 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
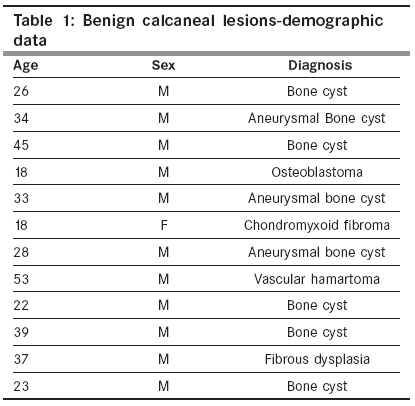
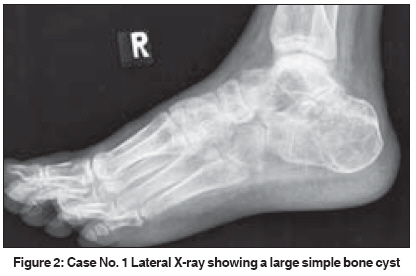
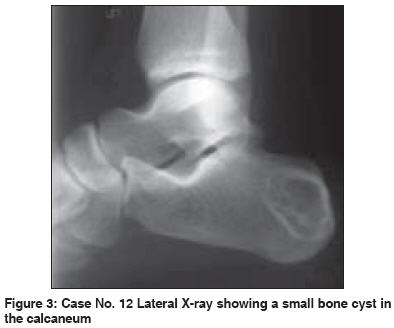
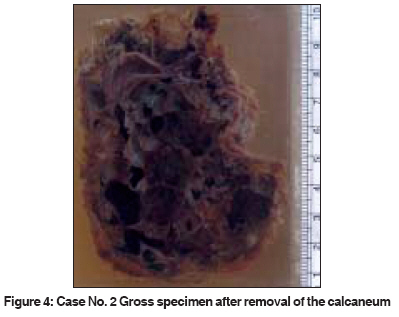
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 234-236 Brief Report Benign tumors and tumor-like lesions of the calcaneum: A study of 12 cases Oommen AT, Madhuri V, Walter NM Department of Orthopedics Unit 2, Christian Medical College, Ida Scudder Road, Vellore - 632004 Code Number: cn09050 PMID: 19574677 Abstract Benign tumors of the calcaneum are rare. Cystic lesions such as simple bone cysts and aneurysmal bone cysts are commonly seen.Aims and Objectives: To evaluate tumors of the calcaneum, which were seen over a 12-year period. Materials and Methods: We analyzed noninfectious, noninflammatory, benign lesions of the calcaneum seen in the Orthopedic Out Patient Department from 1991 to 2003. Twelve such tumors were encountered. There were 11 males and one female and their ages varied from 18 to 53 years with a median of 31. Data was collected from the histopathology reports, radiographs, and inpatient and outpatient records. One of the coauthors reviewed the histopathologic findings of all the tumors. Results: Twelve benign lesions were seen in 12 patients. In our series, cysts predominated, with three aneurysmal bone cysts and five simple bone cysts. The other benign tumors were: one fibrous dysplasia, one vascular hamartoma, one osteoblastoma, and one chondromyxoid fibroma. The bone cysts were treated by curettage, with or without bone grafting, except for one large aneurysmal bone cyst, which was treated by excision of the calcaneum. The postoperative function in this patient was good, with modified footwear. Conclusion: The calcaneum is an uncommon site for most bone tumors, and in our series, bone cysts were the most common benign lesions. Curettage and bone grafting or the use of bone substitutes can be effectively used in the treatment of symptomatic bone cysts of the calcaneum. Keywords: Aneurysmal bone cyst, bone cyst, bone grafting, calcaneum, curettage Introduction Tumors and tumor-like lesions of the calcaneum are rare, [1],[2] the most common being simple bone cysts, aneurysmal bone cysts, and chondroblastomas. [3],[4] Other lesions that have been encountered are lipomas, pseudocysts, and hemophilic cysts. [5] Cystic lesions in the calcaneum differ from those at other sites because they are less prone to pathological fractures and also respond differently to therapy. [5] The clinical relevance of calcaneal bone cysts have been controversial, as most of these lesions have been discovered incidentally. Even very large cystic lesions do not often present with pathological fractures. In a series of 47 patients with 50 calcaneal cysts only four pathological fractures were reported. [5] The frequency and behavior of benign calcaneal tumors has not so far been reported in the Indian population. The purpose of this study is to evaluate these lesions, as seen in our department, over a 12-year period. Materials and Methods We analyzed 12 consecutive benign tumors of the calcaneum, seen over a 12-year period, from 1991 to 2003. Data was collected from histopathology reports, radiographs, as well as, inpatient and outpatient records. Biopsy slides of all tumors were reviewed by one of the coauthors. The follow-up period ranged from 6 months to 3 years. All patients had a lateral radiograph of the ankle (with heel) as well as an AP projection of the ankle.Results Tumors, benign tumors, and cystic lesions of the calcaneum formed 1.9% (12 out of 617) of the bone tumors seen from 1991 to 2003. There were 11 males and one female. The age of these patients ranged from 18 to 53 years with a mean of 31.3 years at presentation [Table - 1]. In our series, cysts predominated, with three aneurysmal bone cysts and five simple bone cysts. One patient had two small distinct cystic lesions, which were diagnosed as fibrous dysplasia on histopathologic examination. The remaining tumors included one case each of vascular hamartoma, osteoblastoma, and chondromyxoid fibroma. The commonest symptoms were heel pain with swelling [Figure - 1] and associated discomfort on walking. The duration of heel pain (present in all patients) varied from 3 months to 5 years. Swelling of the heel (four patients) was present for 3 months to 1 year and broadening of the heel (three patients) for 2 to 5 years. No patient presented with pathological fractures, although three gave a history of persistent low-grade pain after a trivial injury. Preoperative radiographs were available for eight patients with cysts. These showed single cysts in three cases [Figure - 2] and [Figure - 3], two distinct cystic lesions in one case, multilocular cysts in three cases, and one case with expansile multilocular cystic involvement of the whole calcaneum [Figure - 4]. Five patients underwent curettage alone and another five were treated with curettage and bone grafting. One patient underwent curettage and filling of the cyst with bone substitute (Tricalcium Phosphate pellets). Another underwent excision of the calcaneum. The patient who underwent calcanectomy had an expansile aneurysmal bone cyst involving the entire calcaneum. The tendoachilles was attached to the talus to minimize loss of plantar flexion. This patient was subsequently ambulated with modified footwear. The follow-up period varied from 6 months to 3 years. All cysts healed completely, with no limitation of activities. On follow up, the patient diagnosed with osteoblastoma (treated by curettage) showed filling up of the cavity at 1 year 3 months. Six patients who underwent curettage and bone grafting or bone substitutes had no recurrence at follow up. The lone patient with calcaneum excision was able to ambulate without support for more than 1 km on a postoperative follow up at 3 years. Discussion Among four of the largest series of bone cysts published, the calcaneus shows a prevalence of about 2%. [5],[6],[7] Our study confirms the rarity of benign calcaneal tumors as we were able to find only 12 such lesions in a 12-year period (1.9% of the bone tumors seen during this period). Prior reports have found most of these lesions to be cysts, [3],[4],[5],[8] and this too is reflected in our population, with cysts forming more than 50%. Chondroblastoma, [1],[9],[10] a lesion well known to occur in other bones of the foot was notably absent in our series. A possible reason for this could be that the chondroblastoma formed a much smaller component of a large secondary aneurysmal bone cyst and hence was not sampled by the biopsy procedure. [3] Simple bone cysts of the calcaneum differ from bone cysts in other sites because they have a significantly lesser risk of pathological fracture. [5] Cysts reaching a critical size, defined as 100% intracalcaneal cross section in the coronal plane and at least 30% in the sagittal plane, are said to be at risk for becoming symptomatic and developing a fracture. [5] However, we did not encounter a pathological fracture in any of our cases, including the patient who had an aneurysmal bone cyst lesion with 100% involvement. The treatment for symptomatic bone cysts is curettage and bone grafting or use of synthetic bone substitutes. In our experience both bone grafting and bone substitutes have yielded satisfactory healing, with obviously less morbidity for bone substitutes. Steroid injections, which are useful at other sites, do not seem to be of much value in the treatment of calcaneal cysts.[11] An unusual surgical modification of total calcanectomy, used by us in one patient, was implantation of the tendoachilles into the posterior aspect of the talus. This resulted in a satisfactory outcome, clinically. Conclusion The calcaneum is an uncommon site for benign bone lesions. Most such lesions are cysts rather than true tumors. The prevalence of bone cysts in the calcaneum in our series was 1.3% (eight cysts out of 617 tumors). Simple bone cysts of the calcaneum differ from bone cysts in other sites because they have a significantly lesser risk of pathological fracture. Bone cysts can be satisfactorily treated by curettage and bone grafting or use of synthetic bone substitutes.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09050f1.jpg] [cn09050f3.jpg] [cn09050f4.jpg] [cn09050t1.jpg] [cn09050f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}