 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
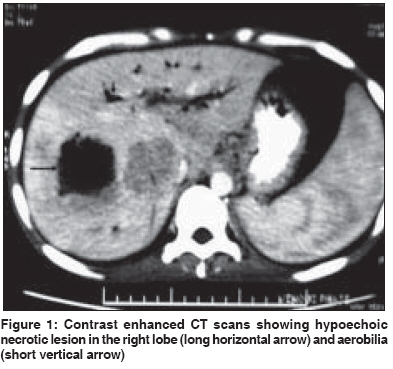
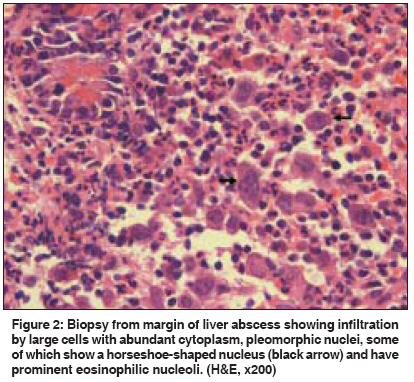
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 240-241 Letter To Editor Anaplastic large cell lymphoma presenting as liver abscess and portal vein thrombosis Chalamalasetty SB, Madan K, Javvaji S, Singh KK, Vijayaraghavan M, Mathur S, Kumar L, Paul S, Acharya SK Department of Gastroenterology and Human Nutrition Unit, All India Institute of Medical Sciences, New Delhi - 110 029 Code Number: cn09052 PMID: 19574679 Sir The presentations of space occupying lesions of the liver may range from being asymptomatic to catastrophic presentations such as the rupture of hepatocellular carcinoma. We report a young man with primary hepatic lymphoma (PHL), who presented with liver abscess and portal vein thrombosis and had a rare variant of non-Hodgkin′s lymphoma (NHL), called the anaplastic large cell lymphoma (ALCL). PHL presenting as a liver abscess, with extra hepatic portal venous thrombosis (PVT) has not been reported earlier. A 28-year-old gentleman presented with a history of fever for one year followed by jaundice and pruritus, and subsequently developed melena without hematemesis. This was followed by pain in the right upper quadrant and abdominal distension along with loss of appetite and weight. On examination, he was emaciated; was febrile, pale, and had bilateral pitting pedal edema. There was no icterus or lymphadenopathy. He had hepatomegaly, palpable globular gallbladder, mild splenomegaly, and ascites. Investigations revealed: Hemoglobin 4.6 g/dL, TLC 12,900/mm 3 with 88% polymorphs, ESR 75 mm/first hour, serum bilirubin 0.7 mg/dL, aspartate aminotransferase 24 IU/L, alanine aminotransferase 19 IU/L, alkaline phosphatase 1466 IU/L, and albumin 2.1 g/dL. AFP, CEA, and CA 19-9 were normal. Ascitic fluid was negative for malignant cells. Enzyme linked immunosorbent assays for hepatitis B surface antigen, antibodies to hepatitis C virus, and human immunodeficiency virus 1 and 2 were negative. Dual phase computed tomography (CT) showed multiple irregular necrotic lesions in both lobes, with the largest one in segment VII, with a peripherally enhancing soft tissue mass, which was seen extending till the porta and infiltrating the second part of the duodenum. There was air within the mass and in the biliary radicles, suggesting bilioenteric communication. The main portal vein and its intrahepatic branches were replaced by collaterals. There was minimal ascites and no evidence of retroperitoneal lymphadenopathy [Figure - 1]. Grade III esophageal varices were seen on endoscopy. A bone marrow examination did not show any abnormal cells. At admission, a provisional diagnosis of multiple liver abscesses with secondary PVT was made and he was started on antibiotics, with catheter drainage of the right lobe lesion. The pus grew Escherichia coli on culture and was negative for malignant cells. The drain fluid became bilious for which an endoscopic retrograde cholangiopancreatography (ERCP) for biliary drainage was planned. However, a side-viewing endoscopy revealed nodular infiltration in the second part of the duodenum. A biopsy from the infiltrated duodenum and from the margin of the liver abscess [Figure - 2] showed cells with abundant cytoplasm and pleomorphic nuclei. Immunohistochemical stains confirmed the diagnosis of ALCL [Leucocyte common antigen: positive; CD-3: positive; CD-30: positive; Epithelial membrane antigen: positive; CD-20: negative; cytokeratin: negative; CD-15: negative]. The patient received chemotherapy with Berlin-Frankfurt-Munster-90 (BFM- 90) protocol, with which he improved, and a repeat CT after four months showed significant resolution of the hepatic lesions. Primary hepatic lymphoma is an extra-nodal NHL localized to the liver without any extrahepatic disease for at least six months after therapy. [1] PHL comprises 0.4% of all extra nodal non-Hodgkin′s lymphomas, and between 1981 and February 2003, only 251 cases of PHL were reported in the literature. [2] Our patient was initially diagnosed to have liver abscesses. Although amoebic liver abscess is the predominant cause of liver abscess in India, hepatocellular carcinoma with necrosis and metastatic colonic cancer with central necrosis need consideration in the differential diagnosis. Only one case of PHL mimicking liver abscess [3] has been reported earlier. Lymphomas may cause portal venous obstruction either by direct infiltration, extrinsic compression at the porta by lymph nodes, tumor thrombus of the portal vein or by a hypercoagulable state. Direct portal infiltration was probably the cause in the present case. PHL causing portal venous obstruction has not been reported, although tumor thrombus in the portal vein has been described in patients with secondary lymphoma. [4] The type of PHL reported most commonly is diffuse large cell lymphoma (DLCL) of the B-cell phenotype. Our patient had a very rare variant known as ALCL of the T-cell phenotype. In a series of 31 patients with PHL, only one patient had ALCL. ALCL strongly expresses CD-30 (Ki-1) antigen; most are positive for the anaplastic lymphoma kinase (ALK) protein and have a characteristic translocation t(2;5). In the present case CD-30 was positive, but ALK staining was not available. Increased prevalence of hepatitis C virus (HCV) seropositivity has been reported in patients with PHL ranging from 21 - 60%, [5] but our case was negative for anti-HCV. In conclusion, this report represents a rare case of primary hepatic anaplastic large-cell lymphoma. Atypical liver masses or abscesses should raise the suspicion of lymphoma as one of the differential diagnoses. Acknowledgments This case was presented as a clinicopathological case at the All India Institute of Medcial Sciences. Brigadier Dr. A C Anand (Advisor, Army Hospital, Research and Referrals, New Delhi) who was the clinical presenter was able to make the correct diagnosis of lymphoma of the liver involving the duodenum and causing portal vein thrombosis.References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09052f2.jpg] [cn09052f1.jpg] |
| |||||||||

{kind=link}
{kind=link}