 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
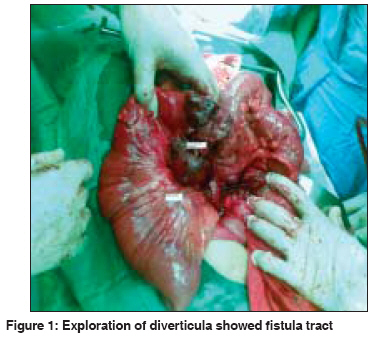
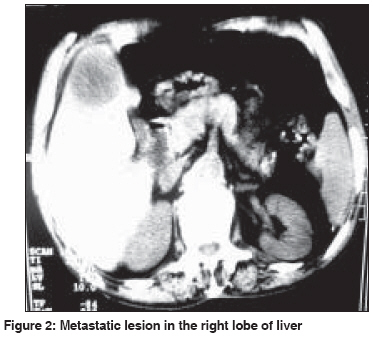
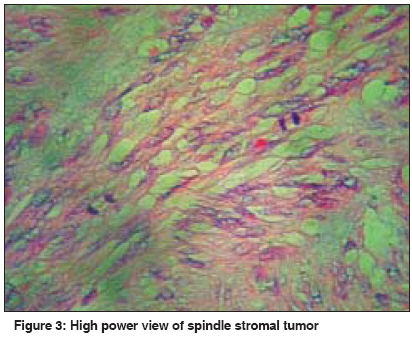
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 246-247 Letter To Editor Enterocolic fistula associated with a gastrointestinal stromal tumor Shamsaeefar A, Hosseini SMohammad Vahid, Motazedian N, Razmi T Department of Surgery, Hormozgan University of Medical Sciences, Bandarabbas Code Number: cn09056 PMID: 19574683 Sir Gastrointestinal stromal tumors (GIST) are the most common primary mesenchymal tumors of the gastrointestinal (GI) tract. [1] GIST usually displace the adjacent organ and have rarely been reported with intraperitoneal rupture or organ invasion. [2],[3] The following case describes a 70-year-old male patient with anemia and chronic diarrhea, who underwent colonoscopic examination. The findings on colonoscopy revealed a large, enterocolic fistula at the spelnic flexure of the colon. Physical examination and Laboratory studies were unremarkable except for the presence of a vague lump in the left upper quadrant and hemoglobin of 7.8 g/dL, respectively. Ultrasonography and computed tomography (CT) showed a mass (8 x 8 cm) at the splenic flexure and a metastatic lesion in the liver. [Figure - 1] and [Figure - 2] Exploration revealed a large diverticulum, which contained a mass that originated from the proximal jejunum and adhered to the medial border of spelenic flexure, associated with entrocolic fistula. Large intraperitoneal and liver metastases were also found. The bowel walls along with the fistula tract were resected and repaired, but the patient was not physiologically suitable for resection of the metastatic lesions. The patient did well in the postoperative period on Imatinib (400 mg/day) during the six-month follow-up. Pathology showed a spindle stromal tumor with low mitosis that was positive for CD117 (Gist tumor). [Figure - 3] Enterocolic fistulas are usually caused by inflammatory conditions such as inflammatory bowel disease. This abnormal communication can also be caused by prior surgery, foreign bodies, pancreatitis, diverticulitis, and, most ominously, by malignancy. [4] The most common sites of tumors are the stomach and small intestine. Most patients with GIST (70%) have symptoms, however, 10% of them are only detected at autopsy. The most common symptom of GIST is anemia due to bleeding from mucosal ulceration. [1],[5],[6] According to our knowledge this presentation of the GIST tumor has been the first report, not only considering the site of occurrence, but also the aggressiveness of the tumor that caused the entrocolic fistula. However, fistula formation can also be explained by tumor pressure and intraperitoneal rupture of the diverticula in advanced GIST, although, in this case the patient had never developed any signs of tumor rupture in his past medical history. Surgery is the definitive therapy for patients with GIST tumor, as radiotherapy and chemotherapy have not been found to be effective in its treatment . Imatinib a selective and competitive inhibitor of tyrosine kinase, has been found to a of metastatic and locally advanced GISTs. We did not resect the metastatic lesions and the patient received only Imatinib, with good response in follow-up. [6] References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09056f1.jpg] [cn09056f2.jpg] [cn09056f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}