 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
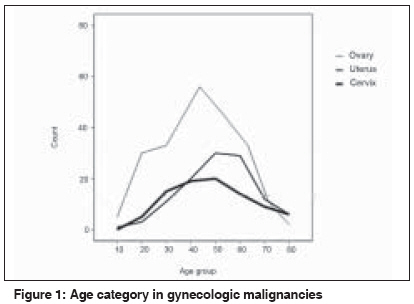
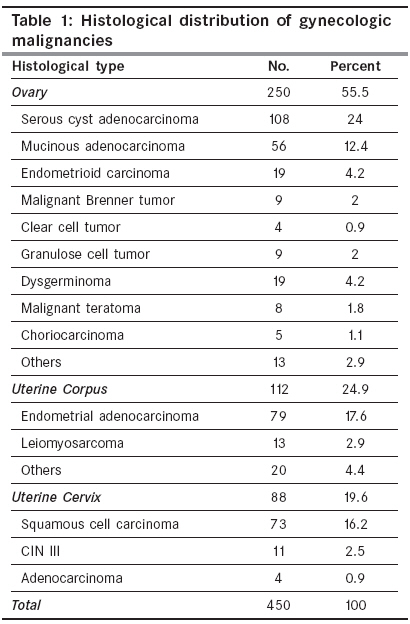
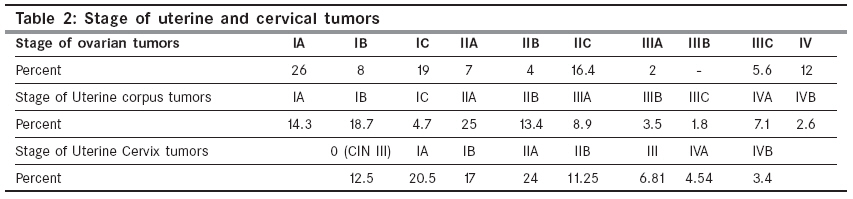
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 226-230 Original Article Assessment of gynecologic malignancies: A multi-center study in Tehran (1995-2005) Momtahen S, Kadivar M, Kazzazi AS, Gholipour F Department of Pathology, HazratRasool-e-Akram Hospital, Iran University of Medical Sciences, Tehran Code Number: cn09048 PMID: 19574675 Abstract Objective: The observed differences in cancer incidence are mainly due to different individuals and social risk factors. This study aims to demonstrate the characteristics of female genital malignancies according to the pathological records in Tehran, Iran.Materials and Methods: In this cross-sectional study, all records of pathological specimens categorized as ovarian, uterine corpus or uterine cervix cancers from 1995 to 2005, in five teaching hospitals in Tehran, were studied. Age, marriage, parity, menopausal status, smoking, oral contraceptive usage, pathological staging, and histological grading were reviewed by a trained general practitioner. SPSS 14 was used for statistical analysis. Result: Mean age (SD) at the time of diagnosis was 50 (15). Fifty-nine percent of ovarian, 33.9 and 47.7% of uterine corpus and uterine cervix malignant patients were premenopausal. About 90% of all were nonsmokers and 82.7% were multiparae. Various types of gynecologic malignancies included ovarian (55.5%), uterine corpus (24.9%), and uterine cervical cancers (19.6%) were diagnosed. In tumors of the uterine corpus and uterus cervix, the most frequent stage of diagnosis was stage IIA. Conclusion: Ovarian cancer was the most frequently occurring gynecologic tumor. Although distribution of age in ovarian cancer was similar to that mentioned in the literature, occurrence of the cancer was more frequent in the premenopausal state. Keywords: Epidemiology, gynecologic malignancies, Iran, pathological reports Introduction Genital tract malignancies are one of the most important diseases among women. Uterine Corpus cancer accounts for 6% of all cancers in women. Ovarian cancer is the second most common gynecologic malignancy, but the most common cause of death among women with gynecologic cancer. [1] Uterine cervical cancer, is a major health problem, with a 75% decrease in the incidence over the past 50 years in developed countries, although it is still the second most common cause of cancer-related morbidity and mortality among women in developing countries. [2],[3] Developing countries are hoping to be on the threshold for decreasing gynecologic malignancies and increasing survival. Assessment of the incidence and prevalence is the first step in this process. We designed this study to establish a nationwide registry, to provide a relative frequency of female genital tract malignant tumors and to explore the various histological types and characteristics of these patients in our society.Materials and Methods In this cross-sectional study, all records of pathological specimens categorized as uterine corpus, ovarian, and uterine cervical cancers from 1995 to 2005, in five teaching hospitals in Tehran, were studied. To improve the representativeness of the samples, we avoided studying known cases from referral centers. It means that all the cases we assessed in each hospital had been diagnosed for the first time in that mentioned hospital. Thus, we have excluded the known cases, which had been diagnosed in other centers by different pathologists and referred for more evaluation and treatment. Vulvar and vaginal malignancies were excluded from this study. With regard to International Federation of Gynecology and Obstetrics (FIGO) classification of uterine cervix neoplasm, stage (0) is called carcinoma in situ (CIS) or cervical intraepithelial neoplasis (CIN) grade III. Although CIN III is a precancerous lesion, it has the same meaning as stage 0 in FIGO classification, so we have included these cases in our assessment. [4] The cases were histologically classified according to the World Health Organization (WHO) typing of gynecologic tumors. [5],[6] Data concerning age, marital status, parity, menopause, smoking and oral contraceptive pill (OCP) consumption, stage of tumors according to FIGO, [4] and histological grade according to WHO classification, [6] were collected and statistically analyzed by SPSS version 14. Results Of the 450 studied cases, the highest percentage was from ovarian cancer (55.5%), followed by malignancies of uterine corpus (24.9%) and uterine cervix (19.6%). The average age (SD) of diagnosis was 50 (15). Mainly the distribution range of age was (48-52), (58-62), and (48-52) for ovarian, uterine corpus, and uterine cervix malignancies, respectively. [Figure - 1] shows the distribution of age category in different types of gynecologic cancers. The incidence of ovarian tumors increase in the first and second decades of a patient′s life more rapidly than the uterine and cervical malignancies and peak at fifty years, while the incidence of uterine cancers rise slowly to the fifth decade and then decrease. Cervical malignancies are more common during the third and fourth decades of life. Most of the cases (94.2%) were married. Ten, 5 and 2% of the patients with ovarian, uterine, and cervical malignancies were not married. About 50% of the total was postmenopausal. Fifty-nine, 33.9, and 47.7% of the patients with ovarian, uterine corpus, and uterine cervix malignancies were premenopausal. Most of the women (82.7%) with gynecologic cancer had more than one pregnancy during their lives. Twenty-seven, 9.8%, and 5% of patients with ovarian, uterine corpus, and uterine cervix malignancies were nulliparae (no childbearing). About 10% of the total had a history of using OCPs. Four percent of the patients with ovarian, 22.3% with uterine corpus, and 7.9% with uterine cervix malignancies had this history during their reproductive life. About 90% of all were nonsmokers. Seven, 10.8, and 19.3% of the patients with ovarian, uterine corpus, and uterine cervix malignancies had a history of smoking during their life. Among uterine cervical tumors, smoking was mostly reported from Squamous cell carcinoma (SCC) rather than adenocarcinoma cases (83% vs. 5%). Based on WHO′s histological classification, we found surface epithelial-stromal tumors (78.4%), germ cell tumors (12.8%), sex cord-stromal tumors (3.6%), and others (5.2%), as different types of ovarian cancers. [Table - 1] shows the histological distribution of gynecologic tumors among all cases. Serous cyst adenocarcinoma (55.2%), mucinous cystadenocarcinoma (28.6%), endometrioid carcinoma (9.6%), malignant Brenner tumor (4.5%), and clear cell tumor (2.1%) were assessed as different subtypes of surface epithelial-stromal tumors. All the sex-cord tumors were defined as granulosa cell tumors. Three different types of germ-cell tumors included dysgerminoma (59.4%), malignant teratoma (25%), and choriocarcinoma (15.6%) were assessed additionally. Other tumors of the ovary included undifferentiated tumors (69.3%), and malignant lymphomas of the ovary (30.7%) were assessed separately. Endometrial adenocarcinoma (70.5%), Leiomyosarcoma (11.7%), and other types (17.8%) as different types of uterine corpus carcinomas, and squamous cell carcinoma (83%), CIN III (12.5%), and uterine cervix adenocarcinoma (4.5%) as different types of uterine cervix malignancies were evaluated additionally. The mean age (SD) of diagnosed endometrial adenocarcinoma, 57.7 (13.1) was a little more than the mean age (SD) of diagnosis leiomyosarcoma, which was 50.6 (9.8). The mean age (SD) of diagnosis SCC of the cervix, 53.1 (15.9) was similar to cervix adenocarcinoma, 52.2 (23.7), but it was more than the mean age (SD) of diagnosis CIN III, 48.5 (15.5). Most of the tumors of the ovary and uterine cervix were diagnosed as well-differentiated or moderately-differentiated tumors, (36%) and (37%), respectively; however, most of the uterine corpus carcinomas were diagnosed as well-differentiated tumors (45%) followed by (27%) moderately-differentiated and (7%) poorly-differentiated. [Table - 2] shows the staging of tumors. Both uterine corpus and uterine cervix cancers were mostly diagnosed in stage IIA. Ovarian tumors were also mostly diagnosed in low stages (stage IA). Discussion Cancer is a major public health problem all over the world. When deaths are aggregated by age, cancer has surpassed heart disease as the leading cause of death for those younger than age 85, since 1999. [1],[7] The incidence of gynecologic malignancies is highly dependent on age; endometrial cancer usually occurs in postmenopausal women (mean age, early 60s). However, it has also been reported in women younger than 30 years of age. [8] Most women with epithelial ovarian cancers (EOC) are diagnosed between the ages of 40 and 65. [9] The overall risk of malignancy of an adnexal mass in premenopausal and postmenopausal women is 6 - 11 and 29 - 35%, respectively. [10] Mean age at diagnosis of invasive cervical cancer is 47 years in the United States. From 1995 to 1999, the US incidence of cervical cancer in girls under age 20 was 0/100,000/year; rising to 1.7/100,000/year in women aged 20 to 24 years, and peaking at 16.5/100,000/year in women aged 45 to 49 years. Only 10% of the cases occurred in women aged 75 or more.[11] Pregnancy confers protection from endometrial carcinoma. Although nulliparity by itself does not appear to increase the risk of endometrial cancer, [12] it is associated with an increased risk of ovarian cancer.[13] The use of combination OCPs decreases the risk of both endometrial and ovarian cancer. [14] There is epidemiological data to suggest that smoking stimulates hepatic metabolism of estrogens, leading to a reduced incidence of endometrial abnormalities, [15] whereas, several studies have suggested that smokers are at an increased risk of developing mucinous ovarian cancer. [16] In a case-control study on risk factors for endometrial cancer in 752 women with histologically confirmed endometrial cancer, in Italy, the cases were less frequently smokers and in premenopause, and the risk of endometrial cancer tended to be lower in parous women. [17] We in our study had 10.8% of uterine corpus tumors with smoking history, which was more than ovarian tumors but less than uterine cervix. Although, our cases like them were less frequently premenopause, most of them were multiparae. The major risk factors for cervical cancer include early onset of sexual activity, multiple sexual partners, a high-risk sexual partner, history of sexually transmitted diseases, smoking, and high parity. [18] Collaborative reanalysis of individual data on 8097 women with SCC and 1374 women with adenocarcinoma of the uterine cervix, from 12 epidemiological studies, indicated that contrary to SCC of the cervix, cigarette smoking is not associated with an increased risk of adenocarcinoma of the cervix compared to nonsmokers. [19] Our data also confirmed these results. Death of young women is also prospected in developing countries. It was reported in the emergency gynecology ward of Kenyatta National Hospital in Nairobi that 46% of the deaths were mainly due to gynecologic malignancy (mainly cervical carcinoma). [20] Despite reports from cancer statistics in 2006, which indicated that the most frequent gynecologic malignancies among 71090 patients with ovarian, uterine corpus, and uterine cervix malignancies were respectively, uterian corpus tumors (58%), ovarian (28.4%), and uterine cervix (13.6%) cancers, [1] distribution of different types of gynecologic malignancies in our study showed a higher incidence rate for ovarian cancer than uterine corpus and uterine cervical malignancies. The lower rate of cervical cancer than ovarian cancer may be due to the widespread screening programs, which have been actively performed during the recent years. In 1999, it was reported that invasive carcinoma of the uterine cervix in Iran was mostly diagnosed at stage II rather than stage I, III or IV. In this study we found results [21] that are similar to reports from developing countries. [22] Mangunkusumo et al ., reported that uterine cervical cancer was the most frequent gynecologic malignancy (60.3%) in Indonesian women, with genital tract neoplasm, followed by ovarian (25.5%) and uterine corpus carcinoma (6.9%). Similar to our study, SCC of cervix, cystadenocarcinoma of the ovary, and adenocarcinoma of the uterus were the most frequent types of malignancies. Distribution of age between different types of gynecologic malignancies in our study was more or less the same as in their reports. [23] Donat et al ., studied different types and frequencies of gynecologic tumors in the Gondar region of Ethiopia for a five-year period, from 1982 to 1986. Uterine cervix carcinoma (34.4%) and breast carcinoma (31.2%) had mostly been reported, followed by endometrial carcinoma (13%) and ovarian carcinoma (11.8%). They have also reported a lower mean age for their patients compared to the data previously reported in the literature. [24] We concluded that race and ethnicity may be the reason for the different incidence of gynecologic cancers. The lower frequency rate of carcinoma of the uterine cervix in our study rather than the mentioned study in Ethiopia, may be due to the increased rate of screening in Iranian women. Bughrara et al ., have studied the incidence of histological types of ovarian tumors in Libya and Poland. Unlike in the Poland series, in Libya, germ cell tumor was the most common type of ovarian neoplasm (50%), while the percentage of epithelial tumors accounted for 33.3%. This proportion of incidence of epithelial and germcell tumors in Libya was in contrast to the relative frequency of these tumor types noted in our study. The difference in incidence of the histological types of ovarian tumors in Libya and our study is probably due to the higher rate of fertility among Libyan women as compared with other populations. [25] The incidence of Epithelial Ovarian Cancer (EOC) varies among races and according to geographical location. Western countries, including the United States, have rates approximately three to seven-fold greater than Japan, although the rate is higher in Japanese immigrants to the United States. Caucasians develop EOC almost 1.5 times more frequently than African-Americans. [26] We concluded that the higher frequency of EOC in our population may be related to various ethnicities. Parazzini et al ., performed a case-control study on women below 75 years in Itlay. The most frequent tumors, as in our study, were serous tumors followed by mucinous tumors. Similar to our study, serous, endometrioid, and other types of ovarian cancers tended to be lower in parous women in comparison with nulliparae. In their study, parity and OCP use were associated with a reduced risk of cancers. [27] In our study we found 27% of the ovarian tumor cases were nulliparae, which indeed was more than in uterine corpus and cervix tumors. Similar to their study, use of OCP was only reported in few cases of our ovarian tumor cases, which meant that most cases of ovarian tumors in our study had not mentioned OCP usage during their life. An analysis of 45 epidemiological studies from 21 countries found that compared to women who had never used OCPs, any use of OCPs was associated with a significant reduction in the risk of developing ovarian cancer, [28] which was confirmed by our data. In an individual incidence data on 7167 ovarian cancer cases diagnosed during the period 1975-1998, from the Osaka Cancer Registry′s database in Japan, the age-adjusted incidence rate of ovarian cancer tended to increase. Poorer prognosis was also suggested in Japanese ovarian cancer patients. [29] While in our study most of ovarian tumor cases were diagnosed as well-differentiated tumors or moderately-differentiated tumors, the incidence seemed to decrease after the obvious peak at 45-55. Although it is mentioned that the overall risk of malignancy for an adnexal mass in premenopausal and postmenopausal women is 6-11% and 29-35%, we found that most of our patients with ovarian carcinoma were premenopausal. [10] In our study, the most frequent age group of patients with endometrial carcinoma was similar to that mentioned in the literature. Also the diagnosis was probably in its early stages. However, like ovarian tumors there were more premenopausal patients than that mentioned in the literature. [30] In summary, in this cross-sectional study we found more ovarian tumors than other gynecologic malignancies. Although distribution of age groups for different tumors was more or less similar to that mentioned in the literature, premenopausal status was indicated more often. Greater awareness of the symptoms of ovarian cancer might lead to earlier diagnosis and treatment and thus possibly improve survival. [31] Annual gynecologic examination with an annual pelvic examination is recommended by the American College of Obstetricians and Gynecologists (ACOG) Committee on Gynecologic Practice for preventive health care. [32] Due to the lack of a convenient and cost-effective anatomical pathology system and computer-based medical records, the interpretation of the data presented in this study is limited. Also, the number of cases was small. To be able to compare cancer incidence in Iran with that in other countries, steps should be and are being taken to establish a population-based cancer registry, besides the pathological- and hospital-based registry which is already in progress. More studies are necessary to assess the nature, age distribution, and stage of different gynecologic cancers, which can help the physicians′ preventive and therapeutic modalities in the community. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09048t2.jpg] [cn09048t1.jpg] [cn09048f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}