
|
Indian Journal of Cancer
Medknow Publications on behalf of Indian Cancer Society
ISSN: 0019-509X EISSN: 1998-4774
Vol. 46, Num. 3, 2009, pp. 203-207
|
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 203-207
Original Article
HPV type 18 is more oncopotent than HPV16 in uterine cervical carcinogenesis although HPV16 is the prevalent type in Chennai, India
Berlin Grace VM
Department of Biotechnology, Karunya University, Coimbatore - 114, Tamil Nadu
Correspondence Address:Department of Biotechnology, Karunya University, Coimbatore - 114, Tamil Nadu
berlin@karunya.edu
Code Number: cn09044
PMID: 19574671
DOI: 10.4103/0019-509X.52954
Abstract
Context: The highest incidence of uterine cervical cancer in India is reported in Chennai. The prevalence and oncopotency are to be considered for the development of vaccines and therapeutic agents.
Aims: The aim of the present study is to analyze the prevalence and oncopotency of high risk type HPV16 and 18 in cervical lesions.
Settings and Design: This study is designed with 130 study subjects for analysis of selected types of HPV 6/11 and 16/18, in four groups, in a course of three years. The Bethesda system of classification is followed for grouping the samples, using histopathologic examination in biopsies.
Materials and Methods: The biopsy samples were collected in 10% buffered formalin and were embedded in paraffin within 24 hours, for long-term preservation. The presence of HPV types were tested by PCR using type-specific primers for HPV16 and HPV18 in the DNA isolated from the subject's biopsies. The stages of cervical lesions were identified by histopathology using the Hematoxylin Eosin stain.
Statistical Analysis Used: The data were subjected to statistical analysis, using the SPSS and INSTAT software packages for their associations and risk estimation, respectively. The Graph Pad Prism 2 x 2 contingency table was used for risk estimation and the Kruskel Wallis test was used for analysis of the associations.
Results: In the study population, the data indicated a high prevalence of HPV 16. However, during the course of study (1999 - 2003), four (66.6%) dysplasia cases with HPV 18, three (21.4%) dysplasia cases with HPV 16, and none with low-risk HPV6/11, turned into invasive cancer, within one year.
Conclusions: The observation of the study implied that HPV16 had a high prevalence in uterine cervical cancer compared with HPV18 cases. However, the development of invasive cancer from precancerous lesions was more for HPV18 infected cases than for HPV16 during the study period, which indicated the higher oncopotency of HPV type 18.
Keywords: HPV prevalence and risk, HPV 18-potent type, invasive cancer, PCR, uterine cervical lesions
Introduction
Chennai is the area with highest incidence of Squamous Cell Carcinoma (SCC) of the uterine cervix ever reported, with a Crude Incidence Rate (CIR) of 84.2 / 100,000. [1] The majority of the cervical cancer cases registered in Chennai registries are from the poor socioeconomic status, which is contrary to breast cancer incidence. The cervical cancer burden in India alone is estimated to be 100,000 in 2001 AD. [2]
Substantial evidence had been gathered for linking cervical cancer with certain genotypes of HPV worldwide. [3] Of more than 35 HPV types found in the genital tract, HPV16 accounts for 50 to 60% of the cervical cancer cases in most countries, followed by HPV18 (10-12%), and HPVs 31 and 45 (4-5% each). [4] However, the prevalence and oncopotency of specific HPV types in cervical cancer may vary with the geographic origin of the specimen. [5] Although HPV16 was identified as the most prevalent type for causing cervical lesions in many areas including Chennai, one of the metropolitan cities of India, [4],[6] this study aims to analyze the oncopotency of HPV16 among the analyzed types of HPV6/11 and HPV16/18, in progression of preinvasive lesions to invasive cancer, which is the prevalent type. The study was carried out between 1999 and 2003 in a study population of 20 control subjects and 110 cases with different grades of cervical lesions. The cases in this study population were from a poor socioeconomic status, residing in the slum areas of Chennai city.
Materials and Methods
The study subjects involved 20 control subjects with normal cervical tissues who underwent total hysterectomy due to complaints other than uterine cervical lesions such as uterine fibroids, endometriosis, and so on, and 110 cases with different grades of cervical lesions. The biopsy samples of the cases were collected from hospital outpatients who showed an abnormal cell change in the Papanicolaou (Pap) smear test, whereas, the cervical epithelium tissue of the control subjects were obtained from the surgical ward after verifying their basic screening report including the normal Pap smear test. Informed consent was obtained from controls as well as cases.
All paraffin-embedded biopsies were then histopathologically classified under the Bethesda system of classification (1988) using the Hematoxylin Eosin staining method, upon consultation with the chief pathologist. Thus, the study subjects along with their age range were grouped as follows: Group I consisted of 20 control subjects of age range 40-60 years, who underwent hysterectomy for various reasons other than cervical lesions and whose cervical tissues were found to be normal on a Pap smear test. The patients who were identified as cases with cervical lesions on Pap smear test were classified as groups II, III, and IV based on their histopathologic examination on their biopsies. The 20, group II patients were CIN 1 of age range 36-50 years, the 28, group III patients were CIN 2 and CIN 3 of age range 39-55 years, and the last group, IV, consisted of 62 invasive cancer cases of age range 42-63 years.
DNA Isolation from Paraffin-Embedded Tissues
About 10-15 sections of 10 µm size were taken using microtome in an ependorff tube and dewaxed by xylene wash. The sections were then rehydrated with 100% ethanol and 1 ml of cell lysis buffer was added along with proteinase K after centrifugation. The tubes were incubated at 55 degrees for 2 days and then the DNA was extracted as per the standard phenol-chloroform extraction, using phenol:chloroform:isoamyl alcohol (25:24:1) mixture. The DNA was then precipitated from the clear aqueous phase by adding 7.5 M ammonium acetate and 100% ice-cold ethanol. The isolated DNA was checked in 1% agarose gel for PCR to be carried out and was quantified using a UV spectrophotometer. The isolated DNA was stored at 4 o C until further use.
Polymerase chain reaction
Polymerase Chain Reaction (PCR) was carried out to examine the presence of HPV DNA using type-specific primers for both high-risk types of HPV (16/18) and low-risk types of HPV (6/11), along with the primer for β-globin, based on the methods described earlier. [7],[8] Briefly, PCR was carried out in a study population of 130 with type-specific primers from the L1 region (GCCTGTGTAGGTGTTGAGG and TGGATTTACTGCAACATTGG) for HPV 16, E1 region (GTGGACCAGCAAATACAGGA and TCCAACACGTGGTCGTTGCA) for HPV 18, L1 region (TAGTGGGCCTATGGCTCGTC and TCCATTAGCCTCCACGGGTG) for HPV 6, and L1 region (GGAATACATGCGCCATGTGG and CGAGCAGACGTCCGTCCTCG) for HPV 11, to amplify 246 bp, 162 bp, 280 bp, and 360 bp fragments, respectively, using the PCR amplification kit. A reaction mixture of 50 µl was prepared using the 1X PCR buffer with 3.5 mM MgCl 2 , 1.25 U Taq DNA polymerase enzyme, 200 µM of each of the dNTPs (dATP, dGTP, dCTP, and dTTP), 1 µM of each of the primers (Forward and Reverse), and 2-3 µg of genomic DNA per 50 µl reaction mixture. The reaction mixture without a DNA template and that with a standard DNA template of known molecular size provided in the PCR kit itself, were used as the negative control and positive control, respectively. Thirty cycles of PCR were carried out for HPV 16/18 and forty for HPV 6/11. The PCR products were stored at 4°C for further analysis.
Agarose Gel Electrophoresis
The PCR products were analyzed by electrophoresis in 2% agarose gel along with ethidium bromide. A molecular weight marker of 100 bp range was also run simultaneously to identify the molecular weight of the PCR products. The DNA bands were visualized by UV transillumination and analyzed using the gel documentation system for molecular size determination with respect to the DNA marker.
Statistical data analysis
The data were subjected for statistical analysis to find out their associations and risks, using the SPSS (version 11) package and INSTAT Graph Pad prism (to create a 2 x 2 Contingency table) and were verified by a statistician. An estimated statistic was performed to find a 10% difference between two groups. With a 95% confidence interval (a 0.05) at least 20 samples were required from each of the groups studied. Analysis, showing a confidence interval above 95% ( P < 0.05) was considered significant. In order to find out the association between HPV types and histopathologic stages, we used the nonparametric Kruskal Wallis test for independent samples as we had more than two independent variables.
Results
HPV prevalence in different histopathologic stages of uterine cervix
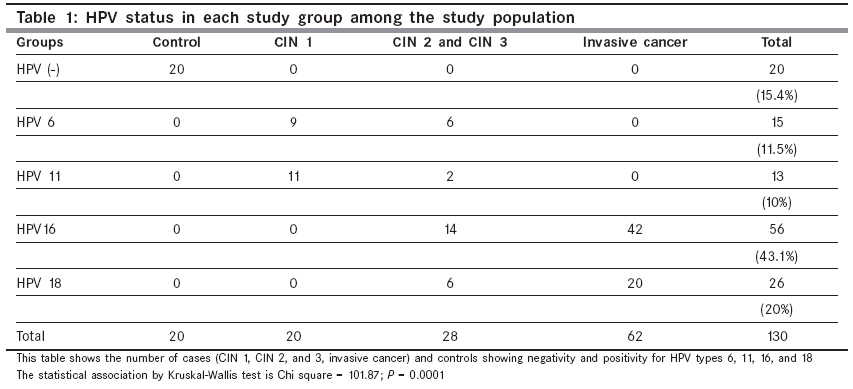
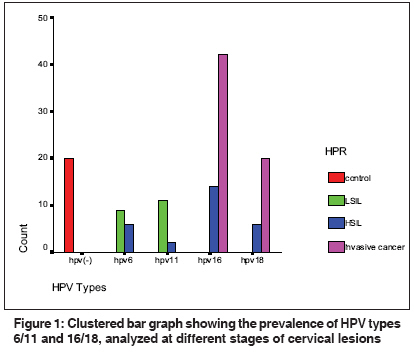
The PCR products for high-risk HPV 16/18 and low-risk HPV 6/11 were checked by agarose gel electrophoresis and the size of the products was found to be 246 bp, 162 bp, 280 bp, and 360 bp for HPV 16, 18, 6, and 11, respectively. Among the 130 study population, all the 110 cases were found to be infected with any one of the analyzed HPV types 6, 11, 16, and 18, out of which, 63.1% was with high-risk types HPV16/18. It was also interesting to note that 43.1% of this was with HPV 16 alone. All the invasive cancer cases analyzed were infected with only high-risk type HPV 16/18, 68% of which were with HPV16. The data analysis for association between HPV types (-), 6, 11, 16, and 18 and different stages of cervical lesions, using the Kruskal Wallis test, showed a highly significant association with a Chi-Square of 101.87 at the significant level of p = 0.0001. The data with the percentage of each type of HPV, analyzed, are given in [Table - 1] and [Figure - 1].
Association of high risk hpv types 16/18 in development of invasive cancer
When we analyzed the patients′ record in the raw data, it was surprising to see that four (66.6%) dysplasia cases with HPV 18 infection and only three (21.4%) dysplasia cases with HPV 16 had turned to invasive cancer within one year. However, none of the low-risk HPV6/11 infected cases turned into invasive cancer cases during that period. The first time report alone was included in this study population, whereas, the second time report as invasive cancer was excluded from our study data. The degree (percent) of association of HPV types in this rapid development of invasive cancer was little greater for HPV type 18 when compared to HPV16.
Risk of HPV types 16 and 18 in developing invasive cancer
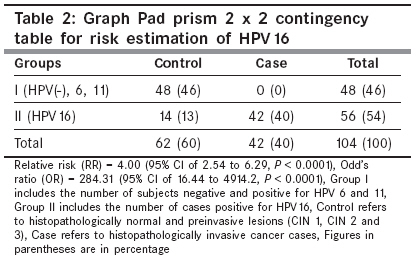
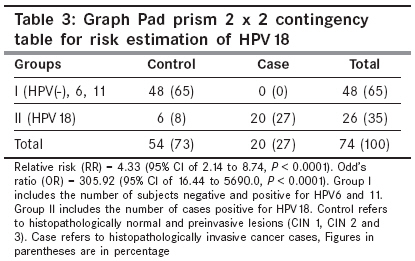
From the study population, the risk of both the high-risk type HPVs 16 and 18 was estimated separately by Fisher′s exact test using the 2 x 2 contingency table as depicted in [Table - 2] and [Table - 3]. The odds ratio for HPV 16 was found to be 284.31 with a 95% CI of 16.44 to 4914.2, which was extremely significant ( P < 0.0001), whereas, that for HPV18 was found to be 305 with a 95% CI of 16.44 to 5690.0 ( P < 0.0001), by using approximation of Woolf.
Discussion
Certain specific types of HPV were identified in cervical diseases that seem to carry different oncogenic risks and potential for malignant transformation. [9] High-risk HPV infection was demonstrated as an indicator of malignant lesions like cervical cancer, [10] with a magnitude of 84%, by Riou et. al ., and 90% by zur Hausen. [11],[12] In this study we observed a highly significant association between high-risk HPV 16/18 infection and development of cervical cancer ( P = 0.0001). Our data also showed that HPV16 was the most prevalent type in cervical lesions, especially invasive cancer, which supported the other reports on this study. However, when the data was analyzed for the risk of high-risk types HPV16 and 18 in the development of invasive cancer, the odds ratio for HPV18 was found to be little higher with a magnitude of 305.92 than that of HPV16 infection (284.31). This suggested that the people who were infected with HPV 18 were at a greater risk of getting cervical carcinoma than the people infected with the higher prevalent type, HPV 16. From this study high-risk type HPV18 might be considered as more oncopotent than high-risk type HPV16
In the study, all the invasive cervical cancer cases were infected with high-risk types HPV 16/18, and none of them were infected with low-risk types HPV (6/11), which suggested the strong association of high-risk HPV with cancer progression. The percentage of preinvasive cases that had progressed to invasive cancer within 12 months during our study period had been evaluated among the analyzed HPV types (6, 11, 16 and 18), and it was found that type HPV 18 (66.6%) had shown greater oncopotency than HPV16 (21.4%). However the oncopotency also depended on certain other factors including antiviral factors, as we had reported earlier that the reduced serum in the trans retinoic acid (ATRA) level was associated with development of cervical cancer in association with high-risk HPV types. [13] The association of high-risk types HPV 16/18 might be due to their DNA integration into the host DNA through the disruption of E2, which led to an uncontrolled production of oncogenic proteins E6 and E7, which could cause malfunction in the cell cycle regulators p53 and Rb. We had also reported previously, a highly significant association of high-risk HPV 16/18 with p53 and bcl-2 expressions in the cervical lesions. [14] Thus the study suggested that the high-risk HPV type 16 is the prevalent viral factor in cervical cancer and HPV 18 is more of the oncopotent type than HPV 16 in carcinogenesis, in Chennai, India. This study thus, necessitates the screening program for women at the age of 30, which may help to identify the women at high risk of developing invasive cancer and treat them. Prevention of cervical carcinogenesis is possible using vaccines as it is associated with HPV infection. [15],[16] Several prophylactic vaccines for HPV 16, 18, 6, and 11 are under clinical trial. [17],[18]
References
| 1. | National cancer registry programme. ICMR; Report of population based cancer surveys at Bangalore, Chennai and Mumbai: Co-ordinating unit of NCRP. Bangalore: 2000. p. 14. Back to cited text no. 1 |
| 2. | Shanta V, Krishnamurthi S, Gajalakshmi CK, Swaminathan R, Ravichandran K. Epidemiology of cancer of the cervix: global and national perspective. J Indian Med Assoc 2000;98:49-52. Back to cited text no. 2 [PUBMED] |
| 3. | Nair P, Nair KM, Jayaprakash PG, Pillai MR. Decreased programmed cell death in the uterine cervix associated with high risk human papilloma virus infection. Pathol Oncol Res 1999;5:95-103. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Bosch FX, de Sanjosι S. Chapter 1: Human Papillomavirus and Cervical Cancer-Burden and Assessment of Causality. J Natl Cancer Inst Monogr 2003;31:3-13. Back to cited text no. 4 |
| 5. | Bosch FX, Manos MM, Muρoz N, Sherman M, Jansen AM, Peto J, et al . Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) Study Group. J Natl Cancer Inst 1995;87:796-802. Back to cited text no. 5 |
| 6. | Franceschi S, Rajkumar T, Vaccarella S, Gajalakshmi V, Sharmila A, Snijders PJ, et al . Human papillomavirus and risk factors for cervical cancer in Chennai, India: a case-control study. Int J Cancer 2003;107:127-33. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Morrison EA, Ho GY, Vermund SH, Goldberg GL, Kadish AS, Kelley KF, et al . Human papilloma virus infection and other risk factors for cervical neoplasia: a case- control study. Int J Cancer 1991;49:6-13. Back to cited text no. 7 |
| 8. | Chan MK, Lau KM, Tsui Y, Wong FW, Huang DP. Human papilloma virus infection in Hong Kong Chinese women with normal and abnormal cervix-detection by polymerase chain reaction method on cervical scrapes. Gynecol Oncol 1996;60: 217-23. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Cass I, Baldwin RL, Karlan BY. Molecular advances in gynecologic oncology. Curr Opin Oncol 1999;11:394-400. Back to cited text no. 9 |
| 10. | Soloman D, Schiffman M, Tarone R; ALTS Study group. Comparison of three management strategies for patients with atypical squamous cells of undetermined significance baseline results from a randomized trial. J Natl Cancer Ins 2001;93:293-9. Back to cited text no. 10 |
| 11. | Riou G, Favre M, Jeannel D, Bourhis J, Le Doussal V, Orth G. Association between poor prognosis in early stage invasive cervical carcinomas and non-detection of HPV DNA. Lancet 1990;335:1171-4. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | zur Hausen H. Human papilloma viruses in the pathogenesis of anogenital cancer. Virology 1991;184:9-13. Back to cited text no. 12 [PUBMED] |
| 13. | Berlin Grace VM, Niranjali Devaraj S, Radhakrishnan Pillai M, Devaraj H. HPV Induced Carcinogenesis of the Uterine Cervix is Associated with Reduced Serum ATRA level. Gynecol Oncol 2006;103:113-9. Back to cited text no. 13 [PUBMED] [FULLTEXT] |
| 14. | Grace VM, Shalini JV, lekha TT, Devaraj SN, Devaraj H. Co-overexpression of p53 and bcl-2 proteins in HPV-induced squamous cell carcinoma of the uterine cervix. Gynecol Oncol 2003;91:51-8. Back to cited text no. 14 [PUBMED] [FULLTEXT] |
| 15. | Hendrix SL. Assessing Human Papillomavirus Vaccine Efficacy and Safety. J Am Osteopath Assoc 2008;108:S8-12. Back to cited text no. 15 [PUBMED] [FULLTEXT] |
| 16. | Duttagupta C, Sengupta S, Roy M, Sengupta D, Chakraborty S, Bhattacharya P, et al . Oncogenic human papillomavirus (HPV) infection and uterine cervical cancer: a screening strategy in the perspective of rural India. Eur J Cancer Prev 2002;11:447-56. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
| 17. | Paavonen J, Jenkins D, Bosch FX, Naud P, Salmerón J, Wheeler CM, et al . Efficacy of a prophylactic adjuvanted bivalent L1 virus-like-particle vaccine against infection with human papillomavirus types 16 and 18 in young women: an interim analysis of a phase III double-blind, randomised controlled trial. Lancet 2007;369:2161-70. Back to cited text no. 17 |
| 18. | Mao C, Koutsky LA, Ault KA, Wheeler CM, Brown DR, Wiley DJ, et al . Efficacy of human papillomavirus-16 vaccine to prevent cervical intraepithelial neoplasia: a randomized controlled trial. Obstet Gynecol 2006;107:18-27 Back to cited text no. 18 [PUBMED] |
Copyright 2009 - Indian Journal of Cancer
The following images related to this document are available:
Photo images
[cn09044t1.jpg]
[cn09044t2.jpg]
[cn09044t3.jpg]
[cn09044f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}