 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
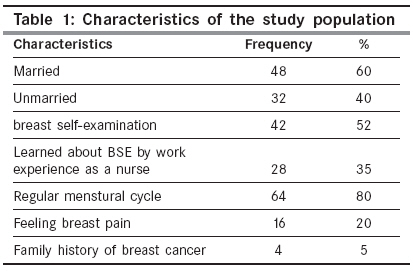
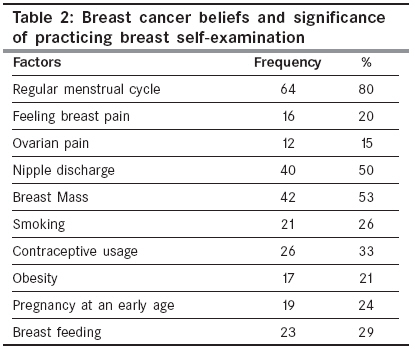
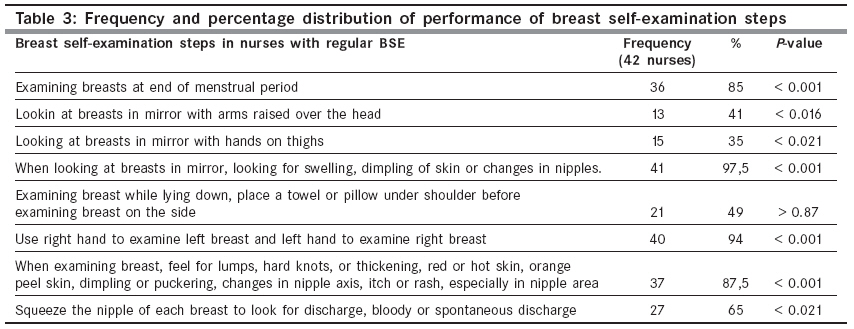
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 208-213 Original Article Breast self-examination among nurses and midwives in Odemis health district in Turkey Ertem G, Kocer A Department of Gynecology, Obstetric, Ege University Odemis School of Health, Izmir Code Number: cn09045 PMID: 19574672 Abstract Background The second leading cause of death due to cancer in Turkey is breast cancer, which accounts for 24% of female cancers.Aims: To determine the practices of nurses and midwives and their attitude toward breast self-examination (BSE). Setting and Design: The descriptive survey was conducted to determine the practices of nurses and midwives and their attitude toward BSE. It tried to cover the total population rather than sampling part of it. However, 15 nurses and midwives, where there were errors detected in their data coding papers, and who did not accept to join the study, were excluded from the study. A total of 80 nurses and midwives were included in the study group. Materials and Methods: This survey was carried out at the State Hospital, all Public Health Cabins, and Family Health Centers, in the rural area of Izmir, a city located in the western region of Turkey. The data was collected between 15 March and 1 April 2004. Statistical Analysis: The analysis included descriptive statistics, to examine the association between BSE and medical history, knowledge of BSE, and attitude toward BSE. Results: The results of the study indicated that 52% of the sample performed BSE. Approximately 35% of those who performed BSE reported that they acquired information regarding BSE during their work experience. A significant relationship was found between higher levels of work experience and BSE practice. Except for age, no significant relation was found between the sociodemographic factors and BSE practice. The sample showed a strong belief in the breast lump being the cause of breast cancer and it had a significant correlation with BSE practice. Conclusion: A positive correlation was found between nursing work experience and their practice alongside BSE medical professionals. Almost all the nurses and midwives knew how to conduct BSE, but did not prioritize practicing it. Keywords: Breast cancer, breast self-examination, nursing and midwives, knowledge, practice Introduction Breast cancer appears to be a disease of both the developing and developed worlds. It is the leading type of cancer in women. [1] Currently, cancer is the second most common cause of death (22%) in developed countries after cardiovascular diseases. This rate is similar in Turkey, increasing gradually since the 1970s, when it was only the fourth most common cause of death. [2],[3] Breast cancer is the most common cancer type and cause of death among women in many countries. Meanwhile, early discovery of breast lumps through breast self-examination (BSE) is important for the prevention and early detection of this disease. [4],[5],[6] The second leading cause of cancer death in Turkey, breast cancer, accounted for 24% of female cancers, with a crude incidence rate of 7.2 per 100,000 women, in 1999. [5] However, it has been considered that the rate has significantly increased in recent years. Statistical data from the first population-based cancer registration center in Turkey demonstrated that most women have advanced or metastatic breast cancer at the time of diagnosis. Frequency of advanced disease was higher in patients living in rural areas, and in situ breast cancer was diagnosed more often in those younger than 50 years. [7] Early detection of breast cancer by population-based screening programs would be a potentially useful approach for controlling the disease and reducing mortality, because early detection through screening is defined by the Center of Disease Control as the best defense against morbidity and mortality from breast cancer. [7] The American Cancer Society and The National Cancer Institute recommend periodical mammograms, clinical breast examinations, and monthly BSE, to detect breast cancer at an early stage. [1],[2],[6] Despite the benefits associated with it, few women regulary perform BSE and many do not even know how to perform it. There is also evidence that women are more likely to perform BSE effectively when taught by physicians or a nurse. [4],[7] Therefore, nurses / midwives are important providers of healthcare. They can train people for breast cancer prevention. It is also essential that nurses / midwives understand the importance of BSE, and believe that it can make a difference, if they expect to convince the women they teach. Unfortunately, in one study, only 19% of the nurses reported teaching BSE, where the major reason for not teaching was the belief that it was not relevant to their work. [8] On the other hand, another reason why nurses do not teach BSE to women was the lack of motivation to perform their own breast examinations. [9] Breast self-examination is an important screening measure for detecting breast cancer. There is evidence that women who correctly practice BSE monthly are more likely to detect a lump in the early stage of its development, and early diagnosis has been reported to influence early treatment, to yield a better survival rate.[10],[11] The early detection and diagnosis rate of breast cancer is considerably low among Turkish women compared to women in Western countries. This fact reflects the lack of awareness of breast cancer as well as low cancer detection and prevention activities among Turkish women. Although early detection of breast cancer can increase the survival rate, there has not been any systematic approach to increase awareness of breast cancer in Turkey. Therefore, many women miss early detection and treatment opportunities due to lack of information, knowledge, and awareness of breast cancer, as well as cancer screening practices. [1],[12],[13] However, only a few Turkish women perform BSE. According to studies, only 27-39% of Turkish women had ever performed BSE, but Secginli reported that women performing BSE once a month constituted 5.5% of the population in Istanbul.[13],[14] Health workers have a responsibility not only for improvement of public health, but also improvement of their own health. In order to improve early detection in the general population, it is very important that health workers (physician, nurse, and midwife) be able to recognize the major risk factors relevant to the development of breast cancer, be able to identify those who are at higher risk of being diagnosed with breast cancer, as well as, be able to identify symptoms associated with breast disease. Moreover, the performance of health workers is important because it can be linked to womens′ breast cancer screening in society. Additionally, women in the general population are likely to emulate the healthcare behavior of health workers, believing that they are setting proper healthcare examples. [15],[16] Nurses and midwives are ideal health professionals who can increase public knowledge of breast cancer and encourage the practice of monthly BSE. [9] They are increasingly involved in providing information and advice to women who are concerned about their risk for breast cancer. Counseling about breast cancer risk, however, may be complicated by the difficulties in understanding the risk estimates, probabilities, and the relative importance of breast cancer risk factors. [14] In Turkey, the midwives who work in primary healthcare also educate women about this subject, by undertaking house visits, which aim to inform the public about the early diagnosis of diseases like cancer. Nurses can combine their knowledge of health services to educate women about breast cancer risk factors and available breast cancer screening services and practices. [17],[18],[19] Thus, nurses and midwives should first be aware of their risk for breast cancer and of the advances in breast cancer screening. Risk perception is a significant component of the awareness of breast cancer risks. The aim of this study was to investigate the knowledge and practice of BSE and factors influencing its compliance among nurses and midwives. Materials and Methods This descriptive study is carried out at the State Hospital, all public Health Cabins and Family Health Centers in the rural area of Izmir, a city located in the western region of Turkey. The data was collected between 15 March and 1 April, 2004. A total of 114 nurses and midwives work in the rural area of Izmir. It tried to cover the total population rather than sampling part of it. However, 15 nurses and midwives, where there was error detected in their data coding paper, and who did not want to join the study, were excluded from the study. A total of 80 nurses and midwives were included in the study group. The survey was conducted on a voluntary basis. Before answering the questionnaire, all subjects, who participated voluntarily, were given instructions on how to fill it out, and the completed questionnaire was placed annonymously in a collection box. All potential subjects were informed about the research and it was made clear to them that participation was voluntary, that is, they were being invited to participate. The questionnaire was developed by researchers and designed to provide a description of the knowledge and practice of the performance of BSE. The sociodemographic factors, medical history, and interrelationsips between these variables, knowledge of breast cancer, attitudes toward BSE, and questions regarding the practice of BSE were also included. The data collected were entered and analyzed using SPSS-11.0 for Windows. Descriptive statistical methods for each question were carried out according to the different demographic data on the collection of respondents. Statistical evaluation was accomplished using the Pearson chi-square test, to test the relationship of sample characteristics and categorical variables. A P value of less than 0.05 was regarded as significant. The purpose of the investigation was explained to the participants and a verbal informed consent was obtained. Furthermore, all study participants were told that they had the right to withdraw from the investigation at any time and that all information would be kept strictly confidential. The required approvals were obtained from the governorship, National Health Ministry, and the management of the relevant Healthcare Centers. Results The age range was 20-40 years with a mean of 33 years and BMI was 26. There were more married women (60%) in the study. The results of the study indicated that 52% (42) of the sample performed BSE and 32% (12) performed it regularly. Only 8% (8) of the subjects were having a positive family history of breast cancer and 80% (64) showed regular menstrual cycle. Out of the total sample, 20% (16) of the nurses reported pain in their breasts [Table - 1]. A significant relationship was found between higher levels in nursing work experience and BSE practice, as 70% of the subjects believed that the presence of masses (breast lumps), family history of breast cancer, and nipple discharge were the causative factors of breast cancer. Eight subjects (10%) believed that the use of contraceptives, smoking, direct sun exposure, ovarian pain, consumption of fatty foods, and obesity were the cause of breast cancer [Table - 2]. The most frequently endorsed steps in BSE were examing the breasts in front of a mirror or examing breasts while lying down and feeling for a lump or hard knots, nipple discharge, or breast thickening. The least frequently endorsed step was looking at the breasts in the mirror with hand on thighs. Overall, the majority of subjects knew most of the recommended steps [Table - 3]. Discussion The midwives and nurses, who work in primary healthcare services, play an effective role in informing and advising women about BSE and also in changing their BSE-related behaviors, for early detection of breast cancer. Therefore, early detection of breast cancer executed by the midwives and nurses, who play an active role in improving public health, may be effective in increasing the awareness in women and in directing women through early detection. The studies researching the problems encountered by midwives during the BSE training are limited (Budden, 1998), and furthermore, there is no such study in Turkey. The discussion of the findings will also be limited. In addition, the study has been carried out with nurses and midwives because the health workers are responsible for the training of BSE at primary Healthcare Centers in Turkey, and also midwives are assigned by Ministry of Health to make home visits twice a year and to teach BSE (2004). [5],[9] In this study it was found that the percentage of those that perform regular BSE was rather low (52%). Likewise, a study by Norwegian female physicians, Rosvold et al . (2001), found that only 25.6% of the female workers performed monthly BSE, and a different Turkish study by Çavdar et al. (2003), of female physicians and nurses reported that 25% of those studied, performed regular BSE. [20],[21] In contrast to our study result, Haji-Mahmoodi et al. (2002), found that only 6% of the female healthcare workers in Tehran performed BSE monthly. [22] However, our study results were lower than results of the previous studies.[8],[23],[24],[25] In a study of 32 African-American nurses and 78 Caucasian nurses, Foxall et al. (1998), found that 42% of the African-American nurses performed BSE monthly, but only 20% of the Caucasian nurses did. [8] Karahan et al. (2002), reported that 87% of the Turkish nurses performed BSE, but the percentage of individuals performing this regularly was 49%, while Lee (2003), determined that approximately 40% of the Korean nurses performed BSE. [23],[24] Aydin and Isikli (2004), concluded that only 28.6% of the Turkish midwives and nurses working in protective health services performed BSE. [25] When compared with the results of the studies on women who were not employed in healthcare, we note that rates of regular BSE performance are higher in healthcare workers as compared to non-healthcare workers. [14],[26],[27],[28] To date, the etiology of breast cancer is uncertain and adequate primary prevention is not possible. Thus, early detection measures remain the first priority. More than 50% of the total breast cancer diagnosed annually is found in premenopausal patients, creating the need to initiate breast cancer screening programs in this population. These measures include BSE, which is inexpensive, noninvasive, involves little time and physical energy, is simple and does not depend on professional help. However, the effectiveness of BSE remains controversial. It is argued that a significant number of women find masses when they are bathing or dressing, and BSE once a month may contribute to a woman′s heightened awareness of what is normal for her. Various factors influence recommendation. However, in one study, it was shown that 81% of the women first noticed the symptoms themselves. [29] The evidence of primary cancer prevention is slowly growing; its strategies cannot yet be implemented in clinical prevention programs, therefore, secondary prevention and early detection of cancer remains the main focus for reducing breast cancer mortality. This is especially true because of the proven relationship between mortality and the size of the primary tumor as well as the status of the axilla. Thus, one may argue that if women find most breast cancer themselves, as it has occurred in our study, (about 37 nurses felt a sort of self-awareness of breast etiology or abnormality during their study time course), they may worry about other help. Normal breast tissue is present in both males and females of all ages. This tissue responds to hormonal changes, and therefore, certain lumps can come and go. Breast lumps may appear at all ages: infants may have breast lumps related to estrogen from the mother, young girls often develop breast buds that appear just before the beginning of puberty, teenage boys may develop breast enlargement and lumps because of hormonal changes, which are considered a normal variation of breast tissue. Fibroadenomas are noncancerous lumps, and similar to fibrocystic disease of the breast, they occur most often during the reproductive years and the only means of definitive diagnosis is by taking a biopsy; other types of lumps might be: milk cysts, lipomas, or papillomas. Furthermore, treatment of a breast lump depends on the cause. It is very important for self carefulness to be able to recognize the signs of their illness BSE is and that should be perfect nurses. As they have knowledge of the clinical signs of breast cancer and of the examination tecnique; nurses can promote monthly BSE, especially among married women. Moreover, they can do it themselves without consulting a physician. Furthermore, they are especially aware of the importance of early detection of breast cancer for successful treatment. It has been shown that confidence in one′s BSE ability is strongly correlated with BSE practice in the general population. [9],[22] In one study, Budden reported that 96% of nursing students performed BSE during a year, but only 46% had practiced regularly, once a month, and 65% of the primary health nurses were aware of early detection.[9] Lee EH, reported that, 40% of the nurses had performed BSE. [23] Haji-Mahmoodi et al. , reported from across a sectional study of female healthcare workers that more than 70% of the subjects had a knowledge of BSE and also strongly believed in its beneficial effects, but only 6% of them performed BSE regularly. [22] It is well documented that beliefs and behavior surrounding breast cancer vary with several factors, such as, ethnicity, age, education, socioeconomic status, and inherited genetic mutations. Other factors that increase breast cancer risks include a long menstrual history (menstrual periods that started early and / or ended late in life), obesity after menopause, recent use of oral contraceptives, postmenopausal hormone therapy, never having had children or having the first child after age 30, ethnicity characteristics, exposure to radiation, or consumption of one or more alcoholic beverages per day. Similarly, some studies have reported that less than half of their study groups actually practice BSE monthly.[6],[9],[22],[30] The finding in this research that 5% of the participants had a history of familial breast cancer is consistent with the literature. Most physicians and nurses with a familial history of breast cancer performed BSE, however, the researchers expected all healthcare professionals who were educated on the subject to perform BSE. Our study showed that there was a strong belief that breast mass was a causative factor of breast cancer, which was reflected in its significant correlation with BSE practice. The result of this study suggests that for nurses and midwives, if more emphasis of BSE occurs in the work place and in undergrauate and postgraduate courses, teaching of BSE to clients may increase. Also, the provision of BSE educational programs is necessary to increase the nurses′ knowledge, confidence, performance, and teaching of BSE. Further research is recommended, using a larger sample size of midwives and nurses including the cost effectiveness of designing and implementing preventive care. This study had several limitations. First, there was a lack of pertinent literature on similar prior studies on health beliefs and mammography screening for early detection of breast cancer in women, especially inclusive of female health workers, conducted in Turkey. Thus, the study was limited in its comparison of some aspects of screening behaviors and health beliefs of participants. Additionally, since this study was carried out only in Izmir, Turkey, these results could not be generalized to all Turkish female health workers. Future studies were needed, using larger samples, in several healthcare centers in different regions of Turkey. Conclusions These results can be considered highly important, as nurses and midwives working in public health can effectively guide women for the early diagnosis and treatment of breast cancer. Consequently, nurses can consider belief factors in training to early detection of breast cancer and also nurses′ educational practices can more successfully reach the purpose of dealing with the early detection of breast cancer. The results of this study demonstrate that although nurses and midwives have a knowledge about breast cancer screening behavior, such as BSE, the rates of performance are not adequate. It is therefore recommended that to increase rates of regular breast cancer screening behavior, mass health protective programs be conducted, especially for female health workers who undertake the responsibility of raising breast cancer prevention and awareness in society. In this manner, nurses and midwives can perform breast cancer screening regularly and periodically. The result of this study shows that positive health beliefs are effective in stimulating the performance of BSE in nurses and midwives. This result also shows that additional studies are needed to investigate the relation between health beliefs. The study findings cannot be generalized to include all midwives and nurses in Turkey. Acknowledgments The authors acknowledge the interest and participation of the nurses and midwives, and the authorities of the sampled health centers, for permitting them to carry out the study.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09045t1.jpg] [cn09045t3.jpg] [cn09045t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}