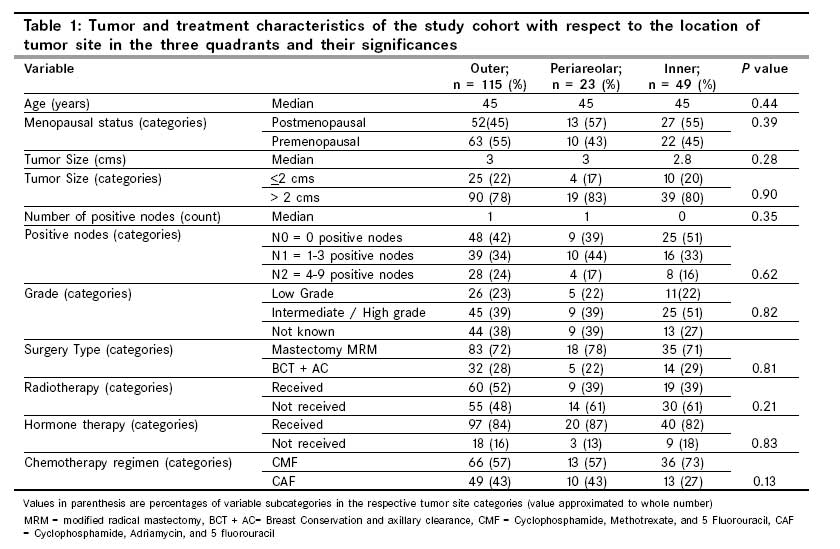
Results A total of 187 patients were identified who fulfilled the inclusion criteria. The median age of the study population was 45 years, median tumor size 3 cms, and median follow-up 43 months. The commonest site of tumor location was the outer quadrant seen in 62% (n = 115), followed by inner in 26% (n = 49), and periareolar in 12% (n = 23). The descriptive statistics of the three groups has been tabulated in [Table - 1]. There was no significant difference among the three groups with respect to presentation characteristics and treatment options. [Table - 2] shows the projected Kaplan Meier five-year survival estimates expressed as % + SE and their significances in the log rank test, compared pair-wise for the three tumor site locations, separately, for individual substrata classifications. Patients with tumors in the inner and periareolar quadrants had a significantly poorer outcome than those located in the outer quadrants (p-value = 0.01, and 0.03, respectively, for the inner and periareolar quadrants in comparison with the outer quadrants). On further substratification the difference related to tumor site location was notable, with inferior survival for inner quadrant tumors, especially in high-risk patients:
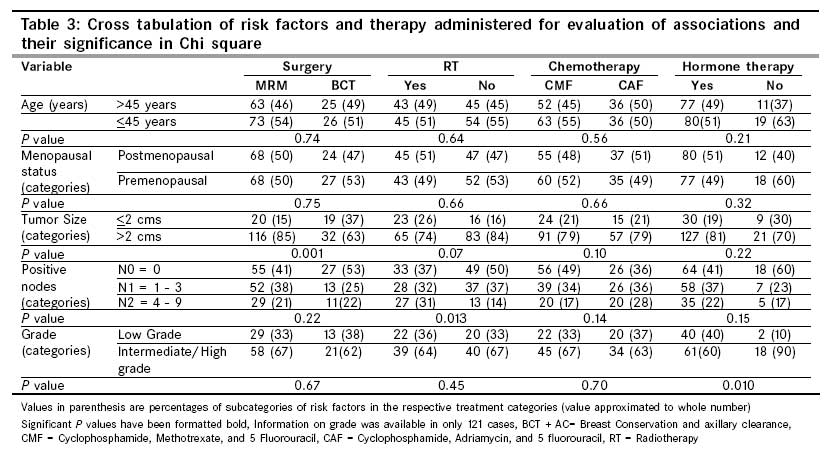
As the difference in survival varied with the risk stratifications and type of treatment, a further analysis was done to assess any possible association between risk categories and therapies [Table - 3]. In multivariate regression using COX′S proportional hazard model, with inclusion of the independent factors previously listed, the location of the tumor in the inner and periareolar quadrants was observed to be associated with higher hazards for systemic disease relapse when compared with that of the outer quadrant tumors. Data on the Nottingham combined grade was present in only 121 cases, but the significance with respect to tumor site location in multivariate analysis persisted both on inclusion and exclusion of the grade as an independent factor. A hazard ratio of 2.53, 95% CI: 1.18 - 5.42; p value = 0.02 and 2.73, 95% CI: 1.04 - 7.14; P value = 0.04 was observed for the inner and periareolar quadrants, respectively, when compared with that of the outer quadrant tumors. Additionally the number of pathological positive nodes and the type of chemotherapy regimen also emerged as significant independent predictors with higher hazards for patients with more number of positive nodes and those treated with CMF chemotherapy. (hazard ratio 4.01, 95% CI: 1.70 - 9.42; P value = 0.00 for 1 - 3 positive nodes and 3.19, 95% CI: 1.21 - 8.39; p value = 0.02 for 4 - 9 positive nodes as compared to node negative patients and a hazard ratio of 4.21, 95% CI: 1.46 - 12.14; p value = 0.01for patients who had received CMF chemotherapy as opposed to CAF chemotherapy). The sites of relapse in the patients of the respective groups were also further evaluated for any probable internal mammary relapses, that is, documented internal mammary metastasis, parasternal relapses, mediastinal metastasis or pleural effusion without parenchymal lung metastasis. There was no difference among the groups as regards probable internal mammary metastasis observed in four, four, and two cases, respectively, in the outer, inner, and periareolar quadrant tumors. Discussion In our study patients with inner quadrant tumors had higher hazards for systemic disease relapse when compared to those located in the outer quadrants (2.53, 95% CI: 1.18 - 5.42; p value = 0.02). Although a difference in systemic disease free survival was noted in the whole study group (projected five-year survival 87% vs 61% vs 69% for outer, periareolar, and inner quadrant tumors, respectively), further substratification revealed that the inferior survival of inner quadrant tumors was confined only to patients with high risk features, that is, age < 45 years, premenopausal status, intermediate and high grade histology, tumor size> 2 cms, positive axillary nodes, and in patients who were less aggressively treated, that is, with breast conservation, and CMF chemotherapy. Literature evidence reflects on a poorer outcome of inner quadrant tumors and the difference in survival of patients with inner quadrant tumor has been reported to vary in high-risk and low-risk disease stratifications as also among treatment subgroups. [7],[8] Our findings corroborate with that of Lorisch et al. who had evaluated medial and lateral half tumors for systemic relapse. They had observed 50% excess risk of systemic relapse and breast cancer deaths in patients with tumors in the medial halves. In their study the difference in survival of patients with inner quadrants was observed mainly in a subgroup of high- risk patients, that is, greater than 2 cm tumors with positive axillary nodes. [7] Other authors have reported that inferior survival persists irrespective of nodal status. [6],[8] However, use of systemic therapy was taken into consideration as a discriminant in the former, [7] but not in the latter two studies . [6],[8] A difference with respect to the type of surgery and radiotherapy has also been suggested. Gaffney et al . proposed that the survival difference was particularly observed in inner quadrant tumor patients treated with mastectomy without local radiotherapy, as opposed to breast cancer patients treated with breast conservation and local radiotherapy, thereby emphasizing the role of possible internal mammary radiotherapy. However, data in their study was obtained from heterogeneous sources in cancer registries and it is not known whether any special radiotherapy was given for internal mammary nodes in the respective centers. [8] In another study evaluating local recurrence, but not distant relapse, in breast cancer patients, the location of tumor in the inner quadrants was cited to be a borderline risk factor in patients treated with mastectomy. [5] On the contrary Zucali et al. had observed a 30% increase in risk for distant relapse, in the inner / central tumors, treated with a conservative approach. [6] They had compared inner and central quadrant tumors as a combined group with outer quadrant tumors, as they observed the survival of the former two groups to be similar and had evaluated for distant relapse, which contrasts with that of Gaffney et al. who had compared disease relapse including local relapse of outer and central quadrant tumors combined as a single group entity with that of inner quadrant tumors The diminished survival of inner quadrant tumors has been attributed to untreated internal mammary metastasis. Data from a series of patients treated with extended radical mastectomy has shown that incidence of internal mammary metastasis may be as high as 44-65% in inner quadrant tumors. [11] However the clinical relapse in undissected internal mammary chain for patients treated with modified radical mastectomy and adjuvant systemic therapy may be as low as or even less than 1% with or without prophylactic radiation [11] and it is important to note that the site of relapse is not necessarily the mediastinum and often, distant failure rather than local recurrence is the first site of relapse in these patients. [11] Alternatively reports exist of increased incidence of pericardial and pleural effusion in inner quadrant disease. [12] In our series the incidence of mediastinal relapse, as evidenced from documented internal mammary metastasis, parasternal relapses, and isolated mediastinal nodal involvement, as also the proportion of patients with pleural effusion or intrathoracic relapses in inner quadrant tumors was not significantly higher than those in outer quadrant tumors. It has been argued that the incidence of internal mammary relapse may be low due to the fact that most patients with axillary node positive disease and larger tumor sizes usually receive chemotherapy. [11] It also may be an underestimation of the true incidence of internal mammary relapse given the limitations of conventional imaging and CT (computed tomogram) scans, in the detection of internal mammary metastasis . [13] As significance of the type of treatment given has been suggested to be influencing survival in most studies evaluating the prognosis of inner quadrant tumors, it appears that additional therapy may be beneficial in these patients. Additional therapies targeting the internal mammary nodes, namely, internal mammary dissection and irradiation have been the commonly evaluated treatment modalities. Although the results of internal mammary dissection have been controversial, [14],[15] relative benefits have been observed in a subgroup of inner quadrant tumors, especially with positive axillary nodes. [16],[17] The role of internal mammary irradiation is also controversial and any relative benefits of internal mammary radiation is believed to be offset by an increase in the number of deaths due to cardiovascular events. [18],[19] Until the completion of an ongoing randomized trial to address the issue, definite conclusions cannot be drawn. Additional treatment for the internal mammary node, namely, internal mammary dissection and/or radiotherapy for internal mammary nodes was not given to any of our patients. In our study, patients with inner quadrant tumors who were treated with radiotherapy had an inferior survival curve when compared to outer quadrant tumors in a univariate analysis. A possible explanation for this observation could be that radiotherapy was administered to patients in high-risk categories (i.e., greater number of axillary nodes). We have also observed that inner quadrant tumors treated with CMF chemotherapy had an inferior survival when compared to their counterparts with tumors in the outer quadrants, which was of borderline significance. In our study no difference in survival was noted in patients treated with CAF, and in this context, it remains to be determined whether use of better chemotherapeutic regimens can decrease the observed difference in survival related to tumor site. Another issue that needs clarification is the status of central/periareolar tumors in quadrant classifications, which has been varied and largely arbitrary. Some authors have included them in one of the two groups namely outer or inner, [6],[8] and others have excluded them from the analysis in entirety. [7],[10] Zucali et al. had included medial and central groups as a similar variable, [6] whereas, Gaffney et al. have found no difference in breast cancer specific survival rates among the outer quadrant and central tumors and have combined such tumors as a single subset in their analysis. [8] Alternatively, it has been suggested that breast cancers be classified by their distance from the axilla. [9] Although central quadrant tumors have been shown to have an intermediate rate of internal mammary node involvement, the rates can be very high (63%) if the nipple is involved. [11] Despite the small number of patients with periareolar tumor in our study, they had significantly inferior survival and higher hazards of systemic relapse (hazard ratio 2.73 95% CI: 1.04 - 7.14; p value = 0.04) in comparison with outer quadrant tumors. A clinically useful prognostic factor is one that is statistically significant, independent, and clinically relevant. [20] Quadrant of involvement in breast cancer can emerge as an important parameter in this regard. If the inferior survival seen in inner quadrant tumors is due to a true reflection of internal mammary metastasis, more studies on the exact stratification of prognosis based on tumor site locations may be able to help in the development of a quadratic classification adjusted for tumor locations, which can ease the difficulties that relate to detection of internal mammary nodes, for staging. [21] On the other hand, if the adverse outcome relates to alternate pathways of spread, which may not necessarily be the internal mammary route, the quadrant of involvement has the potential to evolve as an additional prognostic parameter. Also unlike other prognostic variables like tumor size and nodal status, the quadrant of involvement as such is relatively independent of the effect of a temporal association with the disease and thus may be especially beneficial in an unscreened population, where most patients present in advanced stages. However the number of patients who present with inner and central quadrant disease being small in our study, these observations merit substantiation in a larger series. Conclusion We have observed that the location of a primary tumor is an independent predictor of systemic relapse in operable breast cancer patients with higher hazards for patients with tumors located in inner and periareolar quadrants as compared to patients with outer quadrant tumors. The inferior survival outcome was observed more in the high-risk groups of inner quadrant tumors and those treated with conservative therapies. The findings of our study further substantiate the likely importance of the tumor site as a prognostic factor in operable breast cancers. Investigation on the use of additional therapies to improve the outcome in such patients is suggested.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09027t2.jpg] [cn09027t1.jpg] [cn09027t3.jpg] |
| |||||||||

{kind=link}
![Table - 2]](/showimage?cn/photo/cn09027t2.jpg){kind=link}
{kind=link}