 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
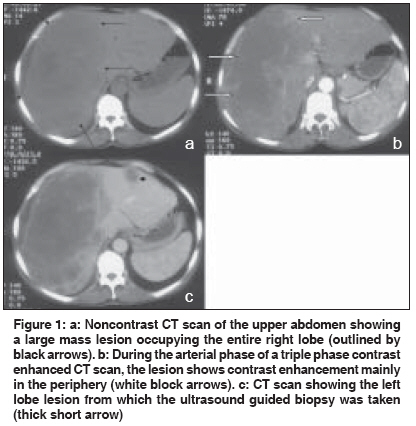
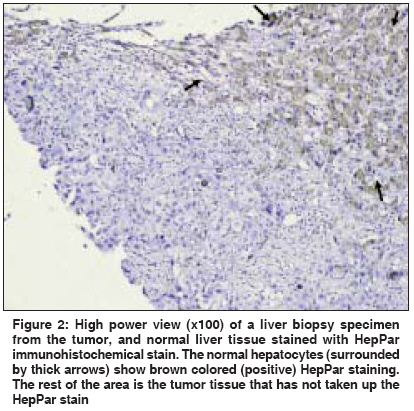
Indian Journal of Cancer, Vol. 46, No. 3, July-September, 2009, pp. 253-254 Letter To Editor Alpha-fetoprotein production by non-hepatocellular carcinoma, malignant liver tumor Saini V, Madan K, Mittal VV, Sakhuja P, Sarin SK Department of Gastroenterology, G B Pant Hospital, New Delhi; Department of Hepatology, Institute of Liver and Biliary Sciences, New Delhi Code Number: cn09061 PMID: 19574688 Sir A 60-year-old, gentleman presented with a three-month-history of a lump in the right upper abdomen. On examination, there was no pallor, jaundice, lymphadenopathy or lower limb edema, and an abdominal examination revealed large, irregular, hard hepatomegaly. Investigations revealed: hemoglobin, 11.3gm%; total leukocyte count, 9200 mm -3 ; platelet count, 330000 mm -3 ; total bilirubin, 1.3 mg%; aspartate aminotransferase, 69 IU/L; alanine aminotransferase, 27 IU/L; alkaline phosphatase 60 IU/L; and an INR of 1.15. HBsAg, total anti-HBc and anti-HCV were negative. A triple phase contrast enhanced CT (TPCT) scan of the abdomen revealed a large, irregular, hypodense lesion in the right liver lobe showing peripheral enhancement in the arterial phase and it was seen compressing the right portal vein. In addition, two hypodense lesions of about 2 x 2 cm showing mild peripheral arterial enhancement were seen in the left lobe of the liver without any abdominal lymphadenopathy [Figure - 1]. Esophagogastroduodenoscopy revealed grade 2 esophageal varices and serum alpha-fetoprotein (AFP) levels were 372 ng/ml. A provisional, working diagnosis of hepatocellular carcinoma (HCC) was considered. For confirmation, a trucut biopsy from the left lobe lesion was performed, which revealed an undifferentiated malignant tumor. Immunohistochemistry of the tumor cells was negative for HepPar, p-CEA (polyclonal carcino-embryonic antigen), and CK-7 (cytokeratin-7) [Figure - 2]. A primary site could not be localized even after colonoscopy, CT scan of the chest, abdomen, and pelvis. Carcinoembryonic antigen levels (2.05 IU/L) and CA 19-9 levels (37.04 IU/L) were normal. The patient refused further workup, and a final diagnosis of AFP producing metastatic adenocarcinoma to the liver, with occult primary, was made. AFP is usually regarded as a specific tumor marker for HCC and germ cell tumors. However, there are case reports in the literature demonstrating that AFP can also be produced by other malignancies, such as gastric adenocarcinoma, pancreatic carcinoma, colonic adenocarcinoma, and prostatic, bladder, and ovarian malignancies. [1],[2] Although AFP levels above 400 ng/ml are considered to be specific for HCC, it is not unusual for HCC to have normal AFP levels, [3] and solely relying on AFP as a predictor of HCC is not recommended. In the present case, the AFP levels were 372 ng/ml and the patient had portal hypertension, which suggested a probable diagnosis of HCC. However, the immunohistological profile was suggestive of a non-HCC and non-cholangiocarcinoma tumor, pointing to a diagnosis of adenocarcinoma. HepPar (or Hepatocyte Antigen) is a monoclonal antibody with high sensitivity and specificity (> 80%) for HCC. [4],[5] It never stains adenocarcinoma cells as in the present case [Figure - 2]. p-CEA is a polyclonal antibody with which a characteristic pericanalicular pattern of staining is seen in HCC specimens, whereas, metastatic adenocarcinomas typically show a diffuse cytoplasmic pattern of staining in > 90% of the cases, [6] however, it was negative in our patient. Negative CK-7 immunostaining argued against a diagnosis of intrahepatic cholangiocarcinoma. Almost all cholangiocarcinomas are CK-7 positive, whereas, HCC and metastatic adenocarcinomas are invariably CK-7 negative. [4] In our case we were not able to detect any primary tumor. Metastatic liver disease with occult primary has been reported earlier, but our case, probably represents a first case of AFP producing metastatic adenocarcinoma in the liver, with occult primary. There is no denying the fact that further investigations might have picked up the primary lesion, but the patient at this stage refused any further investigation or therapy. It is also possible that the tumor may represent a small undifferentiated focus within a larger cholangiocarcinoma or HCC. The tumor may also be having both components of HCC and cholangiocarcinoma within the same lesion and a single small trucut biopsy would have missed such lesions. [6] However, as mentioned earlier, negative CK-7 staining made the diagnosis of cholangiocarcinoma less likely. However, short of a resected specimen, this was the best tissue that could be obtained after an informed consent. In conclusion, this report further strengthens the already accumulating evidence against the specificity of AFP in making a diagnosis of HCC and suggests that AFP may only be a marker of an embryonal de-differentiation of malignant cells, rather than their site of origin. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09061f1.jpg] [cn09061f2.jpg] |
| |||||||||

{kind=link}
{kind=link}