
|
Indian Journal of Cancer
Medknow Publications on behalf of Indian Cancer Society
ISSN: 0019-509X EISSN: 1998-4774
Vol. 46, Num. 2, 2009, pp. 170-172
|
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 170-172
Letter To Editor
Gutka or areca nut Chewer's syndrome
Chaturvedi P
Head and Neck Service, Department of Surgical Oncology, Tata Memorial Hospital, Mumbai - 400 012, India
Correspondence Address:Head and Neck Service, Department of Surgical Oncology, Tata Memorial Hospital, Mumbai - 400 012, drchaturvedip@rediffmail.com
Code Number: 09021
Sir,
I propose a new name to a well known disease entity as "Gutka syndrome or Areca Nut Chewer′s syndrome", which is highly prevalent in the Indian subcontinent. Most of the signs and symptoms of this syndrome are well known and amply reported in the literature. To my knowledge, this new terminology describing a prevalent entity has not been reported to date. Gutka Syndrome or Areca Nut Chewer′s syndrome is a combination of several well known disabilities that are directly related to chewing of areca nut (or betel nut that is the seed of the Areca palm called Areca catechu , which grows in the tropical Pacific, Asia, and parts of east Africa.) with or without smokeless tobacco consumption. This is usually seen in those chewing these products for several years. The fundamental cause of this syndrome is varying degree of fibrosis in the sub-mucosal layers and in the muscles of mastication leading to varying degree of trismus. The mucosa of these individuals is white, lacks suppleness, is extremely temperature sensitive and easily bruised. Trismus leads to typical facial and systemic features that are characteristic of chronic users. Most authors attribute it to areca nut consumption and partly to smokeless tobacco. [1] While areca nut is implicated as the cause of progressive sub-mucosal fibrosis, tobacco enhances its addictiveness and carcinogenicity. Pan, gutka, pan masala, pan mawa etc. are the popular names of tobacco and areca nut combinations. [2] Pure smokeless forms of tobacco are khaini, jarda, masheri, nas etc. Gutka is the predominant form of areca nut (with or without tobacco) consumption in most parts of India. [2] Gutka (also called gutkha, guthka) is a powdery or granular preparation of betel nut, tobacco, lime and savory flavorings. [2] It is a popular product in India and available under several dozen brand names. It is sold as small sachets that cost less than 10 cents (4 rupees) apiece. As expected, it is highly addictive and it is portrayed as a mouth or breath freshener! Consumed by millions, gutka, mawa and pan masala are important causes of high prevalence of oral pre-cancer and cancer in the Indian subcontinent. [3],[4] Typically, the addiction starts at a very young age. Because of cheapness, bright pouches, easy availability, sweet taste and forceful misleading advertisements, it is popular amongst children and adolescents. [5],[6] Signs and symptoms of submucous fibrosis, leucoplakia and erythroplakia are often seen in young adolescents. [6] Smoking is socially unacceptable in India but gutka, just like tobacco chewing, enjoys social approval. The consumption of gutka or similar products has not only been reported from Asia [7],[8],[9] but also from the western world. [10],[11]
With a decade of experience in oral surgery, I see several areca nut (with or without tobacco) chewers every day in my clinic. Over the years I have found a striking pattern in the signs and symptoms amongst these chewers The various components of this syndrome are-
General
- Usually seen in individuals who are using areca nut containing products such as gutka, pan masala, mawa, pan etc. However, I have seen this entity in some non-areca nut smokeless tobacco users as well.
- May develop within 5 years of areca nut / tobacco chewing habits. However, most people with gutka syndrome have a history of tobacco and or areca nut for more than 10 years.
- Typically affects young or middle aged persons. I have reported such abnormalities in young school children as well. [6]
- Male and female both can be affected. Because of higher prevalence of the chewing habit amongst male population, it is more common in males. [12]
- These individuals may have higher incidence of developing oral cancers. [4]
Following are the features of this syndrome-
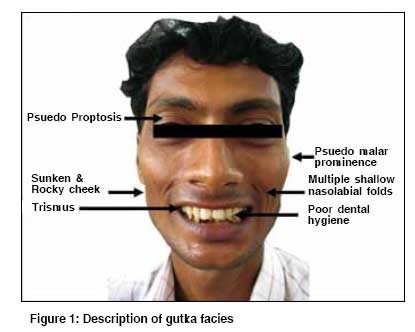
Gutka Facies [Figure - 1] :
- Sunken cheek: Due to:
- Loss of facial and buccal fat due to chronic malnutrition
- Stiffening of the soft tissue around the buccal fat that leads to loss of chubbiness and suppleness in the cheek region.
- Fibrosis of the muscles of mastication (e.g. buccinator, masseter, pterygoid etc)
- Stiff cheek - In extreme cases, the entire cheek feels hard like a bone or rock due to fibrosis of all the muscles and loss of subcutaneous fat.
- Pseudo - proptosis - Due to loss of facial, especially peri-ocular fat that gives the relative appearance of a bulging eye.
- Multiple peri-oral skin folds: When asked to open their mouths, these develop several shallow skin folds in the peri-oral area instead of a single deep naso-labial fold. This happens due to thinning of the skin consequent to loss of subcutaneous fat.
- Pseudo malar prominence due to loss of subcutaneous fat and sunken cheeks.
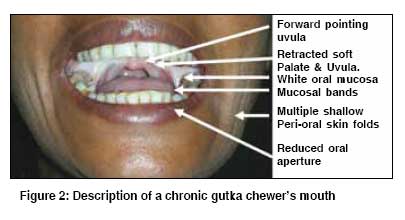
Gutka mouth [Figure - 2]:
Gutka Mouth
- Whitening of the oral mucosa - The entire lining of the mouth appears pale or white instead of normal pink color. This happens due to chronic imflammation, progressive fibrosis and strangulation of sub-mucosal vascular plexus.
- Varying degree of trismus or inability to open the mouth - Due to submucous fibrosis and formation of several sub-mucosal bands. [1]
- Reduced and stiff oral aperture - due to submucous fibrosis in the labial mucosa, the lip gets inverted. This gives an appearance of reduced size of the oral aperture.
- Poor oral hygiene - Chronic chewing causes discoloration of the teeth starting from yellow, brown or dark gray. The inter-dental gaps harbor tartar and encrustations. [13]
- Bald tongue - due to chronic inflammation the tongue becomes bald due to loss of papilla and normal mucosal architecture.
- Chronic non healing Ulcers - The mouths of such individuals may demonstrate several ulcers especially in the area of retro-molar trigone. The rest of the mucosa may also show several ulcers, and red or white patches. Most dentists are misled into biopsying these benign ulcers only to aggravate the symptoms and make the ulcers bigger. [12],[13]
- Discoloration of the commissures - In some individuals the angle of the mouth may show whitish discoloration due to repeated cycles of spontaneous injury and healing. The lip may show deep cracks and bleeding areas on forceful opening.
- Extreme sensitivity - the mucosa of such an individual is extremely sensitive to heat, cold and spice. [12],[13]
- Retracted soft palate and uvula. In these subjects, one can notice pale, retracted and stiffened soft palate.
- Forward pointing Uvula - Due to the fibrosis, the uvula may point anteriorly instead of down ward pointing.
- Unhealthy gingiva - it may show varying degree of chronic gingivitis or gingival recession.
- Unhealthy teeth - the loss of enamel makes the teeth sensitive, teeth are abnormally shaped, teeth are abnormally aligned, razor sharp teeth are common occurrence, premature loss of teeth are very common and the sugar in the product compounded with poor hygiene lead to several cavities.
- Buried last molar - The last molar teeth in such patients are usually partly buried in the adjoining buccal mucosa that leads to chronic trauma and further scarring that may worsen the trismus.
- Loss of gingivo-buccal sulcus - in most cases this space is lost due to progressive submucous fibrosis.
- Loss of tonsillar bulge - due to fibrosis the tonsillar bulge is lost in most chronic chewers.
- Reduced salivary outflow - It may happen due to fibrosis around the Stenson′s duct opening leading to it′s blockage. In severe form, parotid gland may atrophy due to chronic obstruction.
- Oral Melanosis - prdominantly seen in those who also smoke tobacco in addition to chewing.
Gutka speech
These patients have a distinct speech where the pronunciation of words that require a supple tongue and lip is difficult. Due to progressive fibrosis, the tongue and lip become stiff, resulting in alteration of speech. In those with trismus, the inability to move the jaw also affects the speech. Similarly, inability to touch the palate with a stiffened tongue also contributes to altered speech. After every few sentences, they stop and forcibly suck their saliva followed by a peculiar swallowing movement. This suck and swallow action is the result of a stiff tongue and altered swallowing mechanism.
Gutka swallowing
- Avoidance of eating in public - To avoid embarrassment due to reduced mouth opening and consequent inability to eat routine food. Moreover, the mucosa becomes extremely sensitive to hot, cold and spicy food. In extreme cases, they cannot take chewable food and survive only on semisolid or liquid food. Because of their special needs, they prefer to eat in isolation.
- Sucking and swallowing - Normal swallowing requires preparation of bolus by chewing and complex movements of the tongue against palate. Finally the tongue pushes the bolus backwards into the pharynx. In subjects with submucous fibrosis, loss of suppleness of tongue severely affects swallowing. They usually suck liquid food or their saliva due to lack of propulsive action of their tongue.
- Reduced salivary outflow - as already discussed.
- Dysphagia - though rare, the esophagus may show signs of progressive fibrosis and narrowing.
Gutka Hearing
I have seen few patients with hearing impairment probably due to fibrosis around the eustachian tube opening.
Conclusion I wish to propose this entity to give a name to a combination of several disabilities suffered by chronic areca nut chewers with or without tobacco. Most oral surgeons in Indian subcontinent are very well aware of these signs and symptoms. It is a common syndrome in a country where chewing of this combination is endemic.
References
| 1. | Tilakaratne WM, Klinikowski MF, Saku T, Peters TJ, Warnakulasuriya S. Oral submucous fibrosis: Review on aetiology and pathogenesis. Oral Oncol 2006;42:561-8. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Gupta PC. Mouth cancer in India: A new epidemic? J Indian Med Assoc 1999;97:370-3. Back to cited text no. 2 [PUBMED] |
| 3. | Gupta PC. Gutka: A major new tobacco hazard in India. Tob Control 1999;8:134. Back to cited text no. 3 [PUBMED] |
| 4. | Boffetta P, Hecht S, Gray N, Gupta P, Straif K. Smokeless tobacco and cancer. Lancet Oncol 2008;9:667-75. Back to cited text no. 4 [PUBMED] [FULLTEXT] |
| 5. | Gupta PC. Areca nut use in India. Indian J Med Sci 2007;61:317-9. Back to cited text no. 5 [PUBMED]  |
| 6. | Chaturvedi P. Precancerous lesions in oral cavity of Indian schoolchildren may hint at epidemic. Br Med J 2003;326:282. Back to cited text no. 6 |
| 7. | Khawaja MI, Shafiq M, Nusrat R, Khawaja MR. Preventing the oral cavity cancer epidemic. Asian Pac J Cancer Prev 2005;6:420. Back to cited text no. 7 [PUBMED] |
| 8. | Reichart P, Nguyen X. Betel quid chewing, oral cancer and other oral mucosal diseases in Vietnam: A review. J Oral Pathol Med 2008;37:511-4. Back to cited text no. 8 |
| 9. | Zhang X, Reichart PA. A review of betel quid chewing, oral cancer and precancer in Mainland China. Oral Oncol 2007;43:424-30 Back to cited text no. 9 [PUBMED] [FULLTEXT] |
| 10. | Changrani J, Gany F. Paan and Gutka in the United States: An emerging threat. J Immigr Health 2005;7:103-8. Back to cited text no. 10 [PUBMED] [FULLTEXT] |
| 11. | Changrani J, Gany FM, Cruz G, Kerr R, Katz R. Paan and Gutka Use in the United States: A pilot study in Bangladeshi and Indian-Gujarati immigrants in New York city. J Immigr Refug Stud 2006;4:99-110. Back to cited text no. 11 |
| 12. | Ranganathan K, Devi MU, Joshua E, Kirankumar K, Saraswathi TR. Oral submucous fibrosis: A case-control study in Chennai, South India. J Oral Pathol Med 2004;33:274-7. Back to cited text no. 12 [PUBMED] [FULLTEXT] |
| 13. | Hazarey VK, Erlewad DM, Mundhe KA, Ughade SN. Oral submucous fibrosis: Study of 1000 cases from central India. J Oral Pathol Med 2007;36:12-7. Back to cited text no. 13 [PUBMED] [FULLTEXT] |
Copyright 2009 - Indian Journal of Cancer
The following images related to this document are available:
Photo images
[cn09033f2.jpg]
[cn09033f1.jpg]
|

{kind=link}
{kind=link}