 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 151-154 Original Article Tamoxifen use and gallstone formation in postmenopausal breast cancer patients in south Indian population Mohamed APA, Kadambari D, Bhuvaneswari V Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry Code Number: cn09029 Abstract Background: Tamoxifen is being used in patients with estrogen receptor positive breast cancer as an adjuvant or palliative hormonal therapy. Western studies have found a 30% incidence of gallstones in patients who are taking Tamoxifen and they have proved a significant association between the two.Objectives : The objective of the study was to find out the association of Tamoxifen use and gallstone formation in postmenopausal breast cancer patients in a South Indian population. Methods: Ninety patients who had undergone surgery for invasive breast cancer in our institute, and were receiving adjuvant Tamoxifen, were recruited for the study. An equal number of age-matched postmenopausal women were taken as controls. All of them underwent an abdominal ultrasound screening test for gallstones. Presence or absence of gallstones was noted down from their ultrasound scan reports. Pretreatment status of the gall bladder was assessed from the preoperative scan reports. Results: An odds ratio of 1 was derived when the case group was compared with the control group. Conclusions: In our study we could not establish that an association existed between Tamoxifen use and gallstone formation in postmenopausal South Indian women. Keywords: Breast cancer, gallstones, postmenopausal women, tamoxifen Introduction Tamoxifen is a synthetic, nonsteroidal, trans isomeric derivative of triphenylethylene. [1] It has an estrogenic action on tissues such as endometrial and bone tissues, and antiestrogenic action on tissues like those in the breast. Breast cancer is the second most common malignancy in women in our country. [2] Currently, a multimodality approach, which consists of preoperative radiotherapy, neo adjuvant chemotherapy, surgical treatment, and hormonal therapy, is adopted for treating breast malignancies in most centers. [3] Tamoxifen is given to almost all patients who undergo surgery for breast malignancy which is estrogen sensitive. Because of the high prevalence of this particular malignancy, the number of patients receiving the drug is huge. Thus any adverse drug reaction caused by the drug will have a great impact on the quality of life of the patient. It is a well known fact that estrogen intake causes increased risk of gallstone formation. Other risk factors for gallstones are advancing age, female gender, use of oral contraceptives, pregnancy, obesity, rapid weight reduction, gallbladder stasis, hyperlipidemia syndromes etc. A vast majority of gallstones (>80%) are ′silent′ and most individuals remain free of biliary pain or complications due to gallstones for decades. [4] Among individuals of South Indian origin, the prevalence of gallstones was estimated to be 1.8%. [5] Certain animal experiments have demonstrated that Tamoxifen has an estrogenic action on the liver by which it increases the risk of gallstone formation. [6] In a retrospective cohort study done in Turkey, an increased risk of gallstone formation was found in postmenopausal breast cancer patients who were on t0 amoxifen. [7] No such study has been done in India. Optimal use of Tamoxifen with maximum benefit and minimum side effects is still an area of intense investigation. The relation between estrogen exposure and gallstone formation has been well known for a long time. [8],[9] Because Tamoxifen has an estrogen-like activity, a possible relation between long-term Tamoxifen administration and gall stone formation was evaluated in this study. Materials and Methods The subjects for our study were recruited from the Cancer Follow-Up Clinic of our hospital, after obtaining an informed consent. Most of them had undergone surgical treatment, chemotherapy, and radiotherapy for the malignancy and were on a regular follow-up. Demographic details including the age, locality, age at menopause, and so on, were collected. History pertaining to the treatment of breast cancer and history related to gallstones were elicited. Presence or absence of gallstones before starting the treatment was noted from their pretreatment abdominal ultrasound scan reports. If they were found to have gallstones before starting the treatment, they were excluded from the study. As a part of the routine workup during the follow-up visits, an abdominal ultrasound scan was performed and the presence or absence of gallstones was noted. An equal number of age- and gender-matched controls were recruited from the Inpatient Department of Surgery and Medicine after obtaining informed consent. The data obtained were analyzed with appropriate statistical tests. Inclusion criteria
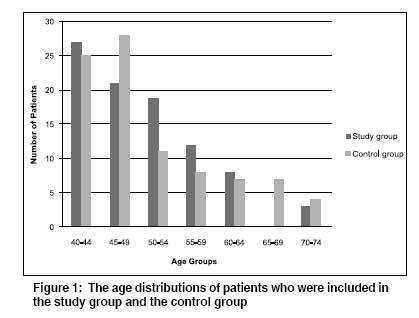
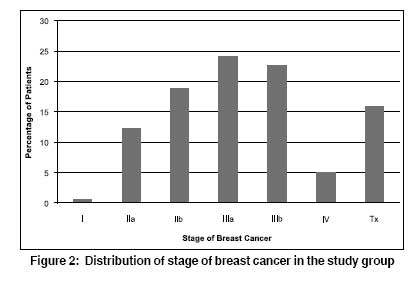
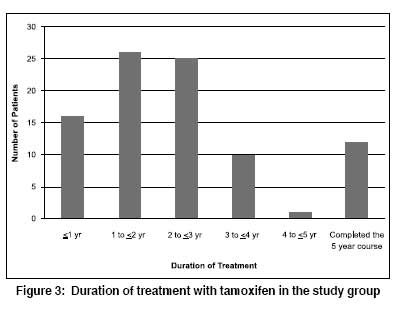
Results After applying the exclusion criteria, a total of 90 subjects were included in the study group. Two patients out of the 90 were found to have developed gallstones while they were on treatment with Tamoxifen. Two out of 90 controls were found to have gallstones. When this data was analyzed, an odds ratio of 1 was derived. The age distribution of patients who were included in the study group and the control group are illustrated in [Figure - 1]. [Figure - 2] shows the distribution of stage of breast cancer in the study group [Figure - 3] depicts the duration of treatment with Tamoxifen in the study group All patients had undergone radiotherapy and chemotherapy following surgery. None of the patients had any symptoms or signs suggestive of gallstone disease. The two patients who developed gallstones, while on treatment with Tamoxifen, were 47 and 55 years of age, and had received the drug for 3 years and 4 years, respectively. However, in the control group, the subjects who had gallstones were 40 and 45 years of age. Discussion Tamoxifen is one of the most effective antineoplastic drugs in use today and is prescribed to millions of women worldwide for the adjuvant or palliative management of breast cancer. [9] Tamoxifen exhibits antiestrogenic, estrogenic or mixed activity depending upon the species and the target genes measured. Recently, experiments on mice have proved that Tamoxifen has an estrogenic action on the liver, which increases the risk of gallstone formation. It is the activation of "estrogen-ERα-SREBP-2" pathway in the liver that augments cholesterol secretion in the bile, leading to increased lithogenicity, due to super saturation of cholesterol in the bile. Similar to estrogen treatment, Tamoxifen significantly promotes biliary cholesterol secretion and cholesterol gallstone formation in gonadectomized mice of both genders. [6] In clinical tests or laboratory studies with human cells, the drug′s activity depends upon the tissue and endpoint measured. [10] For example Tamoxifen inhibits the proliferation of cultured human breast cancer cells in vitro and reduces the tumor size and number in vivo, yet it stimulates the proliferation of endometrial cells and causes endometrial thickening. [11] Thus it has been associated with development of endometrial polyps, endometriosis, and an increased risk of endometrial cancer. [12] A retrospective cohort study done in Turkey has proved that there is an increased risk of gallstone formation in postmenopausal breast cancer patients who are taking Tamoxifen. Around 700 patients were recruited for the study and they were all followed up with annual abdominal ultrasound scans, to look for gallstones for a mean period of 4.7 years. A 33% prevalence of gallstones was found in patients who had taken tamoxifen for more than 3 years. The prevalence in the controls was 2%, which proved that there was a significant association between Tamoxifen and the gallstones. [7] None of the patients had any symptoms or signs suggestive of gallstone disease. All of them had received chemotherapy and radiotherapy following surgery. Around 24% of them had stage IIIa of breast cancer. Most of the patients were on Tamoxifen for 1 year to ≤2 years. The study and the control group were age matched in order to avoid bias. An odds ratio of 1 was derived when the study group was compared with the control group. Two women each in the study and control groups were found to have gallstones. Thus the causal association between Tamoxifen use and gallstone occurrence could not be proved in this study. Almost 24 patients out of the 90 had received Tamoxifen for more than 3 years in our study. The Turkish study found a significant association between the drug and the disease only if it was taken for a duration of more than 3 years. [7] In our study, although we could not prove such an association, the two patients who developed gallstones after starting them on Tamoxifen, had received the drug for a duration of 3 and 4 years. But in order to compare the two groups (those who had taken the drug for < 3 years and> 3 years), a larger number of patients would have to be studied. Several studies done on the effect of Tamoxifen on the endometrium (to assess the risk of endometrial carcinoma) in the West have proved that there is a significant increase in the risk. [13] But a similar study done in our Institute has failed to prove any increase in the risk of malignancy. [14] In the present study also, we could not find a significant association between Tamoxifen and gallstones. Further studies should be done to find out if this discrepancy is due to a genetic difference at the receptor level between the Western and Indian population. Acknowledgements This paper was done under the ICMR STS (Indian Council of Medical Research- Short Term Studentship) 2007 program.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09029f3.jpg] [cn09029f1.jpg] [cn09029f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}