 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
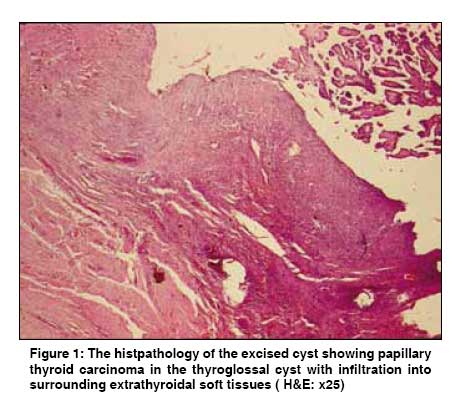
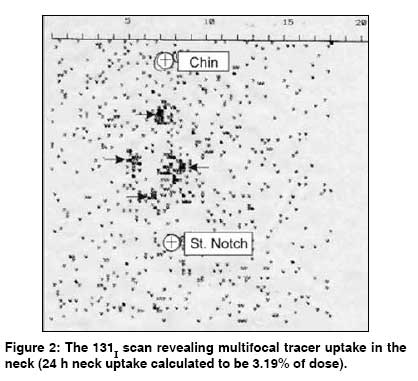
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 169-170 Letters To Editor Outcome of primary papillary carcinoma of thyroglossal duct cyst with local infiltration to soft tissues and uninvolved thyroid Basu S, Shet T, Borges AM Radiation Medicine Centre (BARC), Department of Pathology, Tata Memorial Hospital, Parel, Mumbai-400 012, India Code Number: cn09032 Sir Primary malignancy of the thyroglossal cyst (TGDC), although presently a well-established clinical entity, is relatively rare, with a reported frequency of ~1 % of all thyroglossal duct cysts. [1],[2] The most frequent histological type is papillary carcinoma (~94% of the cases); only about 6% are squamous cell carcinomas. [1] There have been few reports of synchronous papillary and squamous cell carcinoma. [3],[4] Because of its rarity, a considerable difference in opinion remains regarding the mode of management. The concept of de novo origin of primary TGDC carcinoma and excellent outcome of limited surgery in low-risk patients, in the presence of a clinically and radiologically normal thyroid gland, advocates a Sistrunk procedure only as the optimal approach in this setting. In this communication, a 45-year-old male with a papillary carcinoma of TGD Cyst with infiltration into the surrounding soft tissue in the neck is presented, who underwent a Sistrunk excision of his TGD cyst first and a total thyroidectomy and postoperative radioiodine therapy subsequently. The histpathology of the excised cyst was found to be papillary thyroid carcinoma in the thyroglossal cyst with infiltration into the surrounding extrathyroidal soft tissues [Figure - 1]. A diagnostic 131 I uptake and scan [Figure - 2] revealed multifocal tracer uptake in the neck with a 24 h neck uptake of 3.19%. In view of the age, sex, and histopathology, showing that the disease had spread into the surrounding tissues, the patient was treated with 5550 MBq (150 mCi) 131 I and was subsequently put on thyroxin supplementation. Follow-up of the whole body survey six months after residual ablation did not reveal any abnormal focal uptake in the body. The serum thyroglobulin levels in his subsequent four follow-up visits were undetectable and he was disease-free at the end of eight years. The 131- I scan revealing multifocal tracer uptake in the neck (24 h neck uptake calculated to be 3.19% of the dose) The case draws attention to the following important issues in the management of primary TGDC carcinoma: (a) The de novo origin of the disease is reiterated as a diligent search in the histological sections following total thyroidectomy, which did not yield any disease focus in the thyroid gland. The first step of optimal management will include risk assessment in the line of differentiated thyroid carcinoma, a careful pre- and intraoperative evaluation of the thyroid gland and neck for potential disease involvement that would necessitate thyroidectomy and lymph node dissection. A microscopic focus of papillary carcinoma, without cyst wall invasion, can be managed by a Sistrunk procedure. Treatment of all other TGD papillary carcinomas should include addition of thyroidectomy followed by radioactive iodine treatment, which renders the following advantages: (a) its implication for performing 131 I scintigraphy both in clinically diagnosing the inapparent disease foci as well as treating recurrence in the initial and follow-up visits, which is significantly higher in the high-risk patients, with advanced disease, (b) reliability of thyroglobulin estimation in subsequent disease monitoring overall and, (c) an excellent outcome achieved following 131 I therapy. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09032f2.jpg] [cn09032f1.jpg] |
| |||||||||

{kind=link}
{kind=link}