 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
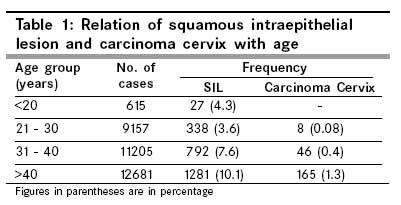
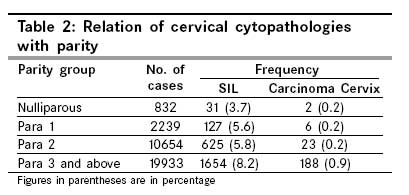
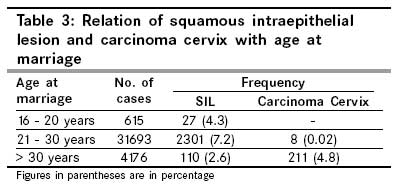
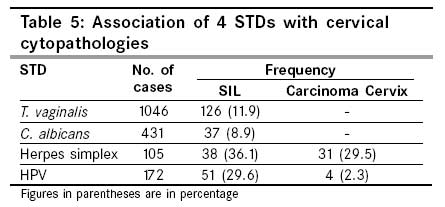
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 155-159 Original Article Risk-factors and strategies for control of carcinoma cervix in India: Hospital based cytological screening experience of 35 years Misra JS, Srivastava S, Singh U, Srivastava AN Department of Obstetrics and Gynaecology and Pathology, C. S. M. Medical University, Lucknow, India Code Number: cn09030 Abstract Purpose: Role of risk factors in cervical carcinogenesis and strategies for control of the disease have been assessed from the accumulated cytological data, derived from 35 years of hospital-based screening in Lucknow, North India.Materials and Methods: A total of 36,484 women have been cytologically screened during a span of 35 years (April 1971 - June 2005) in the Gynaecology out patient department (OPD) of Queen Mary's Hospital. Results: The frequency of Squamous Intraepithelial Lesion (SIL) and carcinoma was found to be 7.2% and 0.6%, respectively, in the present study. The study revealed high age and parity as a predominant factor in cervical carcinogenesis, while viral sexually transmitted disease (STDs) -human papilloma virus (HPV) and Herpes simplex virus (HSV) were also largely associated with SIL cases. The study emphasized great value of clinically downstaging the cervical cancer by detecting cervical cancer in the early stage. The study also revealed a significant difference in the frequency of SIL in symptomatic and asymptomatic women. Conclusion: Based on the analyzed data, it was felt that single lifetime screening, which appears to be the most feasible and affordable mode for control of carcinoma cervix in developing countries like India, should be carried out in all women of high parity irrespective of age (with three or more children) and in older women above the age of 40 years irrespective of parity. Keywords: Cervical cancer, risk factors, strategies for control Introduction Carcinoma cervix worldwide accounts for 15% of all cancers diagnosed in women. [1] It is the second most common cancer in women globally and 80% of these occur in developing countries. In India also, it is estimated that approximately 100,000 women develop cervical cancer each year. Cancer cervix occupies either the top rank or second among cancers in women in developing countries, whereas, in the affluent countries cancer cervix does not find a place even in top five leading cancers in women. The truncated rate (TR) in the age group 35 - 64 years in Chennai, India, is higher (99.1/100,000; 1982 - 1995) than the rate reported from Cali, Colombia (77.4/100,000, 1987 - 1991). [2] Seventy percent or more of these are Stage III or higher at diagnosis. The Population based Cancer Registry Program at Kidwai Memorial Institute of Oncology, in Bangalore, found that the observed five-year survival was 34.4% and the relative survival 38.3%.Clinical stage at presentation was the single most important variable in predicting survival. The five-year observed survival, for the stage I disease was 63.3%, for stage II - 44%, for stage III - 30.3%, and for stage IV - 5.7%. [3] The success of cervical cancer screening programs in North America and Western Europe has been the result of centralized cervical cytology screening. This is not possible in the villages of India where 58% percent of females in rural areas are illiterate, health infrastructure is mediocre, and cervical cytology is unknown. [4] Time trend analysis of a ten-year data in Bangalore, Bombay, and Madras and a four-year data in Delhi did not reveal a statistically significant decrease or increase in the incidence of uterine cervical cancer for most of the age groups. [5] Considering this as a very alarming rate, National Health managers are trying to tackle this menace by organizing cytological screening programs through Regional Cancer Centers, which are set up throughout the country. There is an urgent need for initiation of community screening and educational programs for the control and prevention of Cervical Cancer in India. [6] The Indian Council of Medical Research (ICMR) has also come forward in this effort by funding such organized cervical cancer screening programs in different parts of the country, especially HPV-related projects. However fund resources and manpower in cytology are far from adequate to organize screening programs for containing the disease. At Queen Mary′s Hospital of this university a cytology monitoring cell has been in operation since April 1971, which was funded by ICMR. Routine cytological evaluation of cervical smears was being carried out on women attending the Outpatient Department (OPD) of the hospital and till June 2005, a total of 36484 women had been cytologically evaluated. In the present communication, different risk factors related to cervical cancer, and its precursors have been investigated in detail. Also an age category has been proposed to control the disease in the Indian Population, based on our 35 years of Cytological Screening. Materials and Methods Routine cytological evaluation of cervical smears is being carried out in women attending the OPD of the Queen Mary′s Hospital, of the University, since April 1971 and till June 2005, a total of 36,484 women had been registered. For the first 20 years the screening was basically opportunistic and round about 600 cases were registered each year. In the next five years, the screening was intensified and approximately 1000 cases had been screened each year. During the last 10 years, from 1996, great emphasis was laid on the screening of symptomatic women and consequently more than 2000 cases had been registered each year. The above description brings the tally of the registered cases to more than 36000 till November 2005. The different clinical lesions were defined as follows: a) Erosion Cervix On examination, there is a bright red area surrounding and extending beyond the external os on the ectocervix, with a clearly demarcated outer edge. b) Hypertrophied Cervix The size of the cervix is enlarged. c) Suspicious and Unhealthy cervix If abnormal growth, ulcer, or vasculature is present, the cervix is clinically diagnosed as unhealthy. In all women, prior to bimanual examination, a scrape smear was taken with help of wooden spatula from the squamocolumnar junction of the cervix and fixed in absolute alcohol. The smears were stained according to the Papanicalaou technique and read by the cytologist. The cytopathological changes in the cervical smears were graded according to the WHO classification of 1973 till 1992, after which the Bethesda system of reporting cervical cytology was followed, and all the previous cases prior to 1992 were again graded accordingly, for the sake of uniformity. [7],[8] A routine cervical biopsy was taken in all High-grade Squamous Intraepithilial Lesion (HSIL) and frank carcinoma cervix cases. The four STDs namely Trichomonas vaginalis, Candida albicans, Herpes simplex, and HPV were also diagnosed in the cytology smears. Although the T. vaginalis and C.albicans were reported on the individual presence of the pathogen in the smear, the viral STDs-HSV and HPV were diagnosed on the basis of cytomorphological changes produced by them in the squamous cells, namely the ground glass appearance of the nuclei in case of HSV and Koilocytosis in the HPV infection (Condyloma). The condyloma study was initiated in March 1989. Results The Cytological findings in the cervical smears of 36484 women screened were as follows: 1. Unsatisfactory smears (Inadequate) - 2956 (8.1%) 2. Normal Smears - 13698 (37.5%) 3. Epithelial cellular changes - 17173 (47.3%) a) STD Infection - 1582 (4.3%) 4. Epithelial cellular abnormalities - 2657 (7.8 %) The grading of SIL in the 2438 cases detected was as follows: Low grade SIL (LSIL) - 1867 (5.5%) The 1867 LSIL cases comprised of 1695 cases of mild dysplasia (5.1%) and 172 condyloma (HPV) cases (0.5%). The 571 HSIL cases comprised of 536 cases of moderate dysplasia (1.5%) and 35 cases of severe dysplasia (0.1%). Cervical biopsy could be performed in 398 of the 536 cases of moderate dysplasia (74.2%), the remaining 138 cases did not return for the biopsy. The histopathology report in the 398 biopsied cases showed moderate dysplasia in only 276 cases (69.3%). The discrepancy in the diagnosis between the two procedures was thus 30.7% (122/398). This discrepancy was found due to the biopsy site not being selected under colposcopic guidance, as the instrument was not available till February 1989. This is relevant from the following findings: April 1971 - February 1989 - 42/123 (34.1%) Cervical biopsy was taken in all 35 cases of severe dysplasia and the cytology report showed compatibility with histopathology in all 35 cases. However, cervical biopsy could be performed in only 182 of the 219 cases of frank carcinoma cervix diagnosed on cytology. The compatibility between histology and cytology was 100% in these 182 cases. However, 29 fresh cases of cervical carcinoma were reported on histology. The cytology reports in these 29 cases had been inflammatory in 21 and inadequate smear in eight. The percentage of false negatives with cytology, for diagnosis of invasive carcinoma of cervix, was thus 10.3% (21/203). Different Risk factors associated with SIL and cervical malignancy detected in the present study have been analyzed in detail. The findings are summarized below. A) Age The frequency of SIL and carcinoma cervix in relation to age is shown in [Table - 1]. A progressive rise was seen in the frequency of cytopathological abnormalities with increasing age, and maximum frequency was observed in older women beyond 40 years of age.(SIL - 10.7l%, Carcinoma cervix 1.3%) B) Parity The frequency of both SIL and cervical cancer also showed a progressive rise with increasing parity [Table - 2]. However, the increase was more pronounced and statistically highly significant between para 2 and 3 ( p < 0.10). C) Age at marriage The relationship between the frequency of SIL and carcinoma cervix with age at marriage is shown in [Table - 3]. The frequency of SIL was maximum in women who were married between 21 to 30 years. This is obvious because the maximum number of smears have fallen in this age group in whom the smears were taken from five to 20 years after consummation. However the carcinoma cervix was maximum in women who married late, after 30 years. The women in this group ranged between 35 - 60 years age D) Clinical lesions on the cervix Another important aspect of the study has been testing the hypothesis of clinically downstaging the cervical cancer. For this, the frequency of SIL and carcinoma cervix was compared in 11046 women who had shown cervical lesions on clinical examination and the remaining 25408 who presented a healthy cervix. The frequency of the two cytopathologies in the two groups was found to be as follows: As can be seen from [Table - 4], the frequency of both SIL and carcinoma cervix was very high in women with clinical lesions of cervix and the difference was statistically highly significant (p < 0.01). Thus it was amply clear that clinical lesions of the cervix harbor a large number of SIL cases (14.1%) and if such women are subjected to mandatory cytological evaluation, the burden of carcinoma cervix can be reduced significantly. E) Gynecological symptoms Eight thousand three hundred and seventy four out of the 36484women registered complained of gynecological symptoms. The frequency of SIL was found to be 8.4% (708 cases) in symptomatic women as against 6.1% seen in asymptomatic women, and this difference was statistically significant ( p < 0.05). However, the carcinoma cervix frequency was almost identical in the two groups (0.5% - 0.6%). Symptom wise the SIL frequency was maximum in women complaining of postcoital bleeding (25.3%) followed by leuccorhea (8.4%). On the contrary, the frequency of carcinoma cervix was highest with postmenopausal bleeding (2.4%). F) Sexually Transmitted Diseases Trichomonal infection was found to be the most prevalent STD in the population screened, while among viral STD, HPV was seen in 0.6% of the cases. The association of these four STDs with SIL and carcinoma cervix as shown by their concomitant occurrence with the cervical cytopathologies is shown in [Table - 5]. Both viral STDs were highly associated with SIL (30-35% of cases), while HSV showed more affinity to carcinoma cervix (29.5%). Strategy for control of carcinoma cervix Based on Indian circumstances, three strategies of cytological screening have been suggested for the control of cervical cancer by Prabhakar (1992) - screening at five-year intervals, 10-year intervals, and single lifetime screening at 45 years. [9] Considering the expenditure involved and lack of cytology manpower, screening at five and 10-year intervals appears to be a remote possibility in developing countries like India. Hence single lifetime appears to be a feasible approach as a strategy for control / downgrading of cervical cancer. According to WHO Recommendations (1986), screening at 45 years of age is the most correct approach, which could detect approximately 20% of the total cervical cancer. Our experience of 35 years of cytological screening also advocates adhering to the principle of single lifetime screening, but prefers to cover the following groups in light of our findings: a) As 67.8 %of the total SIL cases and 85.8% of the total carcinoma cervix cases were seen in women of high parity (with three or more children) it was felt that this group needs to be screened at least once in their lifetime to detect any premalignant / malignant manifestation in the cervix. b) Further, the study revealed a high incidence of both cervical cytopathologies (SIL/Ca Cx) in the older women above the age of 40 years. In fact, 51.5 %of the total SIL cases and 75.3% of the total cancer cases detected occurred in this group. Hence it is felt that older women above the age of 40 years irrespective of their parity should be screened at least once in their lifetime to detect early cases of cervical cancer. Discussion Although oncogenic HPV infection has been established as a causative factor of the precursors of cancer cervix as well as their progression to higher grade and eventually to malignancy, there are some other predisposing factors which play a substantive role in the causation and progression of these lesions. We have tried to delineate these risk factors in cases of cervical dysplasia and malignancy observed during 35 years cytological screening program in 36484 women, at Queen Mary′s Hospital of this University. It was evident from the study that the frequency of cervical dysplasia showed a progressive rise with increasing age and parity. Interestingly enough, the percentage of dysplastic smears was found to be very high in women who were married between 21 - 30 years. Thus high parity coupled with increasing age appeared to play a significant role in the progression of SIL. The studies of Caslanda - Inguez and Tuledo (1998) and Lawson et al. (2000), have also pointed out the number of pregnancies as a great risk factor in the development of cervical dysplasia. [10],[11] Further, our study clearly emphasized the importance of clinically downstaging the cervical cancer, as the frequency of both SIL and carcinoma cervix was found to be very high (14.1% and 1.7%, respectively) in women showing clinical lesions in the cervix than in women with a healthy cervix (3.4% and 0.8% respectively). A previous study has also emphasized this point, [12] however, data from some other poor countries like Africa differ. [13] This study revealed slightly higher frequency of SIL, but identical frequency of carcinoma cervix between symptomatic and asymptomatic women. Hence stress should be laid on screening all women even if they are asymptomatic. However, a study displayed high frequency of SIL with postcoital bleeding and carcinoma cervix in cases of postmenopausal bleeding. Hence such women needed mandatory cytological evaluation. The study stressed single lifetime screening as a feasible strategy for control of cervical cancer in developing countries like India. The average cost of screening, as estimated by the International agency, is much higher . The average total costs per 1000 women eligible for screening were US$ 3917,US$ 6609 and US$11779, with VIA,Visual Inspection of Acetowhite Area cytology, and HPV, respectively. The cost of detecting a case of CIN2/3+ using VIA was $522 (95%Cl $429 - $652).The results suggest that more CIN2/3+ cases would be detected in the same population if cytology were used instead of VIA, and each additional case would cost US$ 1065 (95% Cl $713 - $2175.) [14] However, in the Indian setting, it could be further reduced. Based on our findings, it was felt that women of high parity irrespective of the age (with three or more children) and older women beyond 40 years of age should be screened at least once in their lifetime to detect any onset of premalignant lesion in the cervix. A previous study has also specified single lifetime screening in women between 41 and 50 years of age, but we feel that if high risk cases as defined above are screened once in their lifetime, a large number of SIL and carcinoma cervix cases could be detected early, the treatment of which would save many precious lives. [15] In other Cervical Cancer screening programs; the WHO [16] guidelines from the American Cancer Control Program [17] and the International Agency for Research on Cancer, [18],[19],[20] have suggested similar or slightly modified screening programs. However, due to the cost factor and trained manpower they are not suited for our country. A broad coverage approach would be better goal-oriented to obtain the maximum benefit from a limited cytological surveillance program. Acknowledgements The authors thank Director General, Indian Council of Medical Research, New Delhi for financing this project.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09030t3.jpg] [cn09030t5.jpg] [cn09030t2.jpg] [cn09030t4.jpg] [cn09030t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}