 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
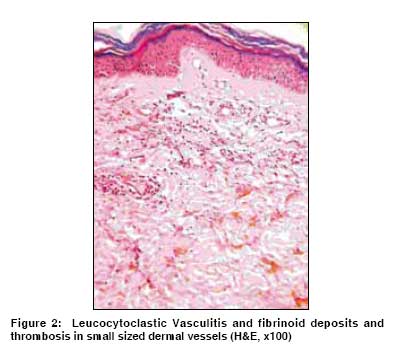
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 173-174 Letter To Editor Multiple myeloma with paraneoplastic leucocytoclastic vasculitis Jain P, Kumar P, Parikh PM Department of Medical Oncology, Tata Memorial Hospital, Dr. E. Borges Road, Parel, Mumbai-400 012, India Code Number: cn09034 Sir 53 year old male, presented to us because of gradual onset of progressively developing body aches, fatigue and multiple ulceronecrotic lesions on both lower limbs on the dorsum of foot and calf area since six to seven months. He had non specific arthralgias from the past one month. Patient had biopsy proven leucocytoclastic vasculitis. He has been evaluated in detail for the skin lesions by various dermatologists. Patient had leucocytoclastic vasculitis and was on topical steroids and anti-fungal creams. On examination, there were different sized ulceronecrotic patchy lesions with necrosis, without any pus discharge, present in the legs and feet [Figure - 1]. A Complete Blood count (CBC), renal and liver functions tests, coagulation tests, serum electrolytes, calcium, phosphorus and chest X-ray were normal. Anti nuclear antibodies (ANA), anti neutrophil cytoplasmic antibodies (ANCA) and anti double stranded (ds) DNA antibodies, cryoglobulins, HIV and hepatitis B and C panels were negative. Compliment levels were normal. ESR was 91 mm in first hour and total serum protein levels were 8.5 gm% (normal 6.4-8.3 gm %). Serum immunofixation and electrophoresis showed an "M" band in the gamma globulin zone, the concentration of which was 3 gm/dL with serum Immunoglobulin G (IgG) levels elevated at 3600 mg/dL. IgA and IgM were at normal levels. An immunoelectrophoretic study confirmed the monoclonal IgG - kappa chain peak. Urinary bence Jones were negative. Bone marrow biopsy showed a plasma cell infiltrate of 35%. Serum beta 2 microglobulins were 1.52 mg/L (Normal value was 0.83 - 1.15 mg/L). A skeletal survey revealed osteolytic lesions in the first rib, right femur intertrochantric region. Skin biopsy of the lesions showed thrombosis involving a large number of upper dermal, small-sized arteries, as well as leucocytoclastic vasculitis, with fibrinoid deposits within the capillary walls in the upper and lower dermis [Figure - 2]. Based on all above data the patient was diagnosed as multiple myeloma stage III a. The patient was treated with six cycles of vincristine adriamycin and dexamethasone (VAD) with monthly pulse of zolendronate. There was remarkable improvement in the ulceronecrotic lesions and patient symptoms. The "M" band concentration fell to 100 mg/dL. The patient is in regular follow up and is on monthly zolendronate. Paraneoplastic vasculitis is a known entity; cutaneous vasculitis is the most commonly observed paraneoplastic vasculitis. It constitutes 30 - 40% of all paraneoplastic vasculitis. [1] Most of the cases of cutaneous paraneoplastic vasculitis are associated with hematological malignancies (90%). [2] The association of myeloma with cutaneous paraneoplastic vasculitis is very rare. Only about 11 cases of paraneoplastic cutaneous vasculitis associated with myeloma were reported so far. [3],[4] Myeloma associated cutaneous vasculitis is mostly associated with IgA type but our case had Ig G type of myeloma. [3] Only two cases with predominantly ulceronecrotic lesions have been reported. Systemic involvement was present only in two cases. [3] In our case the, vasculitis improved once treatment was started in our case but skin grafting was needed as the ulcers were large and deep. [2,5] This patient′s skin biopsy showed typical features of vasculitis. [1] Immunofluorescence studies show immunoglobulin or compliment deposits in vessel walls. Vasculitis usually responds to steroids or to treatment of primary cancer and its prognosis depends on the underlined malignancy. [1] References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09034f1.jpg] [cn09034f2.jpg] |
| |||||||||

{kind=link}
{kind=link}