 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
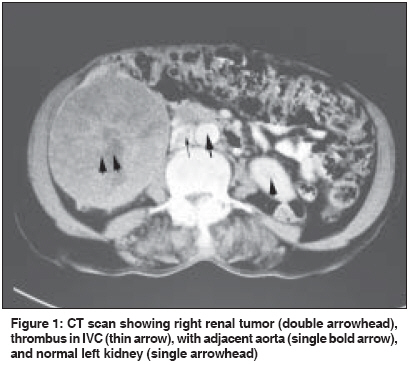
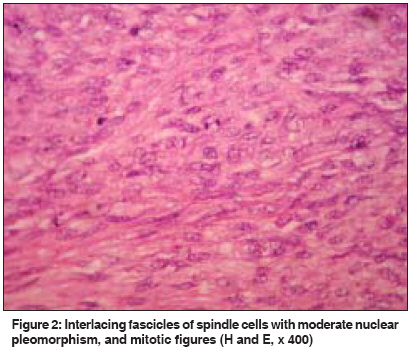
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 241-243 Letter To Editor A case of leiomyosarcoma of kidney clinically and radiologically misdiagnosed as renal cell carcinoma Choudhury M, Singh SK, Pujani M, Pathania OP Department of Pathology, Lady Hardinge Medical College and Smt. Sucheta Kriplani Hospital, New Delhi Code Number: cn09053 PMID: 19574680 Sir Renal sarcomas are rare, but highly aggressive neoplasms, accounting for 1 to 2% of all malignant renal tumors. [1] Since the prognosis for a renal sarcoma is particularly poor, differentiation from sarcomatoid renal cell carcinoma is necessary, but often difficult, based only on clinical presentation, radiographic findings, and, in some cases, pathological analysis. Leiomyosarcoma is the most common histological subtype constituting 50-60% of renal sarcomas. [1],[2] A 65-year-old female presented with an abdominal lump associated with pain, constipation, weight loss, and anorexia, of one-year duration. An ultrasound (US) of the abdomen revealed a large heterogeneous mass in the right lumbar region of the renal fossa measuring 14 x 10 cms. Doppler US showed a large thrombus in the inferior vena cava (IVC) up to the lower level of the hepatic veins. A computed tomography (CT) scan of the abdomen revealed a large exophytic, heterogeneous mass, with foci of necrosis, at the apex and midpolar region of the right kidney [Figure - 1]. A CT scan of the chest was unremarkable. A clinical diagnosis of renal cell carcinoma was made and the patient underwent radical nephrectomy. Thrombolytic therapy (streptokinase) was delivered through a catheter and patient was given heparin for ten days postoperatively. Grossly the tumor was large, globular, and encapsulated, measuring 15 x 11 x 8 cms at the upper pole of the right kidney. The cut surface was a homogenous gray white, firm, with areas of whorling and trabeculations, along with foci of necrosis. The attached kidney measured 6 x 4 x 3 cm. The adrenal gland was unremarkable. The examined microsections showed a tumor composed of spindle cells arranged in interlacing fascicles with moderate nuclear pleomorphism, multinucleation, and focal areas of necrosis. Mitotic figures were 4-5 / 10 hpf [Figure - 2]. Van Gieson`s and Masson`s trichrome stains helped to confirm the smooth muscle origin. On immunohistochemistry, the tumor was vimentin and smooth muscle actin (SMA) positive, and cytokeratin (CK) and desmin negative. Therefore, a final diagnosis of renal leiomyosarcoma was established. Sections from the renal pelvis, ureter, and attached adrenal were unremarkable. Seven aortocaval lymph nodes showed reactive hyperplasia. Postoperative Doppler US revealed a thickened and narrowed inferior vena cava with a normal left renal vein. The patient was closely followed for one year, but thereafter was lost to follow-up. Primary renal sarcomas constitute 0.8 to 2.7% of all renal tumors in adults. [3] Leiomyosarcomas constitute 0.12% of all invasive renal malignancies, as studied by Kendal. [4] Renal leiomyosarcoma has a preponderance in women, with gradually increasing incidence with advancing age. The patients present with a classical triad of flank pain, hematuria, and abdominal mass mimicking renal cell carcinoma. It is difficult to differentiate between leiomyosarcoma and renal cell carcinoma radiologically, and the diagnosis is usually made postoperatively. Histogenesis remains obscure, because renal sarcomas may arise from the smooth muscle fibers of the renal parenchyma, capsule, renal pelvis or vessels. Renal leiomyosarcoma, like many sarcomas, tends to displace rather than invade the parenchyma, and it is characterized by a rapid growth rate, frequent metastasis, and high local and systemic recurrence rates. Radical surgery offers the best chance of cure, and the role of adjuvant chemotherapy and / or radiotherapy remains debatable, due to the paucity of data on the treatment of this rare renal neoplasm. In a study by Kendal WS, leiomyosarcoma exhibited a median overall survival of 25 months, with a 25% five-year overall survival and a 60% five-year cause-specific survival. [4] Different etiologic factors, such as, local problems, malignancies, and lupus anticoagulants seem to contribute to the risk of IVC thrombosis. Retroperitoneal leiomyosarcoma, adrenal cortical carcinoma, and renal angiomyolipoma have all been reported as presenting in association with IVC thrombus, either due to direct compression or vascular invasion. Medical management includes the anticoagulation therapy - heparin, warfarin, and thrombolytic agents, while surgical therapy encompasses caval interruption and thrombectomy. [5] References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09053f1.jpg] [cn09053f2.jpg] |
| |||||||||

{kind=link}
{kind=link}