 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
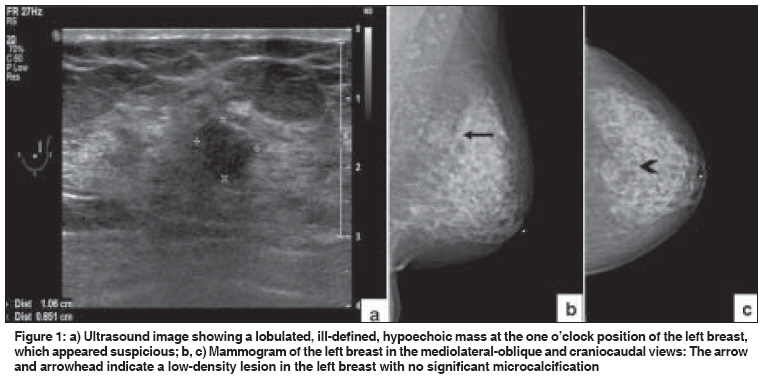
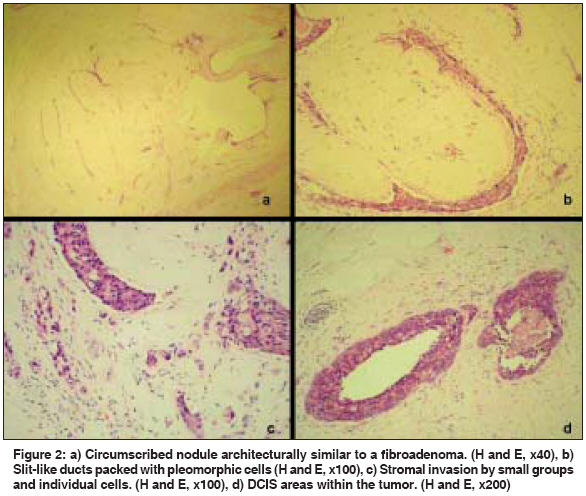
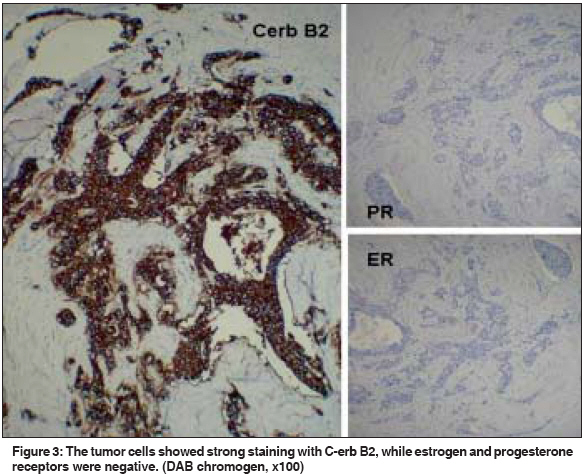
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 244-246 Letter To Editor Infiltrating duct carcinoma within a fibroadenoma Iyengar KR, Peh SC, Yip CH, Vijayananthan A Department of Pathology, Faculty of Medicine, University of Malaya, Kuala Lumpur Code Number: cn09055 PMID: 19574682 Sir Fibroadenoma may rarely be associated with breast cancer, lobular or ductal carcinoma in situ . [1] Infiltrating duct carcinoma (IDC) arising within a fibroadenoma is exceptional. [2] We report a case of fibroadenoma with coexisting IDC and extensive duct carcinoma in situ (DCIS) in a woman with surgical menopause. A 43-year-old woman underwent hysterectomy and bilateral salpingo-oophorectomy in March 2005, for multiple leiomyomata and ovarian follicular cysts. Subsequently she received conjugated equine estrogen (CEE) tablets, 0.625 mg daily, as hormone replacement. A prior breast ultrasonogram showed multiple asymptomatic, nonpalpable fibroadenomas bilaterally, 8.4 mm to 9.5 mm in diameter. No microcalcification was detected on mammography. A follow-up in 2006 was normal, but an ultrasonogram and mammogram in March 2007, showed a suspicious lump [Figure 1a],[Figure 1b],[Figure 1c]. A core needle biopsy was inadequate. No fine needle aspiration cytology (FNAC) was performed. Hook-wire localization and excision of the lump showed a 1.8 cm, firm, whitish nodule. The surrounding breast tissue was unremarkable and surgical margins were uninvolved. Microscopically, the nodule was circumscribed, with slit-like clefts [Figure 2a], resembling a fibroadenoma. However, the cells within the slit-like spaces exhibited marked nuclear pleomorphism and prominent nucleoli [Figure 2b]. There were foci of stromal infiltration by tumor cells [Figure 2c] and typical duct carcinoma in situ [Figure 2d], confined only to the nodule. More than 16 mitoses / 10 high-power fields were noted. Oestrogen or progesterone receptors were negative, but C-erb B2 was overexpressed [Figure - 3]. A diagnosis of IDC with DCIS, probably arising from a fibroadenoma, was made. A carcinoma is deemed to arise within a fibroadenoma when the malignant cells are limited to the fibroadenoma or only focally extend into the adjacent stroma or ducts. [2] Over two hundred cases of carcinoma arising within a fibroadenoma have been reported and the largest series of 105 cases by Diaz et al ., have shown only seven with IDC.[3] Complex fibroadenoma and proliferative disease adjacent to the fibroadenoma are associated with a slight increase in the risk of breast cancer. [4] However, epithelial atypia within the fibroadenoma itself has not been seen to increase the risk of subsequent breast cancer. [5] The Million Women Study has shown that the use of various forms of hormone replacement therapy increased the risk of breast cancer in postmenopausal women, even if they had used it for less than five years. [6] On the other hand, Stefanick et al . has reported that conjugated equine estrogen (CEE) therapy for over seven years following hysterectomy does not increase the risk of breast cancer in postmenopausal women. [7] Thus evidence is conflicting regarding the effect of oestrogen therapy on breast cancer risk. Whether the CEE therapy received by our patient for two years after hysterectomy had a causative role in carcinogenesis in our patient is debatable, since the initial ultrasonogram had shown fibroadenomas, but no histological or cytological examination had been performed. Interestingly in the present case, hormone receptors were undetectable by immunohistochemical studies [Figure - 3]. It was probable that a more sensitive method would have shown a positive reaction. This case highlights the rare association of two common diseases of the breast and the value of regular follow-up for the early diagnosis of malignancy. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09055f1.jpg] [cn09055f3.jpg] [cn09055f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}