 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
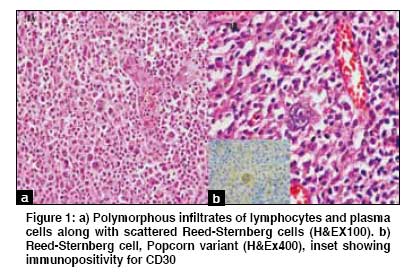
Indian Journal of Cancer, Vol. 46, No. 2, April-June, 2009, pp. 175-176 Letter To Editor Hodgkin lymphoma involving ascending colon and mesenteric lymphnodes: A rare entity Gupta D, Sharma A, Dwary A, Kark AK Department of Medical Oncology and Pathology, Dr. B. R. A. Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi, India. Code Number: cn09036 Sir, Hodgkin lymphoma (HL) characteristically presents as an enlarged supraclavicular, cervical or axillary lymph node in young adults and systemic B symptoms are seen in less than 25% of patients. Hodgkin lymphoma is a malignancy that rarely affects the mesenteric lymph nodes (< 5%) and involvement of bowel is rare. [1] We hereby describe a 45-year-old patient who presented to the Emergency Department and underwent laparotomy for acute abdomen. Prior to surgery he had a history of significant weight loss of 20 kg during the last 4-5 months and acute pain in the abdomen. A preoperative ultrasound revealed a right iliac fossa mass with inflamed mesentery. He underwent right hemicolectomy with mesenteric lymphadenectomy, in view of a preoperative clinical diagnosis of colonic carcinoma. Histopathological examination showed gross thickening and ulceration of the cecum and matted mesenteric lymph nodes. Microscopic examination revealed infiltration by Reed-Sternberg cells in the mesenteric lymph nodes surrounding the soft tissue and transmural infiltration of the cecum and appendix, suggesting HL of the mixed cellularity type [Figure 1A],[Figure 1B]. Immunohistochemistry was positive for CD 30 and negative for CD3, CD20, EMA, LCA, and CD15 [[Figure 1B], inset]. He had no peripheral lymphadenopathy or organomegaly. A postoperative contrast enhanced computed tomography scan (CECT scan) revealed multiple right iliac fossa, mesenteric, retroperitoneal, and pelvic nodes. Bone marrow examination did not reveal any lymphoma infiltration. A positron emission tomography scan (PET scan) revealed increased FDG (18F-fluorodeoxyglucose) uptake in the retroperitoneal, mesenteric, and pelvic nodes. Considering diagnosis of HL, he was started on ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) protocol. Post two cycles, the patient had significant symptom improvement and a PET scan also showed significant resolution of the disease except at the aortocaval and right mesenteric nodes. He was continued on ABVD chemotherapy for another four cycles. Post six cycles a PET scan showed an increase in the size of the aortocaval and mesenteric nodes. Considering progression on chemotherapy he was started on salvage chemotherapy with ifosfamide, carboplatin, and etoposide (ICE). He achieved complete remission after three cycles of ICE chemotherapy, documented by the PET scan. He is undergoing autologous stem cell therapy. The liver and lung are common extranodal sites involved by nodal HL, whereas, the GI tract is noted to be the most frequent site for primary extranodal HL. [2],[3],[4] Hodgkin lymphoma involving the colon with or without nodal disease has been described in literature mostly as a single case report and occasionally as part of a larger series. [5],[6],[7] Our patient had mesenteric lymph node involvement with transmural infiltration of the colon. Histology in this case was of the mixed cellularity type, consistent with the literature, suggesting that mixed cellularity histology more commonly present as a central abdominal disease, as compared to a peripheral nodal disease. Most patients present with intermittent abdominal cramps, anorexia, weight loss, altered bowel habits, and bleeding from the rectum. Although there is no uniformly accepted treatment for primary extranodal HL, most of primary extranodal GI HL reported earlier, without any nodal involvement, was treated with surgery alone. [5],[8] Our patient was treated with ABVD chemotherapy as is standard for nodal lymphoma. But he progressed on chemotherapy, which reflects the aggressive biology of these tumors. He was salvaged with three cycles of ICE chemotherapy to complete remission status and is being considered for autologous stem cell therapy. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09036f1a.jpg] |
| |||||||||

{kind=link}