 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
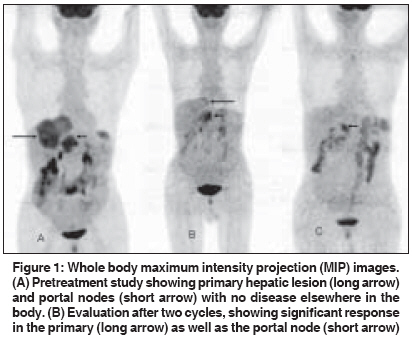
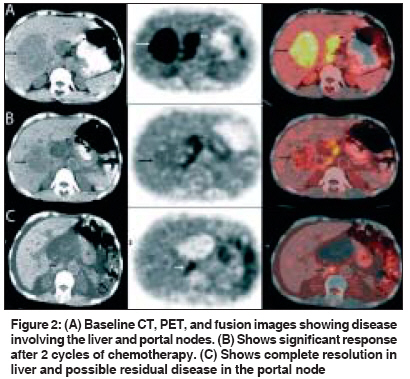
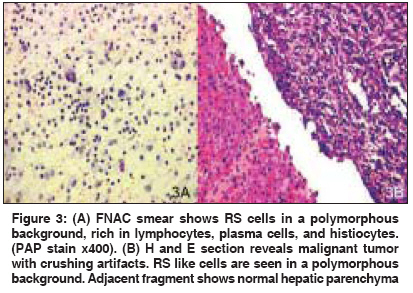
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 237-239 Case Report Positron emission tomography / computerized tomography evaluation of primary Hodgkin's disease of liver Gota VS, Purandare NC, Gujral S, Shah S, Nair R, Rangarajan V Department of Bioimaging, Tata Memorial Hospital, Dr. Ernest Borges Road, Parel, Mumbai - 400 012 Code Number: cn09051 PMID: 19574678 Abstract Occurrence of primary Hodgkin's lymphoma (PHL) of the liver is extremely rare. We report on a case of a 60-year-old male who presented with liver mass and B-symptomatology. Hepatoma or hepatic metastasis from a gastrointestinal primary was initially suspected. Tumor markers like AFP, CEA, Total PSA, and CA-19.9 were within normal limits. Positron Emission Tomography / Computerized Tomography (PET/CT) revealed a large hepatic lesion and a nodal mass in the porta hepatis. A liver biopsy was consistent with Hodgkin's lymphoma. There was complete regression of the hepatic lesion and evidence of shrinkage of the nodal mass following four cycles of chemotherapy. 18F Fluro -de-oxy Glucose (FDG) PET / CT in this case helped in establishing a primary hepatic lymphoma by demonstrating the absence of pathologically hypermetabolic foci in any other nodes or organs. PET / CT scan is a useful adjunct to conventional imaging and histopathology, not only to establish the initial diagnosis, but also to monitor treatment response in PHL. Keywords: Hodgkin′s lymphoma, primary hepatic lymphoma, positron emission tomography / computerized tomography Introduction Primary hepatic lymphoma (PHL) defines an extranodal lymphoma of the liver with or without regional lymph node involvement, without involvement of any other organ. [1] A computed tomography (CT) scan is the commonly used modality for staging lymphomas. The accuracy of anatomic imaging, like the CT scan, in the identification of a disease in normal-sized lymph nodes or in the detection of nonmalignant disease within enlarged nodes is limited. [2] The widespread use of Positron Emission Tomography / Computerized Tomography (PET/CT) takes advantage of the anatomic resolution of the CT scan and the biological characterization provided by 18 F Fluoro -de-oxy Glucose (FDG)-PET. Together, it results in the improvement in the accuracy of detecting the extent of disease, response evaluation, and prognostication. [3] Detection of a more extensive disease by PET / CT, rather than by conventional imaging, would be of major relevance for patients with apparently limited stage hepatic lymphoma (HL0, in whom upstaging could alter the management. PET / CT is also useful in the early assessment of treatment response. We report the PET / CT findings of an extremely rare case of primary Hodgkin′s disease of the liver.Case Report A 60-year-old male presented with a six month′s history of abdominal pain, back ache and a 10-kg weight loss. On examination, te liver was palpable 5 cm below the right costal margin. There was no splenomegaly. Notable laboratory findings included hemoglobin of 10.1 g/dl and serum LDH of 150 U/L. Normal results included those for blood counts, renal and liver function, and chest x-ray. Serology for human immunodeficiency virus (HIV), hepatitis B, and hepatitis C was negative. Computerized Tomography scan of the abdomen and pelvis showed a heterogeneously enhancing soft tissue mass in the right hepatic lobe measuring 9 x 7 cm. In addition a nodal mass was seen at the porta hepatis. The patient referred for a whole body PET / CT study to look for other sites of involvement. The patient was injected with 10 millicuries of 18 F Fluoro de oxy Glucose (FDG) and after 60 minutes of uptake time, underwent a whole body scan in a dedicated PET / CT scanner. A whole body FDG PET / CT study revealed avid FDG uptake in the hepatic lesion and in the portal nodes [Figure 1A], with the rest of the whole body study appearing unremarkable. The liver lesion showed maximum standardized uptake value (SUV) of 21.9 [Figure 2A]. The nodal mass at the porta showed a maximum SUV of 22.5. Tumor markers AFP, CEA were within normal limits. Fine needle aspiration cytology (FNAC) of the liver lesion showed several singly scattered large tumor cells with multilobulated nuclei [Figure 3A]. The background was formed by strands of spindle cells admixed with lymphoplasmacytic cells. The differential diagnosis considered included malignant lymphoma, anaplastic carcinoma, and pleomorphic sarcoma. Ultrasound-guided liver biopsy was performed, which revealed cellular fragments of fibrocollagenous tissue with crushing artifacts. It showed clusters of large atypical cells with occasional binucleate forms amidst mature lymphocytes, plasma cells, and fibroblasts [Figure 3B]. The large atypical cells had prominent eosinophilic nucleoli and were immunonegative to LCA, CD20, CD15, and CD43. A stain for CD30 was weakly positive in these tumor cells. Liver biopsy was consistent with the diagnosis of extranodal classical Hodgkin′s lymphoma. The peripheral blood smear was normal. Bone marrow aspiration and trephine biopsy were performed and revealed normal hematopoesis with no tumor infiltrates. There was no other site of involvement based on physical examination in the FDG PET/CT study. These findings established the diagnosis of primary hepatic Hodgkin′s lymphoma. He was treated with a chemotherapy regimen consisting of Adriamycin, bleomycin, vincristine, and dexamethasone (ABVD). An early response evaluation was done by PET / CT following two cycles of ABVD. The hepatic lesion had regressed and there was evidence of shrinkage of the nodal mass [Figure 1B] and [Figure 2B]. There was a 30% reduction in the size of measurable lesions on the CT images, with significant reduction in the metabolic activity in the liver lesion and the portal nodes (SUV - liver lesions 2.8 and portal nodes 3.7). PET / CT was again repeated following four cycles of ABVD, which showed complete regression of the hepatic lesion on CT, with no significant uptake of FDG in the liver lesion. Low grade FDG uptake of SUV 3 was seen in the portal nodes [Figure 1C] and [Figure 2C].Discussion Primary Hodgkin′s Lymphoma is notably rare, representing < 1% of all extranodal lymphomas. [1] Non-Hodgkin′s lymphoma (NHL) is the major histological subtype of PHL. PHL with Hodgkin′s histology is extremely rare. To the best of our knowledge, only three cases of primary hepatic Hodgkin′s lymphoma have been reported in the literature so far. [4],[5],[6] A definite diagnosis of PHL is difficult to establish on clinical grounds. Hepatoma and metastasis from gastrointestinal (mostly colon) carcinoma present in a similar manner and are much more common. Normal levels of tumor markers AFP and CEA are found in almost all cases of PHL. [1] Diagnosis of PHL requires a liver biopsy compatible with lymphoma and the absence of a lymphoproliferative disease outside the liver. [7] Our case fits these traits: normal levels of tumor markers, liver biopsy consistent with Hodgkin′s histology, and the disease confined to the liver and regional draining nodes only. FDG PET / CT in this case helped in establishing the possibility of PHL, by demonstrating the absence of pathologically hypermetabolic foci in any other nodes or organs. PET / CT identified significant treatment response after two cycles and this was similar to the reported role of PET in lymphomas, in assessing early treatment response. [8],[9] Post a four-cycle evaluation, it raised the possibility of small residual disease in the node. An end treatment scan after six cycles possibly would have clarified if this uptake represented reparative change or residual disease. This was not possible in our patient as he had a sudden death at home prior to the fifth cycle of ABVD. In conclusion, the occurrence of primary Hodgkin′s disease of the liver is extremely rare. Confirmation of the diagnosis requires liver biopsy and exclusion of tumor at other sites. A PET / CT scan is one of most useful noninvasive imaging modalities for the diagnosis and evaluation of treatment response for this condition. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09051f2.jpg] [cn09051f1.jpg] [cn09051f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}