 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
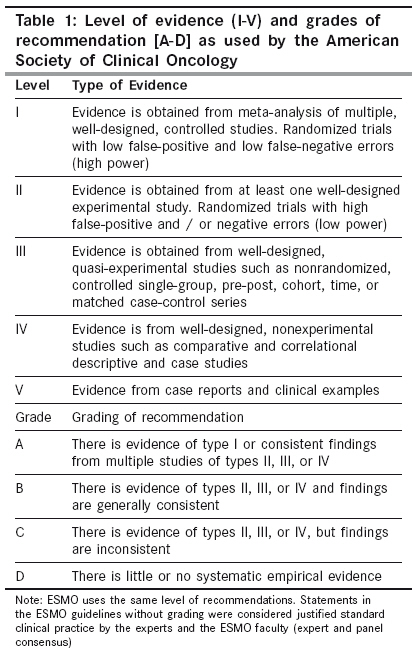
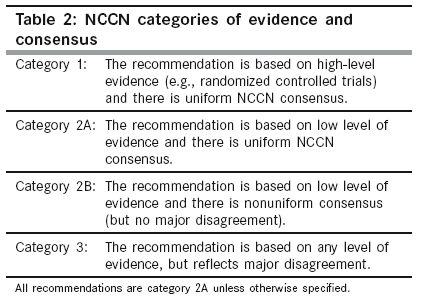
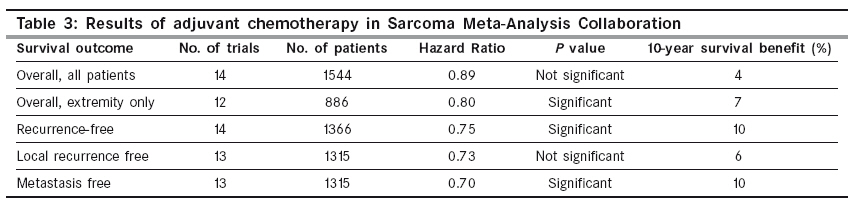
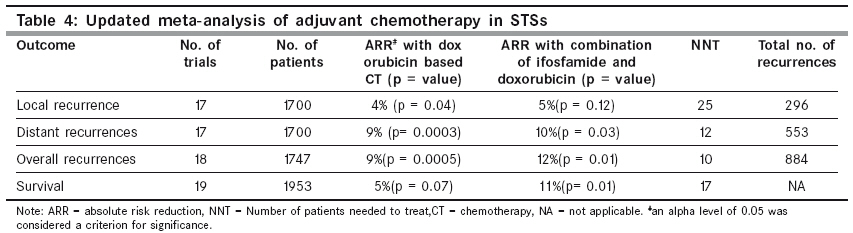
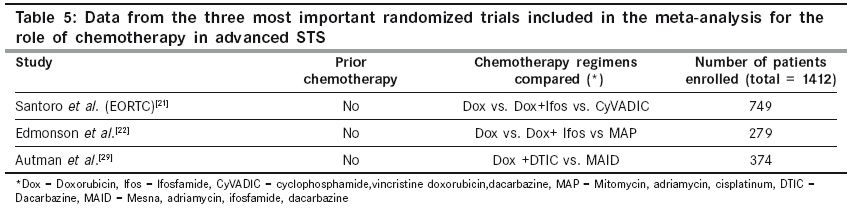
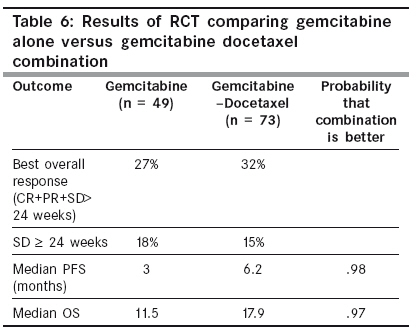
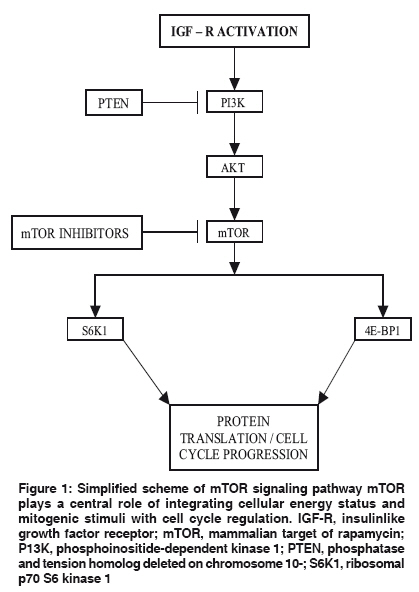
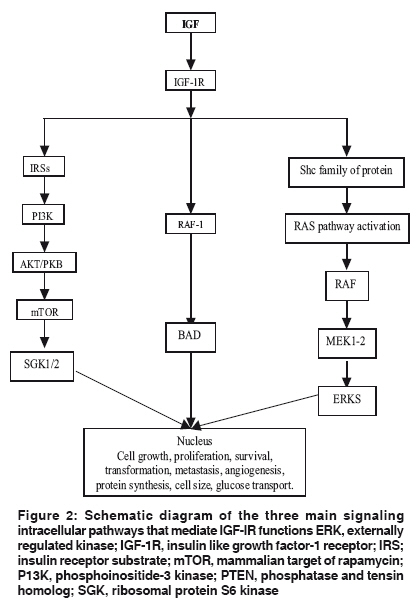
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 274-287 Review Article Chemotherapy in adult soft tissue sarcoma Jain A, Sajeevan KV, Babu KG, Lakshmaiah KC Department of Medical Oncology, Kidwai Memorial Institute of Oncology, Bangalore - 560029 Code Number: cn09087 PMID: 19749457 Abstract Soft tissue sarcomas (STSs) are rare and histologically diverse neoplasms. Recent results of various meta-analyses and development of newer drugs have changed the medical management of soft tissue sarcoma. This review gives an outline of chemotherapy and the newer targeted therapies for the same. We have carried out an extensive search in PubMed, Medline for almost all relevant articles concerning chemotherapy of soft tissue sarcoma. The available data from the literature is mainly composed of the most recent reviews, meta-analyses, phase II, and randomized phase III trials published in various peer reviewed journals and various international conferences. The role of neoadjuvant and adjuvant chemotherapy has been found to be controversial. The recent meta-analysis for adjuvant therapy in STSs has shown an increase in the overall survival with combination of ifosfamide and adriamycin. In locally advanced and metastatic STSs, single agent adriamycin remains the basic standard of medication. The combination of ifosfamide and adriamycin may also be used for rapid symptom relief and in patients planned for curative resection for metastases. Newer combinations of docetaxel and gemcitabine appear promising in selected subgroups, especially in leiomyosarcoma and malignant fibrous histiocytoma. Some recent developments include the European Union's approval of trabectedin for advanced STSs patients who had progressed on adriamycin and ifosfamide therapy. The future of mTOR inhibitors, insulin like growth factor receptor inhibitors and anti-angiogenic drugs appear quite promising. Newer methodologies such as, Bayesian adaptive randomization and inclusion of newer end points like progression-free rate, time of progression rate, and tumor growth rate will improve the results of sarcoma trials. At the end of each section we have also presented recommendations from *European Society of Medical Oncology and **National Comprehensive Cancer Network guidelines v.1.2009 for better correlation with the present literature.Keywords: Chemotherapy, soft tissue sarcoma, neoadjuvant, adjuvant, metastatic STSs, trabectedin, mTOR inhibitors, VEGF inhibitors, IGF inhibitors Introduction Soft tissue sarcomas (STSs) comprise of a group of relatively rare, anatomically and histologically diverse neoplasms. Embryologically these tumors are derived from tissues arising from the mesodermal and ectodermal layer. They account for 1% of adult malignancies and 15% of pediatric malignancies. The incidence of STSs in USA is approximately 8300 new cases annually. These tumors are rare and histologically diverse, which makes it difficult to develop specific therapies for these specific tumor types. [1] We carried forth an extensive literary search in the Pub Med and Medline of almost all relevant articles concerning chemotherapy of soft tissue sarcoma. The available data from the literature is mainly composed of the most recent reviews, meta-analyses, and phase II and randomized phase III trials published in various peer reviewed journals and various international meetings. This review aims to discuss the recent standard chemotherapy management in non GIST (gastrointestinal stromal tumors) STSs and controversies related to neoadjuvant, adjuvant, and palliative chemotherapy in STSs. This review also discusses the newer cytotoxic chemotherapy combinations and targeted therapies that will increase the footholds of the medical oncologist in the management of STSs in the near future. At the end of each section we have also presented recommendations from FNx01(ESMO) [2] [Table - 1] and FNx08(NCCN) [3] [Table - 2] guidelines, in order to be in sync with the present literature. Neoadjuvant Therapy Several methods like neoadjuvant chemotherapy, radiotherapy (RT), chemoradiotherapy, isolated limb perfusion (ILP), and chemotherapy with hyperthermia have been attempted in an effort to get better local control, limb salvage, and survival. With the experience in melanoma, isolated limb perfusion and hyperthermia were attempted in soft tissue sarcoma. Initial studies showed disappointing results, but high dose recombinant human tumor necrosis factor alpha (rhTNFa) started showing encouraging results. [4] In a multicentric trial, isolated limb perfusion with high dose of rhTNF-alpha along with IFN gamma and melphalan had resulted in an overall response rate of 76% with a limb salvage rate of 82%. [5] Following this, several centers in Europe had started using this technique. TNF alpha increases the vascular permeability and eases penetration of the cytotoxic agent specifically on the tumor site. This form of therapy has a potential for severe complications like hypotension and septic shock, rhabdomyolysis, and renal failure, especially if leakage in systemic circulation occurs. This indeed requires a great deal of experience and technical support. Postoperative complications such as edema, blistering, and erythema are common in this regard. No randomized trial data is available comparing TNF alpha ILP followed by surgery with surgery alone, however, this modality has shown a good functional outcome and long-term control rates. [6] Role of Preoperative Radiotherapy The exact role of neoadjuvant radiotherapy in STSs still remains unclear. The advantages are less morbid surgery, less tumor spillage during surgery and less delay in surgery. In the case of extremity sarcoma, a study by O′Sullivan et al . has shown a comparatively better overall survival rate. At 36 months the overall survival rate was 90% in the preoperative group versus 75% in the postoperative group. [7] However in this study preoperative radiotherapy was associated with postoperative wound complication in up to 35-37% of the patients. Moreover, preoperative radiotherapy has not shown any significant statistical survival benefits in other studies. [8] Chemoradiotherapy Chemotherapy with radio sensitizing dosage along with an optimum systemic cytotoxic dose and radiation was carried out in many studies. Doxorubicin at a dose of 12 mg/m 2 per day along with EBRT (150 - 200 cGy/day) was used in a study by Toma et al . [9] The partial response rate was 56%, with 11% complete response. Subsequent studies started using doses up to 20 mg/m 2 /week and fortunately good surgical clearance was reported. [10] Major wound complications were seen in only 23% subjects. Combination chemotherapy with MAID protocol (doxorubicin, ifosfamide, mesna, and dacarbazine) and EBRT 44Gy favored superior disease-free survival, freedom from metastasis, and overall survival compared to historical controls. The alarmingly high rate of wound complications (58%) was a major concern. [11] Another trial by the European Organization for Research and Treatment of Cancer (EORTC) with MAID protocol and External Beam Radiation Therapy (EBRT) showed better surgical clearance and a high rate of toxicity precludes its use outside the clinical trial. [12] Neoadjuvant Chemotherapy Randomized trials exploring the utility of neoadjuvant chemotherapy in STSs are limited. In the EORTC study, high risk STS received preoperative doxorubicin 50mg/m 2 and ifosfamide 5gm/m 2 on a three weekly basis.At the median of a follow-up of 7.3 years, the 5 year disease-free survival rate and overall survival rate were not significant (52 versus 56% and 64versus 65%). [13] The use of neoadjuvant chemotherapy with hyperthermia was addressed in a randomized trial by EORTC. The chemotherapy consisted of etoposide, ifosfamide, and doxorubicin. The eligible patients had more than 5 cm sized tumors, grade 2 - 3, deep with extra compartmental and recurrent sarcoma. The overall response rate for chemotherapy with hyperthermia group was 28.7% versus 12.6% for chemotherapy only arm. Median local progression-free survival was 45.3% in the chemohyperthermic arm versus 23.7% in the chemotherapy-alone arm. Further studies are required to validate these findings. [14] There is an evolving role of neoadjuvant chemotherapy in STSs, and the only strategy that has shown survival is combination chemotherapy with regional hyperthermia (also mentioned in the ESMO recommendation). The NCCN guidelines have assigned category 2A recommendation for preoperative RT for sarcomas with acceptable functional outcome and category 2B recommendation for both preoperative CT and preoperative chemoradiation. Adjuvant Chemotherapy and STSs The role of adjuvant chemotherapy for the treatment of STS is controversial. After adequate local treatment for STS, 50% of the patients invariably relapse with local or distant disease (lungs with extremity sarcoma or liver in abdominal primary). It was found that 45% die of sarcoma within five years. [15] Anthracyclines are the most active agents in sarcoma therapy in metastatic settings, so they were universally employed in adjuvant trials, either alone or in combination. However most of these trials were too small to detect moderate treatment effects reliably. The statistical technique of meta-analysis may overcome the problem of the inadequate power of small randomized controlled trials (RCTs), and meta-analyses based on individual patient data (IPDMA) can minimize other potential biases (e.g., exclusion of unpublished trials, variable follow-up, post randomization exclusions, and differing definitions of end point) that are inherent in the analyses that are limited to published results. Until recently the results of the Sarcoma Meta-Analysis Collaboration (SMAC), published in 1997, in the Lancet journal, provided the maximum insight for the role of adjuvant chemotherapy in patients with STSs. [16] This landmark publication analyzed 14 studies and examined the IPDMA of 1568 patients comparing adjuvant doxorubicin chemotherapy versus no chemotherapy in localized STSs. The results of this meta-analysis provided evidence that adjuvant doxorubicin chemotherapy significantly improved the time of local recurrence and distant metastases in addition to recurrence-free survival. There was a trend toward improvement in the overall survival, with a survival advantage of 4% (P = ns). In a subset analysis of extreme sarcoma (n = 886), there was a 7% benefit ( P = 0.029) [Table - 3]. However, the results of the subgroup analyses should be interpreted with caution because subgroup analyses are currently not recommended in meta-analyses unless it is a part of the original study design for all the studies included. In the recent updates of this meta-analysis Pervaiz et al . analyzed 18 trials with a cohort of 1953 patients. [17] This meta-analysis included four additional studies, in addition to 14 studies taken in the earlier meta-analysis. These four additional studies used the ifosfamide and adriamycin combination therapy as one of the arms. These four studies were selected from 93 abstracts retrieved after screening 31,039 potentially relevant articles. A new parameter for NNT (number of patients needed to treat) was calculated for each outcome, to estimate the number of patients that would need to receive treatment, before reducing the risk in one. This update showed that a combination of ifosfamide and adriamycin resulted in risk reduction of death from 41 to 30%.The authors conclude that there is marginal efficacy of chemotherapy in localized resectable soft tissue sarcoma, with respect to local recurrence, distant recurrence, and overall survival. These benefits are further improved by the addition of ifosfamide to doxorubicin regimen [Table - 4]. Although the risk reductions are significant, these must be weighed against associated toxicities like grade III / IV myelosuppression and cardiotoxicity. Sometimes tumor heterogeneity is a major concern in meta-analysis, but none of the endpoints found significant heterogeneity in this trial. To maintain the consistency of results no subgroup analysis was conducted in this study, as individual data points from the studies were missing. The results of this meta-analysis are encouraging and will generate more confidence in discussing the pros and cons of adjuvant chemotherapy with individual patients. This meta-analysis has not included the data of the EORTC adjuvant trial, which is one of the largest adjuvant trials (published in abstract form only). The interim analysis of this study, published in ASCO 2007, has thus far failed to show a survival advantage for adjuvant chemotherapy in STSs. This trial included 351 patients who received adriamycin and ifosfamide combination therapy, but the overall survival was better in the control arm than in the chemotherapy arm (69 vs. 64%). According to the authors the results of the previous adjuvant chemotherapy trials in STS were better because of better surgery and postoperative radiotherapy, with no role of chemotherapy. [18] The biggest set back for the role of adjuvant chemotherapy in STSs comes from the pooled analysis of the two STBSG-EORTC (Soft Tissue and Bone Sarcoma Group- EORTC) phase III clinical trials presented in ASCO 2008. A total of 819 patients were included, with a median follow up of 8.2 years. Large tumor size, high histological grade, and R1 resection are independent prognostic factors for both progression-free survival (PFS) and overall survival (OS). Tumor size, histological subtype, and grade were not associated with any PFS or OS benefit for adriamycin chemotherapy (adCT). Patients with R1 resection had a significantly better PFS and OS in the adCT arm. This study confirms the previously documented prognostic factors in completely resected STS. adCT is not associated with a better outcome in young patients or pathological subgroups. Quality of initial surgery is the most important prognostic and predictive factor for PFS and OS. [19] In recent times, a meta-analysis presented at ASCO 2008, which included the data of the EORTC 62931 trial with a total number of 2170 patients, has shown significant benefit of doxorubicin adjuvant chemotherapy in terms of a five-year DFS and OS. [20] The detailed analysis of the last four studies in the form of peer reviewed literature is eagerly awaited. In conclusion outside a clinical trial, adjuvant chemotherapy in the care of STS needs to be discussed with the patients on an individual basis. The small potential benefit of adjuvant chemotherapy is worth attempting with concerns related to short-term and long-term toxicities of treatment. The latest updated meta-analysis is one more positive step toward increasing the role of adjuvant chemotherapy in STSs. Surprisingly, there are very few proponents of adjuvant chemotherapy in spite of the recent meta-analysis showing encouraging data for the same. The ESMO clinical recommendations have proposed adjuvant chemotherapy only in high-risk individual patients (having G2-G3, deep, > 5 cm tumor). Till the time this writing came up, NCCN version 1 for the year 2009 has assigned Category 2B recommendation for adjuvant chemotherapy and they have not included the recent meta-analysis by Pervaiz et al . Advanced or Metastatic STSs Even after good local control, about 50% patients of non-GIST (gastrointestinal stromal tumor) STSs develop locally advanced or metastatic disease. These patients have a median survival time of 8 to12 months, except for the metastatic alveolar soft part sarcoma, which may persist for years. Lung is the most common site of metastasis from primaries of the extremity or trunk. Most common tumors to develop pulmonary metastases are malignant fibrous histiocytoma (MFH), synovial sarcoma, and leiomyosarcoma. Almost 80% of the patients develop metastasis in the first two years of diagnosis. Myxoid liposarcoma is an exception because areas containing fat (the pelvis, retroperitoneum, soft tissue, and bone marrow) are the most common sites for metastases. Patients who can undergo resection of pulmonary metastases have the best chance of survival with some series reporting five-year survival rates of 20 - 30%. [1],[15] Chemotherapy Chemotherapy is the main stay of treatment for patients with locally advanced inoperable or metastatic disease. Agents like doxorubicin, ifosfamide, and dacarbazine are commonly used. Single Agents Doxorubicin This drug is the backbone of any combination regimen used for STS. The single agent response rates (RR) are in the range of 20 to 30% with median survival in the range of 7.7 -12 months. [21] This response rate was 11% in one of the studies, in which the outside review of imaging studies was performed. [22] Doxorubicin has a dose response relationship so RR increases with higher doses. The best response rates are seen with dosages in the range of 75 mg/m 2 to 90 mg/m 2 . Epirubicin is a less cardiotoxic analog of doxorubicin, which failed to demonstrate any benefit as compared to doxorubicin. [23] Pegylated liposomal doxorubicin can be used in patients where doxorubicin is contraindicated, but the response rates of this drug as a single agent are lower than the conventional doxorubicin. [24] The use of doxorubicin is mainly limited by myelosuppression and cardiotoxicity. Ifosfamide Besides doxorubicin, ifosfamide is the only drug that consistently shows activity against advanced soft tissue sarcoma, with similar outcomes. This drug also has a dose- response relationship and higher doses can be used as it lacks cardiotoxicity. In an extensive study of the main active and toxic ifosfamide metabolites, it has been seen that continuous infusion and short infusion schedules, using ifosfamide as a monotherapy with an identical dose (9 gm/m 2 ), given over three days, by either continuous infusion or three-hour infusions daily, were equivalent in terms of pharmacokinetic endpoints, such as areas under the concentration time curve. [25] Recently, the first study to directly compare doxorubicin with ifosfamide in a phase III trial was published, comparing two schedules of ifosfamide (9 gm/m 2 over three days by continuous infusion (CI) or 3 gm/m 2 per day in three hours over three days) with standard-dose doxorubicin(75 mg/m 2 ) every 21 days in advanced or metastatic STS. Although toxicities were more in both the ifosfamide arms, no differences in progression-free survival (PFS), RR, or OS were seen among the three treatment arms. [26] In an excellent review by Tascilar et al , the authors concluded that ifosfamide is likely to exhibit antitumor activity that is equivalent to that of doxorubicin. Doses of approximately 9-11 g/m 2 every 21 days are recommended, with no clear preference for CI or infusion, in three to four hours. There is no data suggesting that higher doses yield greater anti-tumor response, which is likely a result of the saturated conversion of ifosfamide into active metabolites at doses > 12 gm/m 2 . [27] Dacarbazine Dacarbazine has been used most extensively, either as a first line agent in combination with doxorubicin and ifosfamide (MAID) or as a second line salvage treatment. It is commonly given in divided doses over three to five days, but it can be given as a short infusion of 1.2 gm/m 2 over 20 minutes with the availability of effective antiemetics. Temozolamide, the oral equivalent of dacarbazine, appears to have the same activity against leiomyosarcoma as well. Combination Chemotherapy There are number of phase II trials where combination chemotherapy has been tried for the management of STS. Most studies have tried doxorubicin in combination with alkylating agents (cyclophosphamide or ifosfamide). The most recent meta-analysis for the role of combination chemotherapy in advanced STS has generated important information. This meta-analysis included three phase III trials and 23 single-arm phase II trials. [28] However, phase II trials were not included for the final conclusion. One year was selected as the time point to pool the mortality data, because the expected median survival of patients with inoperable locally advanced or metastatic STS was 9 - 12 months. Meta-analysis of the three most important phase III trials demonstrated that the addition of ifosfamide to a chemotherapy regimen significantly improved the tumor response rate (RR, 1.52, p = 0.009), but did not produce a significant difference in one-year survival (RR, 0.98, p = 0.76). There was no significant heterogeneity among the three trials (χ2 , 2.57; p = 0.28). The authors critically analyzed one-year survival across the three RCTs and found that the median survival ranged between 8.4 and 13 months. Therefore, survival at one year may represent an appropriate clinical bench mark [Table - 5]. All three RCTs reported higher rates of adverse events in the ifosfamide containing regimens. In the two trials, the reported grade 3/4 adverse events were much higher in the ifosfamide arm. The same trials reported greater rates of grade 3/4 myelosuppression in the ifosfamide arm, with one reporting a statistically significant difference. In addition, Edmonson et al . [22] and Antman et al . [29] reported a higher number of toxic deaths in the ifosfamide-containing arm. Finally the authors concluded that the addition of ifosfamide may improve the response, but this does not translate into survival benefit. The evidence also indicates that addition of ifosfamide significantly adds to the toxicity. Consequently the routine use of combination therapy with ifosfamide and adriamycin is not recommended in patients with inoperable, locally advanced, or metastatic STSs. However, patients with severely symptomatic disease or patients eligible for palliative resection can be treated with combination therapy to get better response rates. If critically analyzed the range of ifosfamide used in this meta-analysis is from 3.7 gm/m 2 to 7.5 gm/m 2 , which is less than the dose where higher response rates and PFS can be achieved. With this question in mind EORTC has initiated a phase III trial, with patients randomized to either single agent doxorubicin (75 mg/m 2 ) or doxorubicin (75 mg/m 2 ) and ifosfamide (10 gm/m 2 per cycle). The results of this study are eagerly awaited. Now the question arises as to why combination therapy is not yielding better PFS and OS? There can be many reasons for this, in addition to lower doses of ifosfamide used. These trials were conducted before the recognition of GIST as a separate histological type and many patients with a diagnosis of metastatic leiomyosarcoma, who were actually GIST, were included in RCTs of combination therapy, therefore diluting the results of the final data. Secondly phase III trials are considered more representative of the general population, but there can be a selection bias from the investigator′s side and younger patients are treated off trial and patients who are less likely to be benefited from chemotherapy are recruited in the clinical trial. [1] Is there any role of high dose therapy with granulocyte colony stimulating factor (G-CSF) support or stem cell rescue? The use of hematopoietic growth factors has allowed the study of higher doses of chemotherapy in sarcoma. However, with escalated doses (25% increase) in the MAID regimen there appears to be no significant response rate despite the use of growth factors. [30] The next logical step is to proceed to high-dose chemotherapy with stem cell rescue. Recently in the practice guideline series by Verma et al , [31] the authors analyzed two phase III RCTs, twelve phase II trials, and five phase I dose escalation studies of intensive chemotherapy with G-CSF or stem cell transplant. In the final recommendation they have stated that dose--intensive chemotherapy with G-CSF support and high-dose chemotherapy with stem cell rescue is not recommended in first line treatment of patients with inoperable locally advanced or metastatic STSs. Eligible patients should be encouraged to enter clinical trials assessing novel approaches or compounds. The qualifying statement of the same review suggests that such regimens are more toxic and cause more toxic deaths. Combination Regimens beyond Ifosfamide and Adriamycin As it is proven beyond doubt that combination therapy with Ifosfamide and adriamycin has limited efficacy in terms of RR and OS, newer drugs and other combination therapies are always needed. The regimen which has gone ahead among all newer combinations of cytotoxics is a combination of gemcitabine and docetaxel. Gemcitabine and docetaxel has limited efficacy as a single agent with response rates as low as 3 to 5%. There is a study from the M.D Anderson Cancer Center in which an RR of 18% was achieved with the timed delivery of single agent gemcitabine. In this study the authors concluded that gemcitabine could not be activated faster than 10 mg/m 2 /min and the remainder of a more rapidly administered dose was simply excreted, unchanged, in urine. [32] Hensley and colleagues used this timed infusion of gemcitabine with docetaxel and showed a response rate of 53% in leiomyosarcoma, almost exclusive of uterine origin. [33] When the results of this study were published so many questions were raised, as to, whether the increased response rates were due to the addition of docetaxel or timed infusion of gemcitabine or due to a large number of patients with uterine leiomyosarcoma, which were as such more chemoresponsive tumors. To answer this question SARC (the Sarcoma Alliance for Research through Collaboration) carried out an RCT comparing equivalent myelosuppressive doses of timed infusion gemcitabine versus the combination of gemcitabine and docetaxel. The study employed the Bayesian adoptive randomization design (see below) to produce an imbalance in the randomization, in favor of the superior treatment. The primary end point of the study was tumor response, defined as a complete or partial response, or stable disease lasting at least 24 weeks. The results were initially published in ASCO 2006. The result was superior for combination arm in terms of RR, PFS, and OS. [Table - 6] The final results were published as a phase II trial because the reviewing statistician did not consider it a large enough study to be considered as a phase III trial (personnel communication with Dr. Maki). [34] The maximum benefit was seen in Leiomyosarcoma (LMS) and malignant fibrous histiocytoma / high grade undifferentiated pleomorphic sarcoma (MFH/HGUPS).Toxicities like thrombocytopenia (38%), grade three fatigue and / or grade 3 myalgia (25 vs. 10%) were more common in the combination arm. Trabectedin (Ecteinascidin-743, ET743, Yondelis) This tetrahydroisoquinsoline molecule was derived originally from a tunicate, or ′sea squirt′, Ecteinascidia turbinate (found in the Carribbean and Mediterranean waters), but the current supply is based on a semisynthetic process. [35] It binds to the minor groove of the DNA and forms covalent bonds at the N2 position of guanine. Anti-tumor effects of trabectedin are believed to result from this interference of the binding of other proteins to DNA, in particular transcription factors and DNA-repair proteins. An efficient TC-NER system is crucial to the ET743 antitumor activity. At a cellular level, ET743 slows progression of cells through the S phase. G2-M arrest occurs, resulting in p53 independent apoptosis. [36],[37],[38] A pooled analysis of 183 patients from the three single arm phase II studies, which used doses of 1.5 mg/m 2 administered as a 24-hour infusion once every three weeks, showed some encouraging results. In this analysis though the ORR was only 7.7%, the rate of tumor control (i.e., ORR plus minor responses plus disease stabilization) was 51%. Median overall survival was 10.3 months, and 48% of the patients were alive at one year. [39] A large multicentric randomized phase II study compared weekly and three weekly regimens of trabectedin in liposarcoma and LMS patients whose disease had proved refractory to both anthracyclines and ifosfamide. The median survival was better in once in three weeks regimen (13.8 months vs. 11.8 months) with more neutropenia and tranaminitis. [40] This drug is more active in certain subgroups notably LMS and myxoid / round cell liposarcomas. This drug is extensively metabolized in the liver by CYT3A4 and liver impairment requires dose adjustment. The most important dose limiting toxicities are severe myelosuppression and hepatic dysfunction. Corticosteroid prophylaxis prevents hepatic dysfunction and myelosuppression even if administered just 30 minutes prior to infusion at a dose of 20 mg. It does not cause cardiotoxicity, neurotoxicity, and rarely causes alopecia. [36],[37],[38] There is evidence that STS patients expressing a high level of particular DNA nucleotide excision repair markers (ERCC1 and XPD) and low levels of BRCA1 (a measure of capacity for repairing the double stranded DNA breaks) are highly sensitive to trabectedin. The reverse is true for patients with low levels of ERCC1 and XPD and high levels of BRCA1. [38] In July 2007, the European Union approved this drug for patients with advanced STS after failure of adriamycin and ifosfamide. It also has an orphan drug status in STS in the USA and in ovarian cancer in USA and Europe. [37],[41] The recommended dose is 1.5 mg/m 2 administered over 24 hours thrice weekly, with dexamethasone premedication. The recommendations for metastatic disease are more authentic with anthracyclines as category 1 recommendation in both NCCN and ESMO guidelines. In fact ESMO clinical recommendations have considered multiagent chemotherapy with doxorubicin plus ifosfamide as the treatment of choice when the tumor response is felt to be an advantage and performance status is good. Gemcitabine and docetaxel can be used as second line chemotherapy options and are mentioned in both ESMO and NCCN guidelines. Trabectadin is a second line option in Europe for both leiomyosarcoma and liposarcoma. In USA there are ongoing trials with trabectadin, and therefore, it is not included in the recommendations. ESMO also recommends taxanes as an alternative option for angiosarcoma. Investigational New Drugs Mammalian target of rapamycin (mTOR) inhibitors Other than trabectedin, mTOR inhibitors are the drugs that have gone farthest in the drug development strategies of STSs. ′mTOR′ is a cytoplasmic serine / threonine protein kinase involved in key cell cycle signaling. It lies at the interface of two major signaling pathways, one initiated by PI3K and the other energy-sensing pathway through the serine threonine kinase 11(LKB1). Growth factor like insulin (IGF) primarily regulates the mTOR pathway signaling through the PI3K/Akt pathway. The downstream targets of mTOR, S6K1 (ribosomal kinase), and 4E-BP1 (translational initiation factor) ultimately lead to protein translation when phosphorylated. Inhibition of mTOR affects the downstream messengers S6K1 and 4E-BP1, preventing translation of mRNA involved in G1 to S cell cycle progression. This will lead to impaired cyclin dependent-kinase (CDK) activation, inhibition of RB phosphorylation and renders the cell in G1 arrest [42],[43] [Figure - 1]. Abnormalities in mTOR signaling have been implicated in GIST, leiomyosarcoma, and rhabdomyosarcoma. [44] Mutations of upstream pathways of mTOR-like activation of insulin-like growth factor receptor (IGF-1R) or deletion of phosphatase and tensin homolog deleted on chromosome 10 (PTEN) leads to development of cancer. [43],[45] PTEN mutations are especially involved in LMS. Rapamycin (sirolimus) is a macrolide antibiotic isolated from a strain of strepotomyces hygroscopicus and is first to show mTOR inhibitory activity. Initially it was discovered as an antifungal agent and got FDA approval as an immunosuppressant in renal transplant patients in 1990. The National Cancer Institute discovered its anticancer activity. Recent studies have demonstrated that rapamycins have antiangiogenic effects by inhibition of hypoxia inducible factor (HIF-1α) translation as well as by intercepting VEGF / VEGFR. [46] mTOR inhibitors in clinical development Three rapamycin analogs, CCI-779 (temsirolimus), RAD001 (everolimus), and AP23573 (deforolimus) have been developed to improve the solubility of drugs and are currently in the clinical developmental stage. Interim results of deforolimus therapy in a phase II trial of patients with advanced soft tissue and bone sarcoma are encouraging, with 24% patients experiencing a response of clinical benefit (defined as complete or partial response or stable disease for at least 16 weeks using RECIST), but the objective response rate was as low as 2.6%. [47] These drugs have a high therapeutic index with mucositis, skin rash, and elevated hepatic transaminase as main toxicities. The FDG-PET scan can be used as an early pharmacodynamic marker to monitor patient response to mTOR inhibitors. These drugs are also active in other tumors and temsirolimus is recently approved for renal cell carcinoma. Insulin like growth factor 1 receptor (IGF-IR) inhibitors The insulin like growth factor (IGF) system is composed of multiple receptors and ligands. There are three ligands (IGF-1, IGF-II, and insulin), four receptors, and at least six high affinity binding proteins and binding proteases. IGF-1R is the most important receptor and it is a membrane tyrosine kinase receptor, with an intracellular domain devoted to the initiation of signal transduction cascades responsible for cell growth and proliferation. Activated IGF-1R recruits and phosphorylates adaptor proteins belonging to the insulin receptor substrate (IRS) family or Shc, which leads to the activation of PI3K and MAPK pathways [48] [Figure - 2]. Normally these pathways are very important for growth and development and contribute to about 50% of basal bone cell proliferation. The IGF-1R is the most commonly activated pathway in a variety of sarcomas. The molecular functions that contribute to changes in insulin like growth factor-1 receptor are the overexpression of IGF-1R, overexpression of ligands, reduced expression of IGFBP-3 (insulin like growth factor binding protein), overexpression or constitutive expression of downstream IGF-1R effectors, and loss of PTEN. Types of soft tissue sarcomas with abnormal IGF pathway:
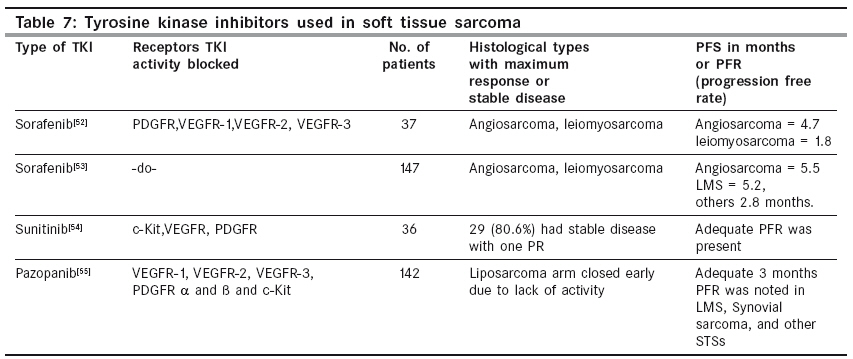
There is definite evidence that inhibition of the IGF-1R pathway enhances the chemosensitivity and radiosensitivity in Ewing′s sarcoma. In the seminal observation by Wan et al , in vitro blocking of the IGF-1R receptor with antibodies blocked the feedback activation of the AKT pathway by rapamycin in the rhabdomyosarcoma cell lines. This observation forms the scientific basis for the future combination therapies of mTOR inhibitors and IGF-1R blocking therapies. The development of resistance to these pathways is slow and limited. In various studies there was no increase in the multidrug resistance protein on prolonged treatment with drugs inhibiting the IGF-1R pathway. Therefore, a combination of these drugs with conventional chemotherapeutic agents will delay resistance to agents like doxorubicin and ifosfamide. The two most common strategies to block IGF-IR are the use of monoclonal antibodies (mAbs) and small kinase inhibitors. Several humanized anti IGF-IR mAbs are under various phases of clinical development and they work by their ability to deregulate the IGF-IR receptor. Transketolase inhibitors are small molecules that modulate the activity of IGF-IR kinase activity. The main toxicities of concern can be hyperglycemia and CNS toxicity. Angiogenesis and STSs Angiogenesis plays an important role in the growth and dissemination of STSs. Among all the proangiogenic factor pathways, the VEGF / VEGFR pathway plays the most important role. High VEGF expression is an independent poor prognostic factor for increased risk of metastases and decreased overall survival. Strong VEGF expression was seen in tumors with epithelioid features, such as epithelioid sarcoma and alveolar soft part sarcomas. [49] High VEGF expression levels have also been described in patients with MFH, dermatofibrosarcoma protuberans, and LMS. [50] High VEGF expression is not only found in tumor tissues but also in blood. The expression of VEGF, PDGF-B, MMP-2, MMP-9 (matrix metalloproteinase), and uPA (uroplasminogen activator) is associated with high tumor grade and usually with short metastasis-free survival in various STSs. The highest level of bFGF is seen in fibrosarcoma and leiomyosarcoma. The data for VEGF is more consistent than that for VEGFR, with one study showing 65% angiosarcoma cases showing VEGFR overexpression. The VEGF / VEGFR pathway is activated in STSs because of various chromosomal translocations, which results in novel fusion proteins and these fusion proteins act as transcription factors for promoters of the VEGF gene. The hypoxia inductible factor (HIF)-1α also acts as an activator for the VEGF gene. [51] STSs with VEGF expression show resistance to various chemotherapeutic agents like doxorubicin. There are several mechanisms explained for VEGF-induced chemotherapy resistance like VEGF-induced increased expression of BcL-2 and survivin antiapoptotic factors. Tumor vessels are also more leaky because of increased VEGF expression, which increases the interstitial tumor pressure and thus prevents drug penetration into the tumor. [51] Roughly there are two drug classes by which the VEGF / VEGFR pathway can be inhibited. These are monoclonal antibodies and tyrosine kinase inhibitors (TKIs). With respect to TKIs, three drugs have been assessed for the effects against STSs [Table - 7]. [52],[53],[54],[55] It is increasingly being recognized that the anti-tumor activity of VEGFR TKIs is not adequately reflected in objective response rates, but is better described in terms of PFS. The concept of better PFS and poor RR has been adequately proven in tumors like GIST, hepatocellular carcinoma, and renal cell carcinoma. Van Glabbeke et al. explored data on 1154 patients of the EORTC-STBSG group, to estimate a new parameter called progression free rate (PFR). [56] According to this study, agents induce a three-month PFR> 40%, which warrants further investigation. Hence, if the PFR is applied to both studies of sorafenib, it seems to exhibit effective anti-tumor activity. In both the studies of sorafenib,> 50% of the angiosarcoma patients were progression-free for three months. For pazopanib, a world wide placebo-controlled randomized phase III study in non-GIST STS, other than Liposarcomas, start accrual shortly. VEGF targeting agents and conventional cytotoxic agents can be combined because of nonoverlapping toxicities. In a single arm phase II study of 37 patients with doxorubicin and bevacizumab 11 patients had stable disease for > 12 weeks, which suggests that this combination has anti-tumor activity. This combination is not tested further because of increased cardiotoxicity even at doses of > 300 mg/m 2 of doxorubicin, with concurrent use of dexrazoxane. [57] Ifosfamide can be an effective alternative for doxorubicin in such trials. Therefore the above-mentioned studies suggest that tumors of vascular origin (angiosarcoma and solitary fibrous tumor), leiomyosarcoma, and synovial sarcoma have shown more response rates with anti-angiogenic drugs, with respect to no activity in the liposarcoma. Most of the above studies with sorafenib, sunitinib, and pazopanib are published in abstract form with limited information, so extrapolating this data to the general population will take a couple of years with the availability of more mature data from these studies and ongoing randomized trials. The same is also applicable for mTOR inhibitors, IGF-1R inhibitors, and newer chemotherapeutic agents. Other cytoxoic agents and targeted therapies in various phases of clinical development are epothilone B derivatives, Trofosfamide, DNA topoisomerase I inhibitors (irinotecan, topotecan, rubitecan), Pemetrexed, Bortezomib, Becatecarin, Biricodar, Exatecan, Soblitodin, Bendamustine hydrochloride, Matrix metalloproteinase inhibitors, Perifosine, EGFR inhibitors, Heat shock protein (HSP) inhibitors, and so on. [58] Newer endpoints and design of clinical trials in STSs: Survival is the ultimate and definite end point for evaluating the efficacy of an oncology drug. However, it takes a long time to mature, and is confounded by subsequent therapies. Therefore, progression-free survival is a better end point to directly measure the benefit from a treatment and it is not confounded by subsequent movements. The newer end points in sarcoma trials are PFR, time to progression ratio, tumor growth rate, progression arrest ratio, and symptom palliation. [59] Bayesian adaptive randomization designs are used in the latest trials of STSs, in which data can be fed back quickly into a randomization model, in real time, to treat potentially fewer patients with inferior therapy in comparison to standard clinical trial designs. [34] Synovial Sarcoma Synovial Sarcoma requires a separate discussion because of its unique molecular biology and high response to chemotherapy. Synovial Sarcoma has consistently demonstrated higher response rates to a combination of doxorubicin- and ifosfamide-based regimens, to the tune of 58%. In virtually all cases (> 90%), synovial sarcomas contain a characteristic translocation between chromosomes X and 18. This translocation, t(X;18) (p11.2;q11.2) involves the SYT gene on chromosome 18 and one of several highly homologous genes (SSX1, SSX2, and SSX4) on the X chromosome. Approximately two-thirds of the cases have a SYT / SSX1 fusion and one-third have a SYT / SSX2 fusion, with only very rare cases reporting a fusion between SYT and SSX4. [60] This fusion protein lacks a DNA binding domain and probably acts as a transcription factor in the regulation of chromosomal remodeling. Antisense oligonucleotides against this protein result in the decreased expression of DNA repair gene XRCC4 and cyclin D1. [61] This fusion protein is a potential target for newer targeted therapies like the SYT-SSX derived junction peptide vaccine. [62] BcL-2 is overexpressed in 79 to 94% of synovial sarcoma, but is rarely expressed in other STS. It is a potential target for Olimerson Sodium, which is an 18 base phosphorothiated antisense oligonucleotide, complementary to six codons of the open reading frame of BcL-2. Members of the EGFR families are clustered with SSX genes in a cDNA cluster analysis. Gefitinib and Transtuzmab are under various phases of clinical development in synovial sarcoma. [61] Summary Soft tissue sarcomas are among the most frustrating neoplasms as far as medical management is concerned. The data for neoadjuvant chemotherapy is robust if regional hyperthermia is added to the combination of etoposide, ifosfamide, and adriamycin. This data needs further confirmation in randomized studies. Even with more data in the future, the scarcity of centers with adequate facilities for hyperthermia will remain a concern for both the developed world and third world countries. Appropriate patients with resectable or unresectable soft tissue sarcoma can get the benefit of preoperative radiation or chemoradiation, to improve the resectability and functional outcome, if thoroughly discussed in the tumor board. These modalities are associated with complications like postoperative delayed wound healing and neutropenia. Adjuvant chemotherapy with single agent adriamycin should be considered if high-risk prognostic features are present, with precautions for complications like cardiotoxicity. All patients showing metastatic STSs or developing metastatic disease after a treatment-free interval will require a multidisciplinary discussion and chemotherapy with a single agent adriamycin or combination therapy of ifosfamide and adriamycin. A subset of patients with good performance status and no comorbidities can achieve long-term survival with the religious use of surgery and chemotherapy. Participation in clinical trials of newer targeted therapies like mTOR inhibitors, IGF-1R blockers, and VEGF inhibitors should be encouraged. The data for these newer drugs appear promising, but most of the studies are in their preliminary stage or published in abstract form. The Medical Oncologists should meticulously analyze the never-ending flow of new data in terms of benefits and cost, before applying it to patients outside a clinical trial. The best care for soft tissue sarcoma requires a multidisciplinary approach with equal involvement of all specialties. The future lies in genomic and proteomic studies because of the vast heterogeneity of soft tissue sarcoma. Acknowledgments Medical writing support provided by Dr. Prakriti Jain and Roche Pharmaceuticals for providing some important journal articles on soft tissue sarcoma. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09069f2.jpg] [cn09069t3.jpg] [cn09069t5.jpg] [cn09069t1.jpg] [cn09069t7.jpg] [cn09069f1.jpg] [cn09069t2.jpg] [cn09069t6.jpg] [cn09069t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}