 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
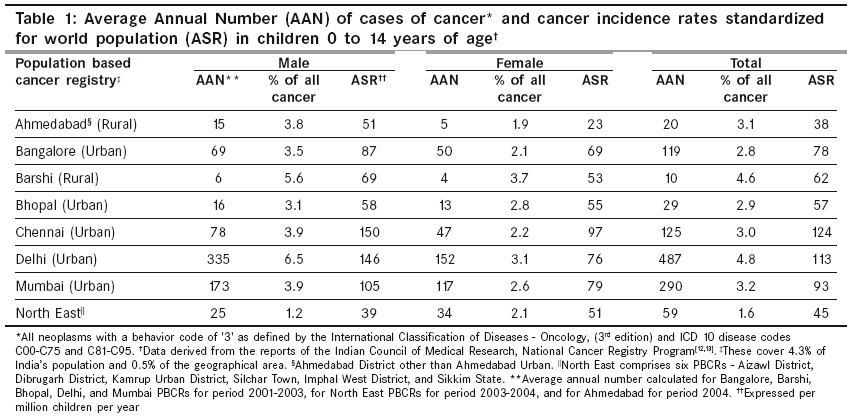
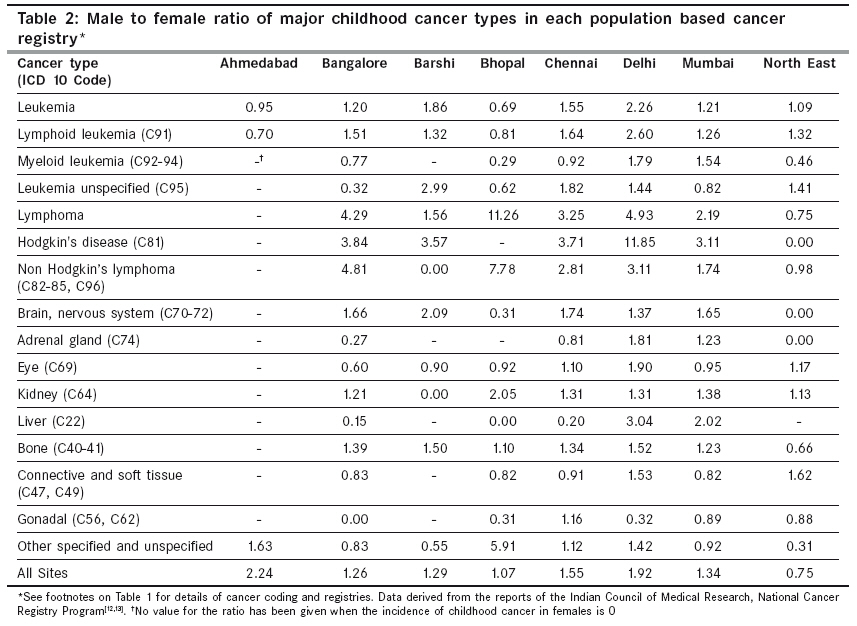
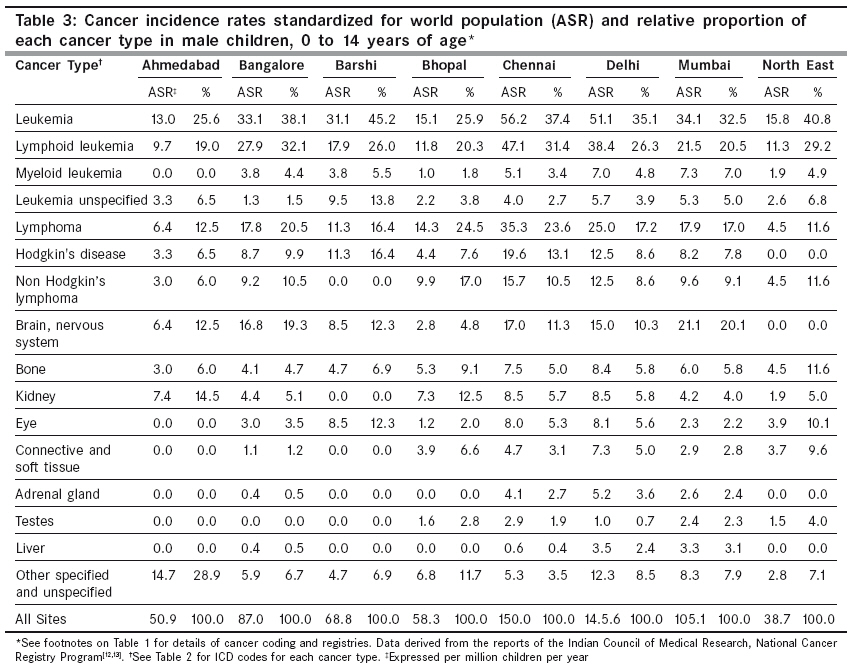
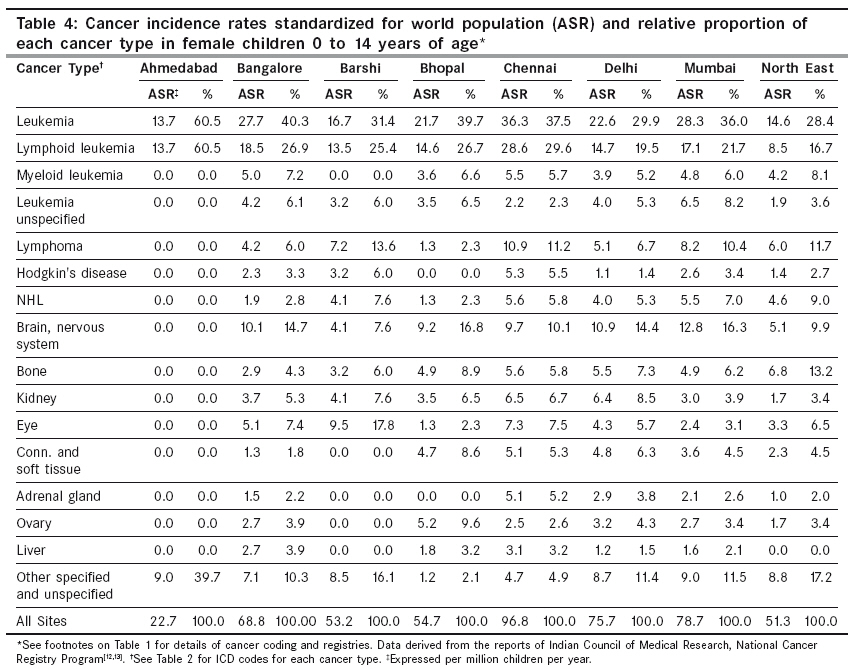
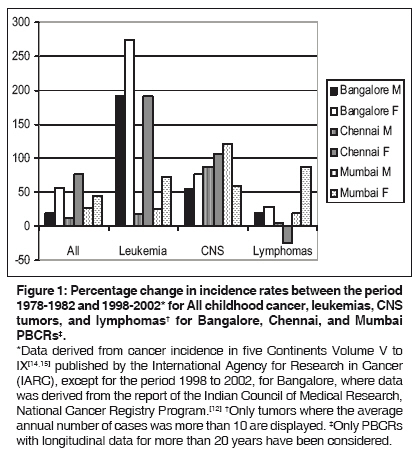
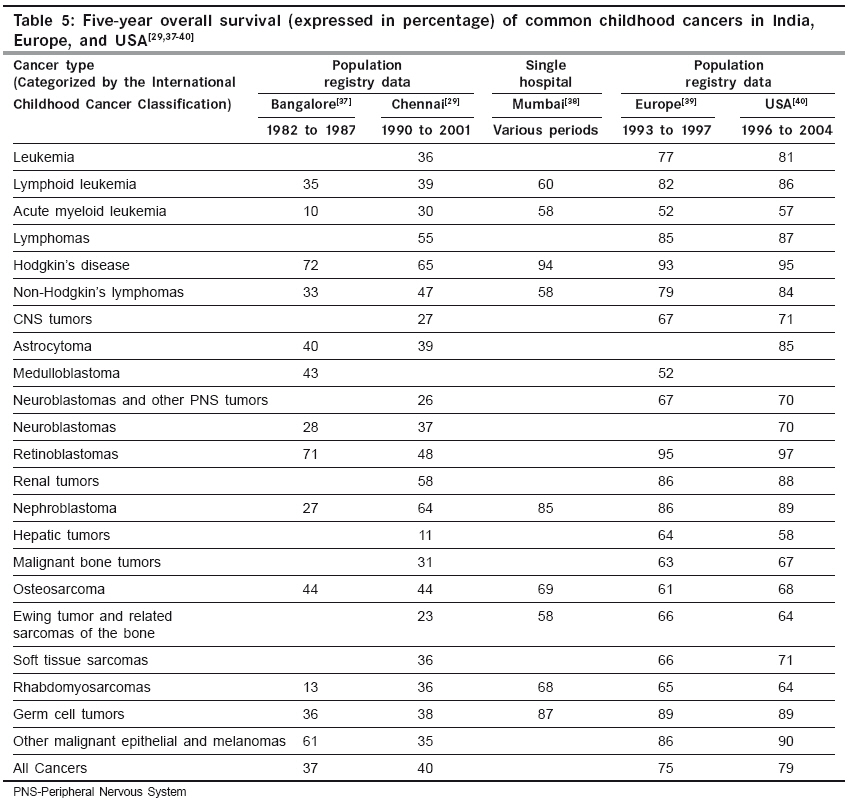
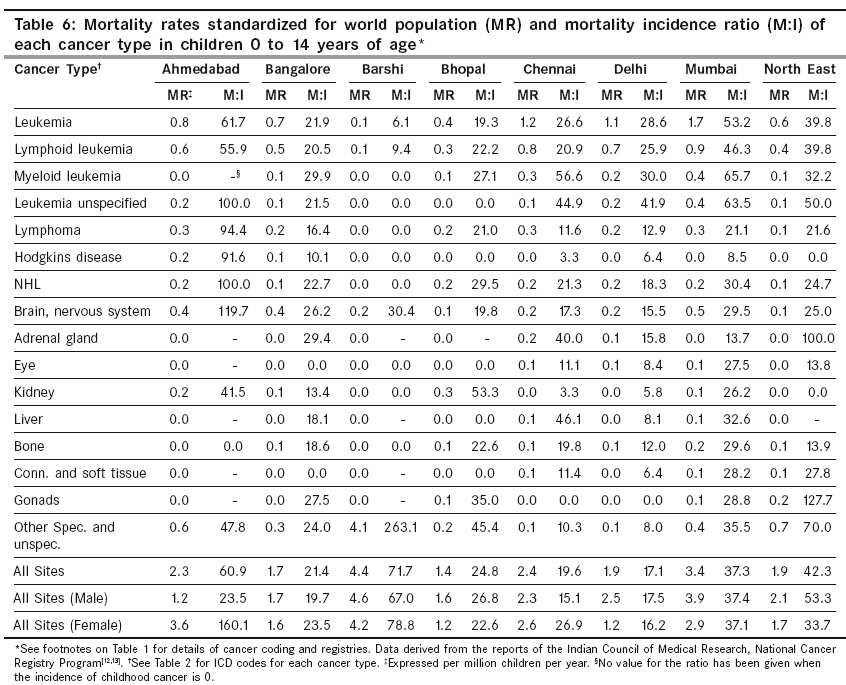
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 264-273 Review Article Epidemiology of childhood cancer in India Arora RS, Eden TOB, Kapoor G Clinical research Fellow, Cancer Research UK Paediatric and Familial Cancer Research Group, University of Manchester, Manchester Code Number: cn09068 PMID: 19749456 Abstract There has been enormous progress in the treatment of childhood cancer in the developed world and the epidemiology in these countries is well described. Hitherto, there has been no attempt to systematically study the burden of childhood cancer in India or to understand how the occurrence and outcome of the disease varies across the country. We have reviewed the epidemiology (incidence, survival, and mortality) of childhood cancer across different population-based cancer registries in India and also compared it with data from the resource-rich countries. Incidence and mortality data were obtained from the National Cancer Registry Program Reports and the Cancer Incidence in 5 Continents publications. Further, a comprehensive review of medical literature was done for information on individual cancers as well as survival data. 1.6 to 4.8% of all cancer in India is seen in children below 15 years of age and the overall incidence of 38 to 124 per million children, per year, is lower than that in the developed world. The considerable inter-regional variation in incidence and mortality rates across India suggests a possible deficiency in ascertainment of cases and death notification, particularly in rural areas. The marked male preponderance of Hodgkin's disease, lower incidence of central nervous system tumors, and higher incidence of retinoblastoma merit further analysis.Keywords: Childhood cancer, cancer registry, epidemiology, India, incidence, longitudinal trends, mortality, survival Introduction Thirteen percent of the annual deaths worldwide are cancer-related and 70% of these are in the low- and middle-income countries. [1] In India, the leading causes of cancer-related death are carcinoma of the cervix in women and carcinoma of the lung and lower airways in men. [2] The focus of the National Cancer Control Program of India has been on primary prevention, by promoting tobacco control and genital hygiene; secondary prevention by screening for cervical cancer, breast cancer, and oropharyngeal cancer; and palliative care. [3] Although child health continues to be the priority health issue, childhood cancer is not yet a major area of focus. The emphasis is on reduction in mortality of infants and under-fives, by promotion of breastfeeding, rational antibiotic therapy for acute respiratory infections, oral rehydration for diarrhea, an extensive immunization program, and appropriate prevention and treatment of malaria. [4] Worldwide, the annual number of new cases of childhood cancer exceeds 200,000 and more than 80% of these are from the developing world. [5] Seven out of 10 children with cancer in the resource-rich countries are cured, with a five-year survival for certain cancers, for example, Hodgkin′s disease and retinoblastoma, now 95%. [6],[7] Recent studies have shown that this success in survival can be replicated in the developing world through twinning programs and shared expertise. [8],[9],[10],[11] As we make progress in reducing infection-related childhood deaths in India, it is no longer acceptable to ignore children with cancer, who have an increasing likelihood of cure with appropriate treatment. A fundamental step in caring for these children is to estimate the current burden of childhood cancer in India and to understand how the occurrence and outcome of the disease varies across the country. In this context, this study aims to describe the epidemiology of childhood cancer in India. This will serve as a reference source for clinicians, epidemiologists, researchers, and health administrators. It should also be the stimulus for further research on the etiology of childhood cancer. Methods Information for this review was obtained from multiple sources. Current incidence and mortality rates were derived from the 2006 National Cancer Registry Program (NCRP) reports, from thirteen population-based cancer registries (PBCRs) across India - rural Ahmedabad, Barshi, Bangalore, Bhopal, Chennai, Delhi, Mumbai, and North-East (Aizawl District, Dibrugarh District, Kamrup Urban District, Silchar Town, Imphal West District, Sikkim State). [12],[13] Data from Cancer Incidence in Five Continents Volume V to IX, published by the International Agency for Research in Cancer (IARC) were used to calculate longitudinal incidence trends from 1978 to 2002. [14],[15] Besides this, a comprehensive review of medical literature was done, for information on individual cancers as well as survival data. Burden of Childhood Cancer Cancer is generally regarded as a disease of adults. In England only 0.5% of all cancer cases occur in children less than 15 years of age. In India however, this proportion appears higher at 1.6-4.8% with variation by place of residence [Table - 1]. This is related to the population structure (33% of the population in India is less than 15 years of age compared to 18% in England) and to a lower incidence in India of adult cancers attributed to a western life-style (e.g. carcinoma of the breast, large bowel, lung and prostate). Similarly, the differences in proportion of childhood cancer among different areas in India can also be a result of the underlying population structure but other factors like completeness of cancer registration as well as geographical variation in exposure to risk factors need to be considered. Despite there being a higher proportion of childhood cancer in India relative to the developed world, it has not been a priority in healthcare. This is because of its contribution to overall childhood mortality. Excluding neonatal deaths, infectious and parasitic diseases are the most common cause of death in children in India. Only 2% of all deaths in this age group are reported to be cancer-related deaths. [16] This contrasts with data from England and Wales where injuries are the most common cause of death in children overall (21%) and cancer the most common cause of disease-related death (20%). [17] Incidence of Childhood Cancer Overall incidence: The incidence of childhood cancer in most populations in the world ranges from 75 to 150 per million children per year. [18],[19] However, the reported age of the standardized incidence rate for India ranges from 38 to 124 per million children per year [Table - 1]. The highest incidence is reported from Chennai and the lowest from rural Ahmedabad. This suggests that either there is truly a lesser incidence of childhood cancer in some areas of India, or as is more likely, there is under-ascertainment of cases. The reported incidence in urban areas (Bangalore, Bhopal, Chennai, Delhi, Mumbai) is generally higher than from rural areas (Barshi and Ahmedabad district) and more comparable with the average world incidence. Again, one can speculate that this can wholly or partly be attributed to under-ascertainment of cases and registration in rural areas, but this remains to be confirmed. It is also necessary to investigate if there are factors associated with urban living like overcrowding, air pollution, and so on, which contribute to a relatively higher incidence of childhood cancers in such areas. Variation by sex: Overall cancer in childhood is more common among males than females and the male to female ratio in the most resource-rich countries is around 1.2:1. [7],[20] However, some cancers like retinoblastoma, Wilms′ tumor, osteosarcoma, and germ cell tumor actually show a slight female preponderance. The reported incidence of childhood cancer in India in males (39-150 per million children per year) is higher than in females (23-97 per million children per year) in all PBCRs except in North East India [Table - 1], and this gives a male to female ratio [Table - 2] that is much higher than what is seen in the developed world. As incidence rates automatically adjust for the sex ratio in the underlying population, there have to be other reasons for this relatively higher incidence of childhood cancer in males seen in India. Gender bias in seeking healthcare, including treatment of cancer, is one possible explanation. [5] The male preponderance for most of the individual cancers types in Delhi would suggest this. One has to also consider other possibilities. Even after accounting for gender bias in seeking healthcare and the well-documented male preponderance of Hodgkin′s disease (HD), the observation of a 12-fold higher incidence of HD in male children in Delhi is truly remarkable and novel, and needs to be further investigated. Also new is the observation that the incidence of childhood cancer in females in the North East is higher. It remains to be determined if this is a true difference or a registration artifact (cancer registration in the North East started in 2003). Variation by cancer type: [Table - 3] and [Table - 4] Leukemia is the most common childhood cancer in India with relative proportion varying between 25 and 40%. Sixty to 85% of all leukemias reported are acute lymphoblastic leukemia (ALL). Compared to the developed world, the biology of ALL appears different in India, with a higher proportion of T-Cell ALL (20-50% as compared to 10-20% in the developed world), hypodiploidy and translocations t(1;19), t(9;22), and t(4;11), all of which contribute to a poorer prognosis of this leukemia. [21],[22],[23],[24] It has been proposed that T-Cell ALL predominates in economically disadvantaged areas, but with urbanization, industrialization, and increasing affluence, common ALL, which peaks in incidence between the age of 2 and 5 years, increases. [25] In the developed world, CNS tumors are the second most common childhood cancer (22-25%) and lymphomas a distant third (10%). [7],[20] In contrast, in India lymphomas often exceed CNS tumors, particularly in males. Not only is the proportion of lymphomas higher in India, but HD exceeds non-Hodgkin′s lymphoma (NHL), a pattern opposite to that seen in the developed world. This specifically seems to be a result of the high incidence of HD in male children in India (incidence rate of 8.2-19.6 per million children, per year, in Bangalore, Chennai, Delhi, and Mumbai PBCRs compared to 5.7 in USA and 6.4 in Britain). [7],[20] In contrast, the incidence of HD in females and of NHL in both sexes is not very different from the incidence in the developed world. Besides differences in incidence, the pathobiology of these cancers is also different. Among NHL, the proportion of T-cell lymphoblastic lymphoma and diffuse large B-cell lymphoma is much higher and the proportion of mature B-cell (Burkitt′s and Burkitt-like) lymphoma much lower in India than that seen in the developed world. [26] Similar to T-cell ALL, the higher proportion of T-cell NHL may be linked to lower socioeconomic status. Mixed cellularity is the most common Hodgkin′s disease subtype and is responsible for the incidence peak at a younger age, as seen in India, compared to the peak seen at ages 16 to 30 years in the developed world, where nodular sclerosis is most common. [19] The high proportion of mixed cellularity in India is thought to be related to early childhood Ebstein Barr virus exposure. [27] In the larger urban areas of Bangalore, Chennai, Delhi, and Mumbai, the incidence rate of CNS tumors is 10-20 per million children, per year, which is half of that in the developed world. Interestingly, the incidence of CNS tumors in children in the developed world has increased in the last 30-40 years with increasing availability of CT and MRI scanners. [28] A relative paucity of neurodiagnostic and neurosurgical facilities, which leads to missed diagnosis in those presenting with headache, seizures, and altered sensorium, could explain the differences in incidence in India. Neuroblastoma, which is the second most common solid tumor in childhood after CNS tumors,, is much less frequently reported in India. Retinoblastoma has an incidence rate of three to five per million children, per year, and accounts for 2.5 to 4% of all childhood cancers in most developed countries. Barshi, Chennai, and Delhi report a 2-3 fold higher incidence of tumors of the eye (majority of which will be retinoblastoma in children < 15 years of age), a finding that has also been previously reported. [29],[30] In North East India, while the incidence of tumors of the eye is not high, the proportion is 6 to 10% of all childhood cancer. The hospital-based cancer registry in Dibrugarh as well as case series from hospitals in North East India confirm their high proportion among childhood cancer. [31],[32],[33] Does this suggest that there is an increased occurrence of retinoblastoma in India or is it because of better diagnosis and recognition of retinoblastoma, which once at an advanced stage is easy to identify? In contrast there could possibly be under diagnosis of hematological and CNS neoplasms, which are often present with nonspecific symptoms like fever, anemia, seizures, and altered sensorium, and where diagnosis may depend on the awareness of the physician and availability of diagnostic facilities. Availability of more data from the recently established PBCRs in North East India will help to clarify this issue in the future. Variation is also seen in the incidence of tumors of the kidney (majority of which are Wilms′ tumor in children < 15 years age), with the incidence in Bangalore and Mumbai being half of that seen in Delhi, Chennai, and other developed countries. Incidence Trends of Childhood Cancer The incidence of childhood cancer is increasing by 1.1% every year in Europe, but the rate of change as well as the direction is different for individual cancer types. [34] The incidence of CNS tumors is increasing by 1.7%, lymphomas by 0.9%, and leukemias by 0.6%. On the other hand the incidence of bone tumors, liver tumors, and retinoblastoma is unchanged. [34] Part of these increases can be explained by changes in diagnostic methods and registration practices, but other environmental and lifestyle factors may have a role. In India, the reported incidence of childhood cancer has increased over the last 25 years, but the increase is much larger in females (44-76% increase) than males (12-27% increase) [Figure - 1]. This striking pattern of sex difference is also seen for leukemias where the increase in female children is even higher. The pattern of CNS tumors is very different, with a 55-120% increase seen in both sexes. Lymphomas show the least increase, and have actually declined in incidence in female children in Chennai. Several conclusions can be drawn from these observations and these need to be further investigated. The disproportionately higher increase in incidence of childhood cancer in females could reflect a shift in the attitude of society toward the female child. Improved case ascertainment in females would result in narrowing of the gap between the incidence of childhood cancer between males and females, which exists because of gender bias. The large increase in incidence in leukemia from Bangalore (190% in males and 275% in females) is likely to be a registration artifact as the registry was only established in 1982. If one considers the percentage of change in leukemia from 1983-1987 to 1988-2002 for Bangalore, that is, the last 20 years rather than 25 years, then the percentage increase is 7% for males and 73% for females. The large and consistent percentage increase in incidence of CNS tumors may be from increased exposure to an unidentified risk factor, or reflect an increased availability of neuroimaging and neurosurgery as has been seen in rest of the world. [28] Finally, one needs to differentiate between HD and NHL before drawing any conclusions from the trends in lymphomas. Survival from Childhood Cancer With centralization of treatment and enrollment in clinical trials, tremendous progress has been made in caring for children with cancer in the developed world and a five-year overall survival for all childhood cancers combined, is now 75-79% [Table - 5]. [35],[36] Similar outcomes have been achieved in India in those treated at tertiary institutes like the Tata Memorial Hospital in Mumbai. [38] However, one cannot extrapolate these results to the whole population as often those who abandon treatment or are lost to follow-up are excluded from the analysis of hospital case series, and such patients may have a more advanced disease and a poorer outlook. PBCR survival data is a better representation of cancer outcomes across India and have been reported from Bangalore and Chennai where the five-year overall survival for all childhood cancers combined is 37-40% [Table - 5]. The highest survival in India is seen for Wilms′ tumor and Hodgkins′ disease where approximately two-third of the children survive for five years or more. The survival for retinoblastoma and germ cell tumors, which are cancers with excellent prognosis in the developed world, is however, disappointingly low and may be related to an advanced stage at presentation and suboptimal chemotherapy regimens used. [41],[42] Also low is the prognosis for leukemia and CNS tumors where approximately only 33% and 25% of the children survive at five years. There is no survival data from rural PBCRs, but it is likely to be still lower. Multiple inter-related factors are responsible for the poorer outlook of childhood cancer in India. Limited financial resources, lack of awareness of the meaning of symptoms, and difficulty in accessing healthcare, contribute to advanced stage presentation. Such a delay in presentation, along with unfavorable biology (e.g., as seen in ALL), leads to a need for more intense treatment, resulting in higher treatment-related morbidity and mortality. [5],[38] Treatment refusal or abandonment, besides treatment-related death, is a frequent unwanted outcome. [43] A higher five-year survival seen in those treated at specialist cancer centers and among those who complete their treatment, reinforces the importance of centralization of treatment and compliance. [29] Of late, twinning programs, which foster interactions between public hospitals in developing countries and established cancer treatment centers elsewhere, have been seen to reduce abandonment and improve survival elsewhere in the world. [8],[9],[10],[11] Similar strategies could be applied here. Clinical trials started by the Indian Cooperative Oncology Network (ICON, www.oncologyindia.org) and adoption of the MCP841 protocol for ALL in major Indian centers have been steps in the right direction for improving childhood cancer outcome. [38] Mortality from Childhood Cancer Although cancer is the most common cause of disease-related death in children in the developed world, with improving survival rates, the mortality rate has declined to approximately 30 per million children per year. [7],[20] In India, the mortality rate (adjusted to world standard population) varies from 14 to 34 per million children per year [Table - 6], and on first glance appears similar or even better than the developed world. However, the incidence of childhood cancer in some areas of India as discussed above, is much less than other parts of the world and the mortality:incidence (M:I) ratio rather than the mortality rate gives a more accurate picture of death from childhood cancer. This varies from 17 to 72% in India as compared to 20-24% for USA and Britain, [7],[20] and is particularly high in rural Ahmedabad (61%) and Barshi (72%). Among the major urban areas, the mortality rate as well as M:I ratio in Mumbai is 1.5 to 2 times higher than that of Bangalore, Bhopal, Chennai, and Delhi. The reliability of these statistics depends on the comprehensiveness of death notification and quality of death certification, which are much higher in Mumbai than other areas of India. [44] Therefore, data from Mumbai is probably a truer estimate of mortality in urban India. The largest contributor to mortality from childhood cancer in Britain are CNS tumors, reflecting the relatively poor survival in this group, followed by leukemias and neuroblastomas. In contrast, in India, leukemia continues to be the largest contributor to cancer-related mortality in children followed by lymphomas and CNS tumors, which have similar mortality rates. This pattern is a result of the relatively high incidence of lymphomas, low incidence of CNS tumors, and a lower survival of all cancers, including leukemias in India. Conclusion We have reviewed the epidemiology (incidence, survival, and mortality) of childhood cancer across different PBCRs in India and also compared it with data from the resource-rich countries. This has highlighted certain facts and raised several questions, which need to be answered in future studies. The marked male preponderance of Hodgkin′s disease, lower incidence of CNS tumors, and higher incidence of retinoblastoma merit further analysis. The considerable inter-regional variation in incidence and mortality rates across India suggests a possible deficiency in the ascertainment of cases and death notification, particularly in rural areas. Acknowledgments We would like to acknowledge that the data for much of this review has been taken from National Cancer Registry Program reports published by Indian Council of Medical Research, as well as from Cancer Incidence in Five Continents Volume published by the International Agency for Research in Cancer, all of which are in the public domain. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09068t3.jpg] [cn09068t4.jpg] [cn09068t6.jpg] [cn09068f1.jpg] [cn09068t5.jpg] [cn09068t2.jpg] [cn09068t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}