 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
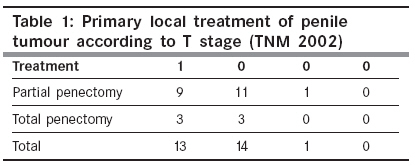
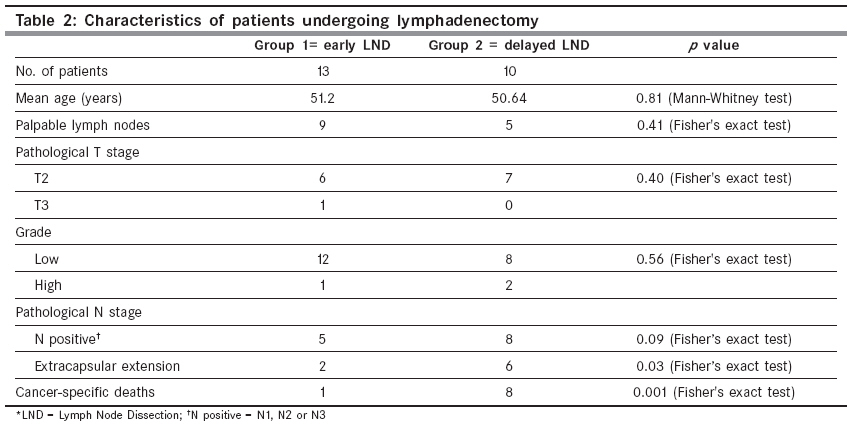
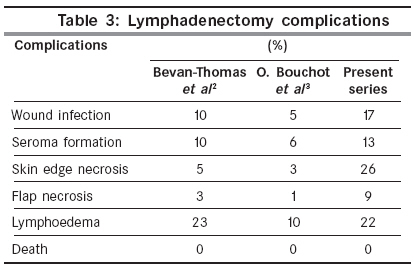
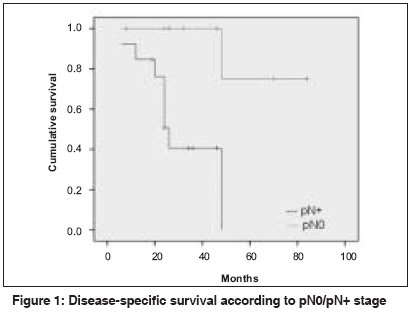
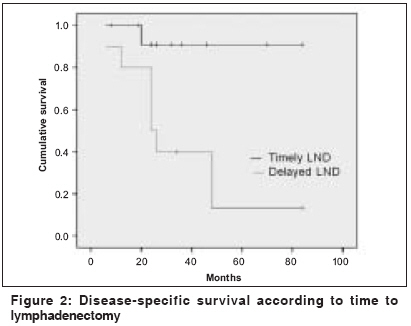
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 214-218 Original Article Impact of delay in inguinal lymph node dissection in patients with carcinoma of penis Gulia AK, Mandhani A, Muruganandham K, Kapoor R, Ansari MS, Srivastava A Department of Urology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow Code Number: cn09046 PMID: 19574673 Abstract Aim: To study the impact of delay in inguinal lymph node dissection (LND) in patients with squamous cell carcinoma of the penis, who have indications for LND at the time of presentation. Keywords: Delayed, lymphadenectomy, penile cancer Introduction Penile cancer is more common in India as compared to Western populations. The age-adjusted incidence rate of penile cancer in India ranges from 0.8 to 1.8 per 100,000. [1] Due to fear, ignorance, and embarrassment patients neglect the penile tumor for months before presenting to a physician. Many of our patients are of low socioeconomic status and never attend the follow-up after local therapy of the penile tumor. Quite a few of these present late with inoperable regional lymph node (LN) metastases, thereby missing the opportunity of a cure. This study analyzes the impact of delayed LND on the outcome of the disease.Materials and Methods The clinical records of 32 patients with squamous carcinoma of the penis treated at our institute between January 2000 and June 2008 were reviewed for age, mode of presentation, local therapy, LN management, and histopathological details. Patients with distant metastases at presentation (two) and those with incomplete records (two) were excluded. Complete records were available for 28 patients. Mean age at diagnosis was 52.1 ± 12.8 years. The penile lesion was present for a mean duration of 8.5 ± 5.8 months before the patient sought medical attention. Six patients had already received local therapy of the penile tumor before being referred to us. Primary tumor location was glans (21), foreskin (three), corona (two), and penile shaft (two). Mean tumor diameter was 3.26 ± 0.88 cm. Preoperative evaluation included clinical assessment of the external genitalia and inguinal LN. Imaging with computed tomography (CT) was used to assess the regional LN status and / or distant metastases, in the presence of a large inguinal lymph nodal mass. Pathological staging and grading of the tumor and LN or distant metastases were assigned according to the 2002 TNM system common to the International Union against Cancer and American Joint Committee against Cancer. Decision to do LND was based on the assessment of risk factors for nodal metastases. Risk factors for nodal metastases were - persistent inguinal LNs after antibiotic treatment, penile tumor stage T2 or greater, and high-grade penile cancer. Patients with any one or more of the above risk factors were advised LND. Patients with none of the risk factors were kept on surveillance. Of 28 patients, five were kept on surveillance and 23 patients underwent LND. Patients undergoing LND were grouped into two, based on the time between surgery for the primary lesion and inguinal LND. Group 1 patients had LND within six months, and group 2 had it more than six months after treatment of the primary. There were 13 patients in group 1 and 10 in group 2. The mean time for LND in groups 1 and 2 was 1.7 (range 0-6 months) and 14 (range 7-24 months), respectively. The reasons for delayed LND were physician- and patient-related factors. Few patients were initially treated outside our institution and management of inguinal LN was neglected. Other patients, despite being advised LND, preferred to delay their treatment for personal or financial reasons. Follow-up of patients included clinical assessment of the penile stump and regional LN, and imaging studies as needed, at regular intervals. The Mann-Whitney test and Fisher′s exact test were used for univariate comparison. Survival was calculated from the time of initial presentation. Survival analysis was done by the Kaplan-Meier method and the Log Rank test, with p < 0.05 considered statistically significant. All statistical analyses were performed using commercially available SPSS software (v16.0, SPSS Inc, Chicago, IL, USA). Results The primary local treatment given according to the stage of disease is shown in [Table - 1]. No patient developed local recurrence at the mean follow-up of three years (6-84 months). Primary LN management consisted of surveillance or regional LND. Of five patients (18%) on surveillance, four patients (80%) had no nodal recurrence at the mean follow-up of 46 (22-84) months, while one patient (with pT1 tumor), who was not regular on follow-up, had returned with a large (> 4 cm), palpable LN, 18 months after surgery of the primary lesion. This patient is receiving neo-adjuvant chemotherapy. Of 23 patients (82%) who had bilateral LND, 17 had palpable inguinal nodes at presentation. The pathological penile tumor stage was pT1 in nine, pT2 in 13, and pT3 in one patient. On a final histopathological examination (HPE) of LND specimens, 10 patients had pN0 disease and 13 patients had lymph node metastases. Of 13 pelvic LN dissections, only three patients had pelvic LN metastases. All three of these patients had inguinal LNs more than 4 cm in diameter. Three of our patients had large (> 4 cm) inguinal nodal disease at presentation, for which cisplatinum-based neoadjuvant chemotherapy was given. In none of the patients could the disease be downstaged. Four patients received cisplatin-based adjuvant chemotherapy; the indication being - extracapsular extension of LN metastases (three patients) and pelvic LN metastases (one patient). Groups 1 and 2 were similar with regard to age, T2-stage, grade, and palpable LNs [Table - 2]. Of 13 patients in group 1, 12 were alive, with no recurrence of disease at a mean follow-up of 37 months (range 8-84 months). One patient died due to distant metastases, 13 months after inguinal LND. Of ten patients in group 2, only two were alive at the mean follow-up of 58.5 (33-84) months. The difference in cancer-specific mortality was significant ( p 0.001). Of the eight patients who died, five died of locoregional recurrences and three of distant metastases. In this series, skin edge necrosis (which healed secondarily) occurred in 26% of the cases. Skin flap necrosis requiring application of skin grafts or myocutaneous flaps was seen in 9%. Lymphedema developed in 22% of our patients, which was managed with conservative treatment. Complications associated with LND are compared with two contemporary series in [Table - 3]. [2],[3] The five-year cancer-specific survival in pN0 and pN+ disease was 75 and 41%, respectively, ( p = 0.003) [Figure - 1]. Delay in LND affected the survival significantly. The five-year cancer-specific survival rates for early and delayed LND were 91 and 13%, respectively, ( p = 0.007) [Figure - 2]. Extracapsular extension of nodal metastases were found in six of 10 (60%) patients who underwent delayed LND, and in two of 13 (15%) who underwent early LND ( p = 0.03) [Table - 2]. Discussion Primary therapy of penile cancer should aim at providing excellent local control with a cosmetically and functionally acceptable result. The majority of our patients were treated with partial penectomy. None of the patients developed local recurrence. In a series of 257 patients reported by Lont et al. , the local recurrence rate was 10% in the group treated with penile amputation. [4] Lymph node involvement is the single most adverse factor affecting the survival of patients with carcinoma of the penis. [5] Primary regional LND is an effective treatment in patients with inguinal nodal metastases. LND alone has been reported to be curative in 75% of patients with one or two involved inguinal nodes, and has cured 20% of patients with pelvic nodal metastases.[6] In the present series LN metastases has significantly affected the survival of our patients, with a five-year cancer-specific survival of 75% in a node-negative disease and 41% in those with positive nodes ( p = 0.003). Lymph node metastasis is the single most important prognostic factor in penile cancer. Early resection of clinically occult LN metastases has been reported to improve survival as compared to delayed LND, which is done once nodal metastases become palpable. [7],[8] A proactive approach to inguinal LNs is a crucial step in the management of carcinoma of the penis. Chemotherapy, either adjuvant or neo-adjuvant, has not been of much help in improving the survival. [9] Some patients continue to present with locally advanced disease, with fixed inguinal nodes. Three of our patients had fixed inguinal nodal disease at presentation, for which cisplatinum-based neoadjuvant chemotherapy was given. In none of the patients, could the disease be downstaged. There are only a few reports in literature evaluating neoadjuvant chemotherapy in this setting. In one of these studies, Leijte et al. reported complete response in two and partial response in 10 of 20 patients. [10] Neoadjuvant radiotherapy has also been used as a potential modality to shrink nodes larger than 4 cm. [11] This study has some limitations. It is a retrospective study, and as our center is a tertiary-care facility, there is an element of referral bias. Because of the rarity of penile cancer, a centralized referral system would be the best way to improve survival. Two of our patients had inguinal LND at the time of partial penectomy, as they received antibiotics while waiting for the histopathological report after an incisional biopsy. This was not associated with any untoward effects of surgical site infection. The need for antibiotics in assessing inguinal nodes on presentation has been questioned. [12] There are reports of penectomy and inguinal LND being performed simultaneously, with no additional morbidity. [13],[14] Proper awareness among primary physicians, patients, and urologists, about the significance of timely inguinal LND would change the way this disease is being treated in our country. Conclusions A significant proportion of our patients come from a rural background with no formal education, and ensuring a regular follow-up with some of them is problematic. When compliance with follow-up is suspect, patients with high-grade or stage (≥ T2) tumor are better served by partial or total penectomy and inguinal LND during the same hospital admission or as early as possible. In any case, LND should not be delayed for more than two months.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09046t1.jpg] [cn09046t3.jpg] [cn09046t2.jpg] [cn09046f1.jpg] [cn09046f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}